
Translation, Cultural Adaptation and Validation of the Nurses Self-Concept Instrument (NSCI) to Spanish

 , , , and
, , , and
Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Study Design and Participants
2.2. Participants
2.3. Procedure
2.3.1. Phase 1: Translation and Cross-Cultural Adaptation of the NSCI
2.3.2. Phase 2: Validation of the NSCI in Graduated Nurses
2.4. Data Analysis
2.5. Ethical Concerns
3. Results
3.1. Sample Description
3.2. Exploratory Factor Analysis
3.3. Reliability Analysis
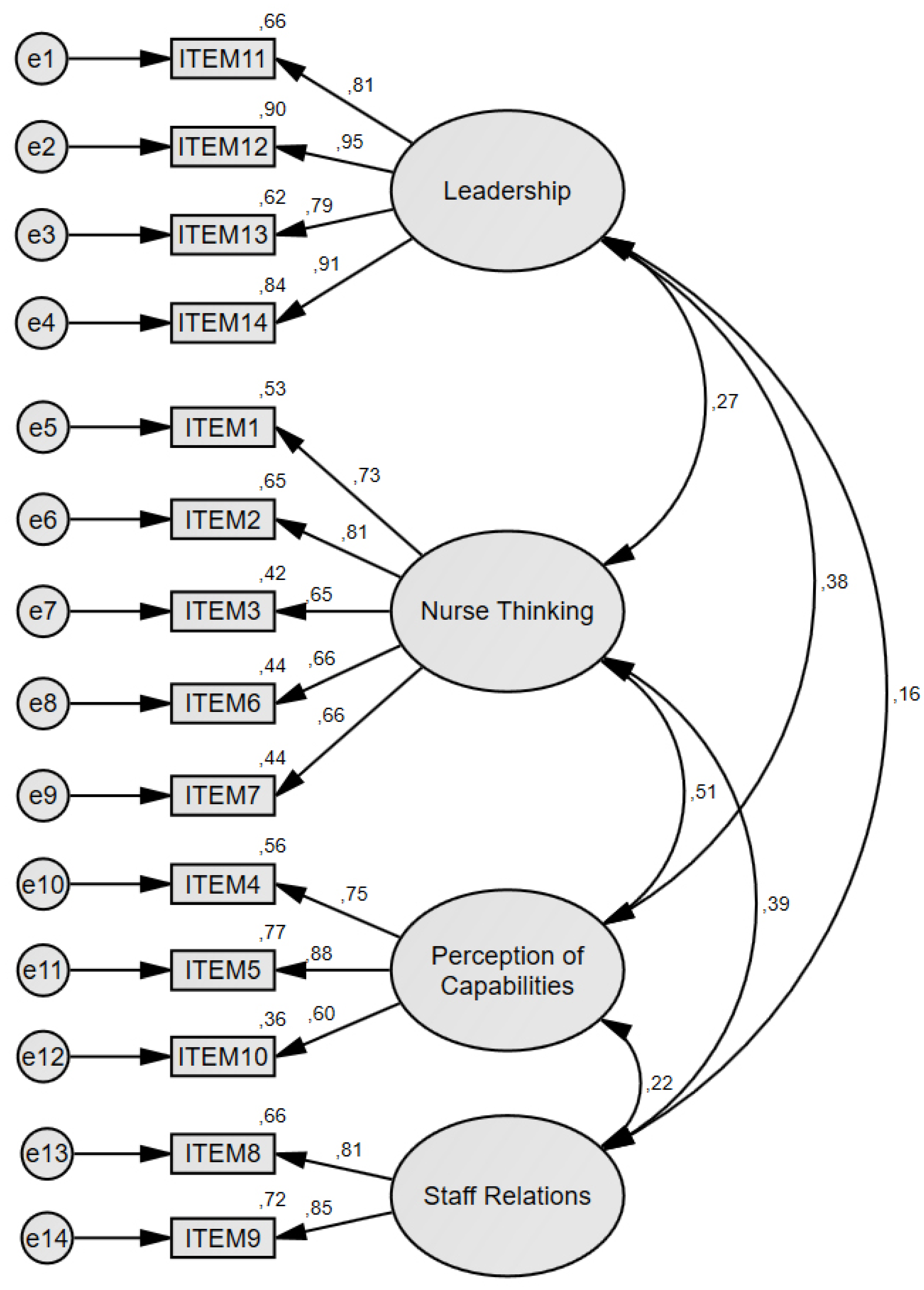
3.4. Confirmatory Factor Analysis
3.5. Cross-Sectional Analysis
4. Discussion
4.1. Renaming the Factors
4.2. Gender Differences
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. NSCI-S
| 1 |  | 8 |
| Totalmente Falso | Totalmente cierto | |
| 1. Me preocupo por las necesidades de mis pacientes. | 1 2 3 4 5 6 7 8 | |
| 2. La manera en que cuido a mis pacientes me hace sentir orgulloso/a | 1 2 3 4 5 6 7 8 | |
| 3. Disfruto mucho cuidando a mis pacientes | 1 2 3 4 5 6 7 8 | |
| 4. Soy capaz de dominar los conocimientos nuevos de la enfermería | 1 2 3 4 5 6 7 8 | |
| 5. Soy bueno/a aplicando mis conocimientos de enfermería a la atención del paciente | 1 2 3 4 5 6 7 8 | |
| 6. Encuentro estimulante aprender nuevos conocimientos de enfermería | 1 2 3 4 5 6 7 8 | |
| 7. Me gusta tener los conocimientos para resolver problemas de enfermería | 1 2 3 4 5 6 7 8 | |
| 8. Me gusta trabajar con mis compañeros/as | 1 2 3 4 5 6 7 8 | |
| 9. Soy capaz de construir buenas relaciones laborales con mis compañeros/as | 1 2 3 4 5 6 7 8 | |
| 10. Soy bueno/a ayudando a mis compañeros/as | 1 2 3 4 5 6 7 8 | |
| 11. Soy/seré un buen líder del equipo de enfermería | 1 2 3 4 5 6 7 8 | |
| 12. Disfruto/disfrutaré teniendo las responsabilidades de dirigir al equipo de enfermería | 1 2 3 4 5 6 7 8 | |
| 13. Soy/seré un líder respetado del equipo de enfermería | 1 2 3 4 5 6 7 8 | |
| 14. Me gusta/me gustará liderar un equipo de enfermería | 1 2 3 4 5 6 7 8 | |
References
- Angel, E.; Craven, R.; Denson, N. The Nurses Self-Concept Instrument (NSCI): Assessment of Psychometric Properties for Australian Domestic and International Student Nurses. Int. J. Nurs. Stud. 2012, 49, 880–886. [Google Scholar] [CrossRef]
- Sasat, S.; Burnard, P.; Edwards, D.; Naiyapatana, W.; Hebden, U.; Boonrod, W.; Arayathanitkul, B.; Wongmak, W. Self-Esteem and Student Nurses: A Cross-Cultural Study of Nursing Students in Thailand and the UK. Nurs. Health Sci. 2002, 4, 9–14. [Google Scholar] [CrossRef]
- Hensel, D. Relationships among Nurses’ Professional Self-Concept, Health, and Lifestyles. West J. Nurs. Res. 2011, 33, 45–62. [Google Scholar] [CrossRef] [PubMed]
- Arthur, D.; Randle, J. The Professional Self-Concept of Nurses: A Review of the Literature from 1992–2006. Aust. J. Adv. Nurs. 2007, 24, 60–64. [Google Scholar] [PubMed]
- Kim, M.S.; Cho, Y.O.; Park, J. Combination Relationship between Features of Person-Centered Care and Patient Safety Activities of Nurses Working in Small–Medium-Sized Hospitals: A Cross-Sectional Study. Nurs. Rep. 2022, 12, 861–872. [Google Scholar] [CrossRef] [PubMed]
- ten Hoeve, Y.; Jansen, G.; Roodbol, P. The Nursing Profession: Public Image, Self-Concept and Professional Identity. A Discussion Paper. J. Adv. Nurs. 2014, 70, 295–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groothuizen, J.E.; Callwood, A.; Allan, H.T. The “values Journey” of Nursing and Midwifery Students Selected Using Multiple Mini Interviews: Evaluations from a Longitudinal Study. Nurs. Inq. 2019, 26, e12307. [Google Scholar] [CrossRef]
- Drevdahl, D.J.; Canales, M.K. Being a Real Nurse: A Secondary Qualitative Analysis of How Public Health Nurses Rework Their Work Identities. Nurs. Inq. 2020, 27, e12360. [Google Scholar] [CrossRef]
- Çöplü, M.; Tekinsoy Kartın, P. Professional Self-Concept and Professional Values of Senior Students of the Nursing Department. Nurs. Ethics 2019, 26, 1387–1397. [Google Scholar] [CrossRef]
- McKinlay, A.; Cowan, S.; McVittie, C.; Ion, R. StartStudent Nurses’ Gender-Based Accounts of Men in Nursing. Procedia-Soc. Behav. Sci. 2010, 5, 345–349. [Google Scholar] [CrossRef]
- Hoffart, N.; McCoy, T.P.; Lewallen, L.P.; Thorpe, S. Differences in Gender-Related Profile Characteristics, Perceptions, and Outcomes of Accelerated Second Degree Nursing Students. J. Prof. Nurs. 2019, 35, 93–100. [Google Scholar] [CrossRef]
- Newman, C.; Stilwell, B.; Rick, S.; Peterson, K. Investing in the Power of Nurse Leadership: What Will It Take? IntraHealth International, Nursing Now; Johnson & Johnson: Washington, DC, USA, 2019. [Google Scholar]
- Woolfolk, A. Educationa Psychology; Pearson: Boston, MA, USA, 2006. [Google Scholar]
- Axpe, I.; Uralde, E. Two Versions (Paper and on Line) of an Educational Program for the Enhancement of the Physical Self-Concept. Rev. De Psicodidact. 2008, 13, 53–69. [Google Scholar]
- World Health Organization. Delivered by Women, Led by Men: A Gender and Equity Analysis of the Global Health and Social Workforce; Human Resources for Health Observer Series 24; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-151546-7. [Google Scholar]
- Roa García, A. El educación emocional, el autoconcepto, la autoestima y su importancia en la infancia. Edetania. Estud. Y Propues. Socioeducativos 2013, 44, 241–257. [Google Scholar]
- Esnaola, I.; Goñi, A.; Madariaga, J.M. El Autoconcepto: Perspectivas De Investigación. Rev. De Psicodidáctica 2008, 13, 69–96. [Google Scholar]
- Cazalla Luna, N.; Molero, D. Revisión teórica sobre el autoconcepto y su importancia en la adolescencia. Rev. Electrónica Investig. Docencia (REID) 2013, 10, 43–64. [Google Scholar]
- Yang, G.; Zang, X. Development of the Professional Competence and Professional Self-Concept of Undergraduate Nursing Students during the Clinical Practice Period: A Cross-Lagged Panel Analysis. Nurse Educ. Pract. 2022, 63, 103360. [Google Scholar] [CrossRef] [PubMed]
- Cowin, L.S.; Johnson, M.; Craven, R.G.; Marsh, H.W. Causal Modeling of Self-Concept, Job Satisfaction, and Retention of Nurses. Int. J. Nurs. Stud. 2008, 45, 1449–1459. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-H.; Kim, J.; Limb, J. Mediating Effect of Psychological Empowerment in Relationship between Professional Self-concept and Burnout in Psychiatric Nurses. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2012, 21, 229. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zou, H.; Wang, H.; Xu, X.; Liao, J. Do Emotional Labour Strategies Influence Emotional Exhaustion and Professional Identity or Vice Versa? Evidence from New Nurses. J. Adv. Nurs. 2020, 76, 577–587. [Google Scholar] [CrossRef]
- Porter, R.T.; Porter, M.J. Career Development: Our Professional Responsibility. J. Prof. Nurs. 1991, 7, 208–212. [Google Scholar] [CrossRef]
- Arthur, D. Measuring the Professional Self-Concept of Nurses: A Critical Review. J. Adv. Nurs. 1992, 17, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Arthur, D.; Thorne, S. Professional Self-Concept of Nurses: A Comparative Study of Four Strata of Nursing Students in a Canadian University. Nurse Educ. Today 1998, 18, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Cowin, L. Measuring Nurses’ Self-Concept. West J. Nurs. Res. 2001, 23, 313–325. [Google Scholar] [CrossRef]
- Xu, Y.; Liang, Y.; Ye, H.; Xu, Y. Literature Review of the Research on Nursing Students’ Professional Self-Concept. Med. Educ. Online 2023, 28, 2153396. [Google Scholar] [CrossRef]
- Arthur, D.; Pang, S.; Wong, T.; Alexander, M.F.; Drury, J.; Eastwood, H.; Johansson, I.; Jooste, K.; Naude, M.; Noh, C.H.; et al. Caring Attributes, Professional Self Concept and Technological Influences in a Sample of Registered Nurses in Eleven Countries. Int. J. Nurs. Stud. 1999, 36, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Gea-Caballero, V.; Castro-Sánchez, E.; Díaz-Herrera, M.Á.; Sarabia-Cobo, C.; Juárez-Vela, R.; Zabaleta-Del Olmo, E. Motivations, Beliefs, and Expectations of Spanish Nurses Planning Migration for Economic Reasons: A Cross-Sectional, Web-Based Survey. J. Nurs. Scholarsh. 2019, 51, 178–186. [Google Scholar] [CrossRef]
- Sheahan, D. Best Nurse Jobs—The Best Countries for Nurses to Work. Available online: https://news.euspert.com/best-nurse-jobs-best-countries-nurses-work/ (accessed on 13 January 2023).
- Kelly, S.; Courts, N. The Professional Self-Concept of New Graduate Nurses. Nurse Educ. Pract. 2007, 7, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-C.; Yeh, M.-L. Translation and Validation of the Nurses Self-Concept Instrument for College-Level Nursing Students in Taiwan. Nurse Educ. Today 2016, 36, 112–117. [Google Scholar] [CrossRef]
- Morgado, F.F.R.; Meireles, J.F.F.; Neves, C.M.; Amaral, A.C.S.; Ferreira, M.E.C. Scale Development: Ten Main Limitations and Recommendations to Improve Future Research Practices. Psicol. Refl. Crít. 2018, 30, 3. [Google Scholar] [CrossRef] [Green Version]
- Myers, N.D.; Ahn, S.; Jin, Y. Sample Size and Power Estimates for a Confirmatory Factor Analytic Model in Exercise and Sport: A Monte Carlo Approach. Res. Q. Exerc. Sport 2011, 82, 412–423. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.-T.; Wen, Z. In Search of Golden Rules: Comment on Hypothesis-Testing Approaches to Setting Cutoff Values for Fit Indexes and Dangers in Overgeneralizing Hu and Bentler’s (1999) Findings. Struct. Equ. Model. A Multidiscip. J. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Angel, E.; Craven, R.; Denson, N. The Nurses’ Self-Concept Instrument (NSCI): A Comparison of Domestic and International Student Nurses’ Professional Self-Concepts from a Large Australian University. Nurse Educ. Today 2012, 32, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Hofstede Insights. Compare Countries. Available online: https://www.hofstede-insights.com/fi/product/compare-countries/ (accessed on 28 December 2022).
- Calleja Toledano, P.; Ferrer Arnedo, C.; Perez Perez-Medrano, T. Claves En El Desarrollo Del Liderazgo: La Experiencia de Unas Enfermeras En España. Available online: https://archive.nursingnow.org/wp-content/uploads/2018/01/ARTICULO-for-Nigthingale-Challenge-Mat_Daley.pdf (accessed on 28 December 2022).
- Arrowsmith, V.; Lau-Walker, M.; Norman, I.; Maben, J. Nurses’ Perceptions and Experiences of Work Role Transitions: A Mixed Methods Systematic Review of the Literature. J. Adv. Nurs. 2016, 72, 1735–1750. [Google Scholar] [CrossRef]
- Fernández-Feito, A.; Basurto-Hoyuelos, S.; Palmeiro-Longo, M.R.; García-Díaz, V. Differences in Professional Values between Nurses and Nursing Students: A Gender Perspective. Int. Nurs. Rev. 2019, 66, 577–589. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, Y.-L. Demonstration of Caring by Males in Clinical Practice: A Literature Review. Int. J. Nurs. Sci. 2016, 3, 323–327. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.; Muldoon, O.T.; Moutray, M. Gender, Gender Roles and Completion of Nursing Education: A Longitudinal Study. Nurse Educ. Today 2010, 30, 303–307. [Google Scholar] [CrossRef]
- Özdemir, A.; Akansel, N.; Tunc, G.C. Gender and Career: Female and Male Nursing Students’ Perceptions of Male Nursing Role in Turkey. Health Sci. J. 2008, 2, 153–161. [Google Scholar]
- Davidhizar, R.; Cramer, C. Gender Differences in Leadership in the Health Professions. Health Care Manag. 2000, 18, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, M.G.; Topp, R.; AlYami, M.S. The Effect of Gender on Transformational Leadership and Job Satisfaction among Saudi Nurses. J. Adv. Nurs. 2018, 74, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hernández Yáñez, J.F. La Enfermería Frente al Espejo: Mitos y Realidades; Documentos de Trabajo (Laboratorio de Alternativas) Laboratorio de Alternativas: Madrid, Spain, 2010; Volume 1. [Google Scholar]
- Dresch, V.; Sánchez-López, M.d.P.; Saavedra, A.I. Gender and Health in Spanish Nurses. Paidéia 2018, 28, e2829. [Google Scholar] [CrossRef]


{kind=link}
| N | % | |
|---|---|---|
| Sex | - | - |
| Man | 54 | 11.2 |
| Woman | 429 | 88.8 |
| Current job | - | - |
| Hospitalization | 390 | 80.7 |
| Primary Care | 93 | 19.3 |
| Mean | SD | |
| Age | 43.87 | 10.79 |
| Years Nursing | 18.22 | 11.84 |
| Years in job | 5.63 | 8.08 |
| Item | Components 1 | |||
|---|---|---|---|---|
| Leadership | Nurse Thinking | Perception of Capabilities | Staff Relations | |
| NSCI11 | 0.83 | - | - | - |
| NSCI12 | 0.94 | - | - | - |
| NSCI13 | 0.84 | - | - | - |
| NSCI14 | 0.92 | - | - | - |
| NSCI1 | - | 0.75 | - | - |
| NSCI2 | - | 0.79 | - | - |
| NSCI3 | - | 0.71 | - | - |
| NSCI6 | - | 0.74 | - | - |
| NSCI7 | - | 0.74 | - | - |
| NSCI4 | - | - | 0.77 | - |
| NSCI5 | - | - | 0.84 | - |
| NSCI10 | - | - | 0.73 | - |
| NSCI8 | - | - | - | 0.88 |
| NSCI9 | - | - | - | 0.89 |
| Explained variance | 23.52 | 21.46 | 15.01 | 13.14 |
| Cronbach’s alpha | 0.92 | 0.81 | 0.77 | 0.82 |
| Model | χ2 | gl | χ2/gL | CFI | IFI | RMSEA |
|---|---|---|---|---|---|---|
| NSCI—Spanish model | 193.726 | 71 | 2.729 | 0.921 | 0.922 | 0.088 |
| NSCI—Original model | 329.961 | 71 | 4.647 | 0.834 | 0.836 | 0.128 |
| NSCI—Taiwanese model | 461.204 | 76 | 6.068 | 0.752 | 0.755 | 0.150 |
| Dimension | Gender | N | Mean (SD) | Z | p |
|---|---|---|---|---|---|
| Nurse Thinking | Man | 54 | 7.04 (0.75) | 5.53 | <0.001 |
| Woman | 429 | 7.56 (0.51) | |||
| Perception of Capabilities | Man | 54 | 6.64 (0.84) | 2.01 | <0.05 |
| Woman | 429 | 6.89 (0.76) | |||
| Staff Relations | Man | 54 | 7.28 (1.05) | 0.18 | 0.86 |
| Woman | 429 | 7.35 (0.85) | |||
| Leadership | Man | 54 | 6.62 (1.88) | 5.91 | <0.001 |
| Woman | 429 | 5.42 (1.53) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laborería-Romances, A.; Navas-Ferrer, C.; Anguas-Gracia, A.; Callén-Galindo, M.; Antón-Solanas, I.; Urcola-Pardo, F. Translation, Cultural Adaptation and Validation of the Nurses Self-Concept Instrument (NSCI) to Spanish. Int. J. Environ. Res. Public Health 2023, 20, 1529. https://doi.org/10.3390/ijerph20021529
Laborería-Romances A, Navas-Ferrer C, Anguas-Gracia A, Callén-Galindo M, Antón-Solanas I, Urcola-Pardo F. Translation, Cultural Adaptation and Validation of the Nurses Self-Concept Instrument (NSCI) to Spanish. International Journal of Environmental Research and Public Health. 2023; 20(2):1529. https://doi.org/10.3390/ijerph20021529
Chicago/Turabian StyleLaborería-Romances, Alba, Carlos Navas-Ferrer, Ana Anguas-Gracia, Marta Callén-Galindo, Isabel Antón-Solanas, and Fernando Urcola-Pardo. 2023. "Translation, Cultural Adaptation and Validation of the Nurses Self-Concept Instrument (NSCI) to Spanish" International Journal of Environmental Research and Public Health 20, no. 2: 1529. https://doi.org/10.3390/ijerph20021529
APA StyleLaborería-Romances, A., Navas-Ferrer, C., Anguas-Gracia, A., Callén-Galindo, M., Antón-Solanas, I., & Urcola-Pardo, F. (2023). Translation, Cultural Adaptation and Validation of the Nurses Self-Concept Instrument (NSCI) to Spanish. International Journal of Environmental Research and Public Health, 20(2), 1529. https://doi.org/10.3390/ijerph20021529