
Virtual Reality Exercise Program Effects on Body Mass Index, Depression, Exercise Fun and Exercise Immersion in Overweight Middle-Aged Women: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
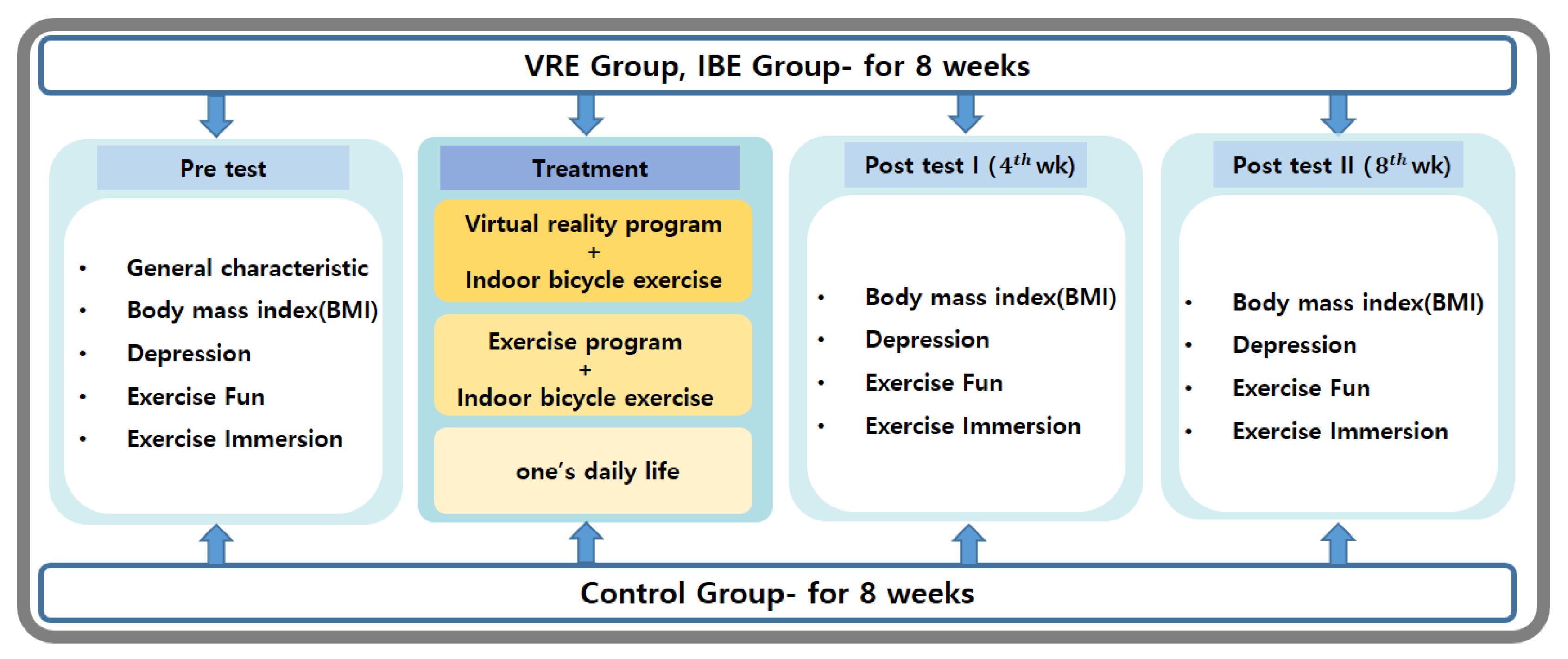
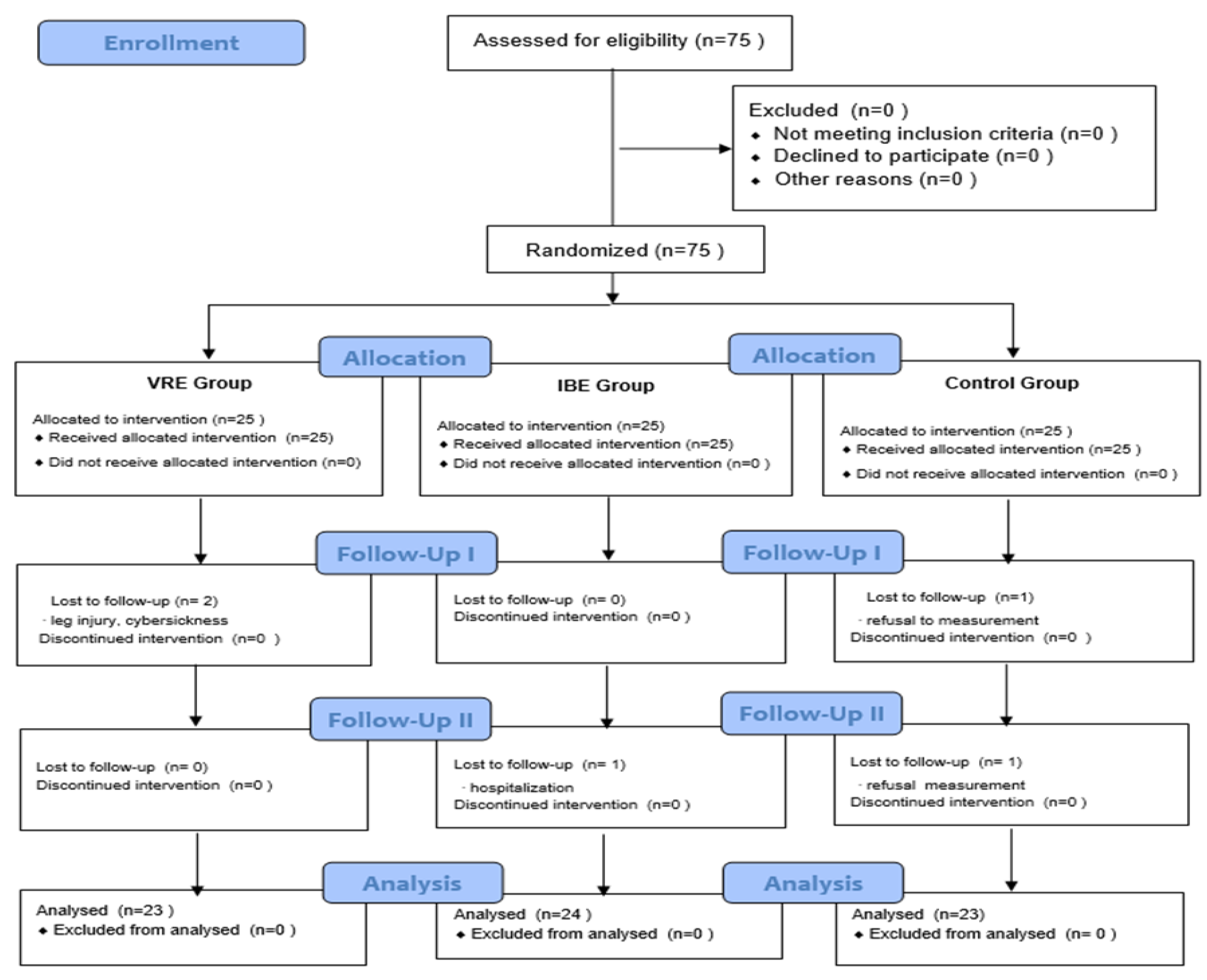
2.1. Study Design and Population
2.2. Randomization
2.3. Interventions
2.4. Outcome Measurement
2.4.1. BMI
2.4.2. Depression
2.4.3. Exercise Fun
2.4.4. Exercise Immersion
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
3.1. Homogeneity of the Participants’ General Characteristics and Prior Dependent Variables
3.2. Outcome Variables
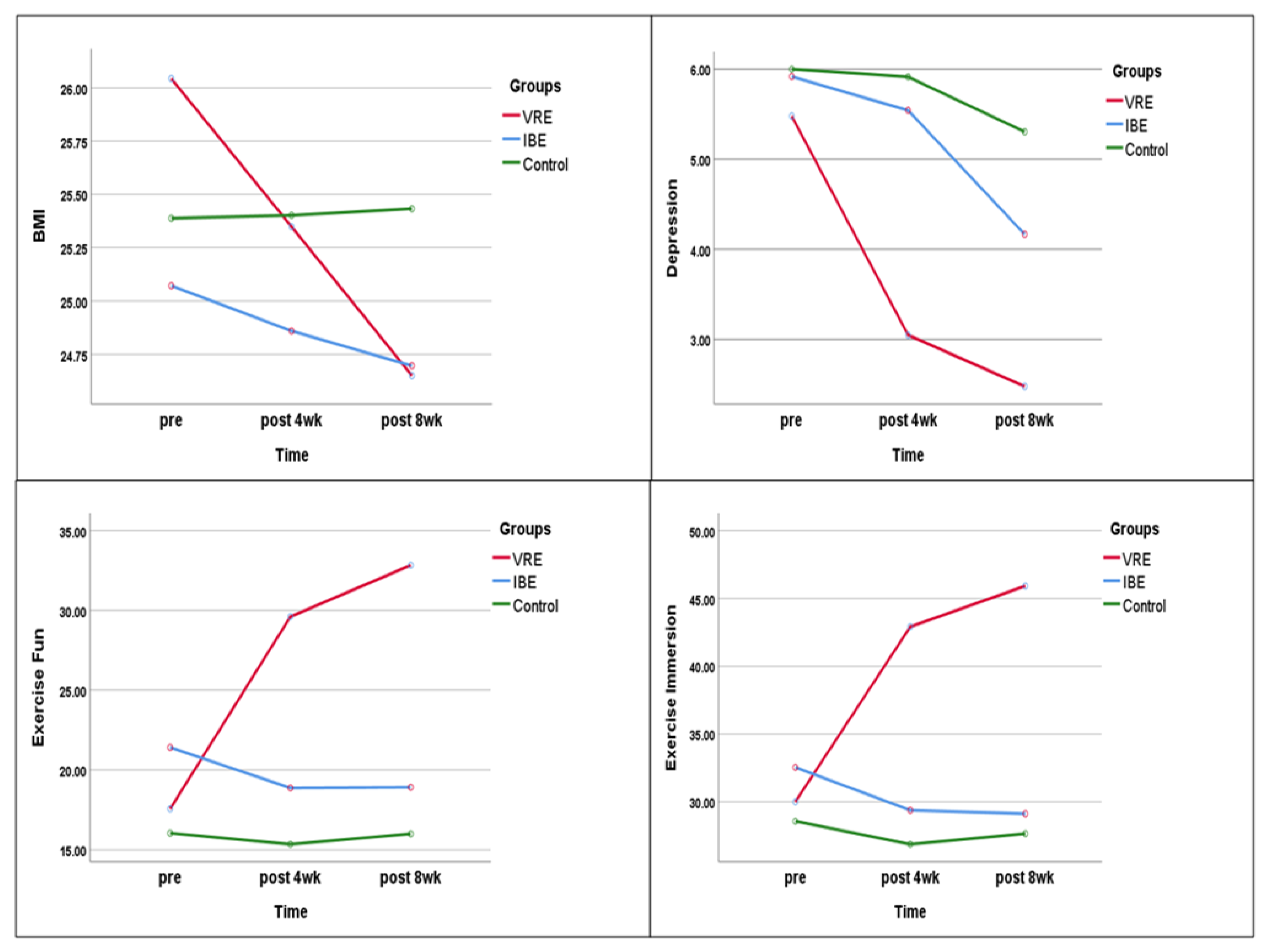
3.2.1. BMI
3.2.2. Depression
3.2.3. Exercise Fun
3.2.4. Exercise Immersion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, W.P.T. Obesity: A global public health challenge. Clin. Chem. 2018, 64, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.J.; Morton, J.; Brethauer, S.; Mattar, S.; De Maria, E.; Benz, J.K.; Titus, J.; Sterrett, D. Obesity in America. Surg. Obes. Relat. Dis. 2017, 13, 1643–1650. [Google Scholar] [CrossRef] [PubMed]
- National Health Statistics: Health and Welfare Ministry E-Country Indicators of Obesity Prevalence. 2018. Available online: https://www.index.go.kr/ (accessed on 7 March 2021).
- Chu, S.H.; Lee, M.K.; Kowalski, J.; Beck, J.; Schwertz, D. Effect of estrogen on ovariectomy-induced obesity in rats. J. Korean Biol. Nurs. Sci. 2008, 10, 80–87. [Google Scholar]
- Upadhyay, J.; Farr, O.; Perakakis, N.; Ghaly, W.; Mantzoros, C. Obesity as a disease. Med. Clin. N. Am. 2018, 102, 13–33. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Ma, R.W. A comparison of factors influencing health-related quality of life by obesity among middle-aged women. Asia-Pac. J. Multimed. Serv. Converg. Art Humanit. Sociol. 2018, 8, 691–702. [Google Scholar]
- Mulugeta, A.; Zhou, A.; Power, C.; Hyppönen, E. Obesity and depressive symptoms in mid-life: A population-based cohort study. BMC Psychiatry 2018, 18, 297. [Google Scholar] [CrossRef] [Green Version]
- Wright, S.M.; Aronne, L.J. Causes of obesity. Abdom. Radiol. 2012, 37, 730–732. [Google Scholar] [CrossRef]
- Koithan, M. Mind-body solutions for obesity. J. Nurse Pract. 2009, 5, 536–537. [Google Scholar] [CrossRef] [Green Version]
- Chun, T.; Park, K.; Seo, D. Effects of combined exercise training on endocrine system and immunoglobulin in middle aged women. Exerc. Sci. 2008, 17, 157–162. [Google Scholar]
- Mi, C.S. Coronavirus infections-19 and challenges for future disease response. Korea Inst. Health Soc. Aff. 2020, 374, 1–8. [Google Scholar]
- Koh, K.W. Physical activity guideline for social distancing during COVID-19. Korean J. Health Educ. Promot. 2022, 37, 109–112. [Google Scholar] [CrossRef]
- Pagan, I.; Costa, D.L.; McGee, J.K.; Richards, J.H.; Dye, J.A.; Dykstra, M.J. Metals mimic airway epithelial injury induced by in vitro exposure to Utah Valley ambient particulate matter extracts. J. Toxicol. Environ. Health Part A 2003, 66, 1087–1112. [Google Scholar] [CrossRef] [PubMed]
- Ristovski, Z.D.; Miljevic, B.; Surawski, N.C.; Morawska, L.; Fong, K.M.; Goh, F.; Yang, I. Respiratory health effects of diesel particulate matter. Respirology 2012, 17, 201–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, A.S. Impact of particulate matter on health. J. Korean Med. Assoc. 2014, 57, 763–768. [Google Scholar] [CrossRef]
- Suyanto, B.; Egalita, N.; Sugihartati, R. Facing the new reality of post Covid-19: A demand for lifestyle-based social engineering. Talent. Dev. Excell. 2020, 12, 2333–2342. [Google Scholar]
- Lee, S.; Park, C.; Jeong, D.; Choi, J.; Kim, H. Development of physical activity monitoring system using multiple motion sensors. In Proceedings of the Korean Society of Computer Information Conference, Gyeongju, Republic of Korea, 5–7 October 2020; Korean Society of Computer Information: Gyeongju, Republic of Korea, 2020. [Google Scholar]
- Yang, Y.J. Evidence based exercise to control weight. J. Korean Med. Assoc. 2017, 60, 806–816. [Google Scholar] [CrossRef] [Green Version]
- Youn, J.-H.; Choi, H.-S. Development of sportainment realistic bike simulator. J. Korea Contents Assoc. 2014, 14, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Burdea, G.C.; Coiffet, P. Virtual Reality Technology; John Wiley & Sons: New York, NY, USA, 2003. [Google Scholar]
- Bowman, D.A.; McMahan, R.P. Virtual reality: How much immersion is enough? Computer 2007, 40, 36–43. [Google Scholar] [CrossRef]
- Sveistrup, H.; Thornton, M.; Bryanton, C.; McComas, J.; Marshall, S.; Finestone, H.; McCormick, A.; McLean, J.; Brien, M.; Lajoie, Y.; et al. Outcomes of intervention programs using flatscreen virtual reality. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004. [Google Scholar] [CrossRef]
- Sanchez-Vives, M.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef]
- Cho, H.; Sohng, K.-Y. The effect of a virtual reality exercise program on physical fitness, body composition, and fatigue in hemodialysis patients. J. Phys. Ther. Sci. 2014, 26, 1661–1665. [Google Scholar] [CrossRef] [Green Version]
- You, Y.H. The effect of participation in virtual reality sports on exercise commitment and lower extremity muscular function of persons with intellectual disability. Korean J. Phys. Educ. 2017, 56, 613–623. [Google Scholar] [CrossRef]
- Song, C.; Shin, W.S.; Lee, S. The effect of a virtual reality-based exercise program using a video game on the muscle strength, balance and gait abilities in the elderly. J. Korea Gerontol. Soc. 2009, 29, 1261–1275. [Google Scholar]
- Kim, Y.G.; Kang, S.H. Effects of virtual reality-based exercise on balance, gait, and falls efficacy in patients with Parkinson’s disease: A pilot study. J. Korean Soc. Integr. Med. 2016, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.H. Effects of a virtual reality exercise program (wii) on cognitive function of elderly people with Alzheimer dementia. Off. J. Korean Acad. Kinesiol. 2017, 19, 35–44. [Google Scholar] [CrossRef]
- Kim, Y.G. The effect of the virtual reality rehabilitation system on activities of daily living, cognitive function, self-esteem in stroke. J. Korea Acad.-Ind. Coop. Soc. 2015, 16, 5476–5484. [Google Scholar] [CrossRef]
- Jang, Y.S. Future of taekwondo contents industry based upon the development of virtual reality system. Taekwondo J. Kukkiwon 2018, 9, 177–195. [Google Scholar] [CrossRef]
- Ou, S.W. Exercise prescription in obese patients. Korean J. Health Promot. Dis. Prev. 2002, 2, 167–172. [Google Scholar]
- Swain, D.P.; Brawner, C.A.; Chambliss, H.O.; Nagelkirk, P.R.; Bayles, M.P.; Swank, A.M. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Kim, H.S.; Shin, C.H.; Jin, J.K. Validity of RPE-13 as optimal exercise intensity. Exerc. Sci. 1997, 6, 33–44. [Google Scholar]
- Kaminsky, L.; Leonard, A. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Park, D.S. Let’s find your own exercise method! Mon. Diabetes 2008, 219, 15–19. [Google Scholar]
- Jung, Y.G. Validity Verification of Sport Commitment Behavior Scale. Korean Soc. Sport Psychol. (KJSP) 2004, 15, 1–22. [Google Scholar]
- Lee, J.I. Effect of walking exercise intensities on fatigue, serum lipids, and immune function among middle-aged women. J. Korean Acad. Nurs. 2006, 36, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Eta-Squared and Partial Eta-Squared in Fixed Factor Anova Designs. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Kim, C.S.; Kang, S.Y.; Nam, J.S.; Cho, M.H.; Park, J.S.; Nam, J.Y.; Yoon, S.J.; Ahn, C.W.; Cha, B.S.; Lim, S.K. The effects of walking exercise program on BMI, percentage of body fat and mood state for women with obesity. J. Korean Soc. Study Obes. 2004, 13, 132–140. [Google Scholar]
- Lee, K.-J.; Yi, Y.-J.; Kim, C.-N. Comparison of the effects of an exercise program in non-obese and obese women. J. Korean Acad. Nurs. 2007, 37, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lee, W.H. The effect of an integrated kinetic program on the change of body composition and blood lipid components in middle-aged women. J. Korean Soc. Phys. Ther. 2012, 24, 41–50. [Google Scholar]
- Choi, H.J.; Cha, H.J.; Choi, S.M. VR sky walking: A VR fitness system using a sky walker equipment. Proc. HCI Korea 2018, 157, 280–283. [Google Scholar]
- Ko, D.-S.; Jung, D.-I.; Lee, S.-H. Physical functions of industrial workers with chronic low back pain and changes in health-related quality of life according to virtual reality exercise program. J. Korea Acad.-Ind. Coop. Soc. 2012, 13, 4564–4571. [Google Scholar] [CrossRef] [Green Version]
- Ha, C.A. The Effect of Virtual Reality-Based Exercise Program on the Mobility and Balance Abilities for the Elderly; Chosun University Graduate School of Public Health: Gwangju, Republic of Korea, 2010. [Google Scholar]
- Song, G.B.; Park, E.C. Comparison of the effects of task-oriented training and virtual reality training on upper extremity function, balance ability, and depression in stroke patients. J. Korean Soc. Phys. Med. 2016, 11, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.J.; Choi, S.W.; Moon, S.Y.; Park, H.I.; Hwang, H.K.; Kim, M.K.; Seok, J.H. Treatment effect of psychoeducation and training program using virtual reality technique in the patients with depressive symptoms. J. Korean Neuropsychiatr. Assoc. 2020, 59, 51. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Lee, S.K.; Kim, Y.H.; Chae, J.B. The effects of 4 weeks training using virtual reality game on balance and gait ability, depression of elderly people. J. Korea Proprioceptive Neuromuscul. Facil. Assoc. 2012, 10, 41–46. [Google Scholar] [CrossRef]
- Kim, Y.N.; Lee, D.K. Effects of dance sports in virtual reality on balance, depression and ADL in stroke patients. J. Korean Soc. Phys. Ther. 2013, 25, 360–365. [Google Scholar]
- Bae, J.E.; Kim, S.I. A Development plan of serious game based on virtual reality through the trend analysis on internal/external game industry. J. Digit. Des. 2014, 14, 737–748. [Google Scholar] [CrossRef]
- Kang, M.W.; Lee, J.K.; Lee, H.G.; Kim, H.; Kang, M.S. A development of extreme escape game using virtual reality. In Proceedings of the Korean Institute of Information and Communication Sciences Conference; The Korea Institute of Information and Communication Engineering: Cheonan, Republic of Korea, 2014; pp. 557–558. [Google Scholar]
- Yao, S.; Kim, G. The effects of immersion in a virtual reality game: Presence and physical activity. In HCI in Games; Fang, X.W., Ed.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 234–242. [Google Scholar] [CrossRef]
- Park, M.J.; Lee, B.J. The features of VR (virtual reality) communication and the aspects of its experience. J. Commun. Res. 2004, 41, 29–60. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Category | VRE (n = 23) | IBE (n = 24) | Control (n = 23) | X² or F * | p-Value |
|---|---|---|---|---|---|---|
| M (SD) or n (%) | M (SD) or n (%) | M (SD) or n (%) | ||||
| Age (years) | 47.74 ± 5.50 | 49.00 ± 6.77 | 48.26 ± 7.56 | 0.213 | 0.809 | |
| Marital status | Married | 20 (87.0) | 18 (75.0) | 17 (73.9) | ||
| Single | 2 (8.7) | 5 (20.8) | 4 (17.4) | |||
| Divorced | 0 | 0 | 1 (4.3) | |||
| Widowed | 1 (4.3) | 1 (4.2) | 1 (4.3) | 3.515 | 0.742 | |
| Education | Less than high school | 7 (30.4) | 9 (37.5) | 4 (17.4) | ||
| More than college | 16 (69.6) | 15 (62.5) | 19 (82.6) | 2.385 | 0.303 | |
| Employment | Yes | 17 (73.9) | 19 (79.2) | 15 (65.2) | ||
| No | 6 (26.1) | 5 (20.8) | 8 (34.8) | 1.175 | 0.556 | |
| Alcohol consumption | Yes | 12 (52.2) | 14 (58.3) | 14 (60.9) | ||
| No | 11 (47.8) | 10 (41.7) | 9 (39.1) | 0.376 | 0.829 | |
| BMI | 26.04 ± 2.25 | 25.07 ± 2.01 | 25.39 ± 1.67 | 1.449 | 0.242 | |
| Depression | 5.48 ± 4.50 | 5.92 ± 3.22 | 6.00 ± 2.84 | 0.141 | 0.869 | |
| Exercise fun (NRS) | 17.57 ± 8.78 | 21.42 ± 8.21 | 16.04 ± 9.55 | 2.309 | 0.107 | |
| Exercise immersion | 30.00 ± 7.20 | 32.54 ± 8.61 | 28.57 ± 8.41 | 1.454 | 0.241 | |
| Variables | VRE (n = 23) | IBE (n = 24) | Control (n = 23) | F * (p) | F ** (p) | |
|---|---|---|---|---|---|---|
| BMI(kg/m2) | Baseline | 26.04 ± 2.25 | 25.07 ± 2.00 | 25.39 ± 1.67 | 1.449 (0.242) | Time |
| 109.320 (p < 0.001) | ||||||
| After 4 weeks | 25.35 ± 2.09 a | 24.86 ± 1.97 b | 25.40 ± 1.07 c | 30.541 (<0.001) | G*T | |
| 59.491 (p < 0.001) | ||||||
| After 8 weeks | 24.65 ± 1.96 a | 24.70 ± 1.81 b | 25.43 ± 1.78 c | 112.527 (<0.001) | Group | |
| 0.548 (p = 0.581) | ||||||
| Depression | Baseline | 5.48 ± 4.50 | 5.92 ± 3.22 | 6.00 ± 2.84 | 0.141 (0.869) | Time |
| 16.371 (p < 0.001) | ||||||
| After 4 weeks | 3.05 ± 1.89 a | 5.54 ± 3.51 b | 5.91 ± 3.84 b | 7.804 (0.001) | G*T | |
| 3.462 (p = 0.010) | ||||||
| After 8 weeks | 2.48 ± 1.47 a | 4.17 ± 2.71 b | 5.30 ± 3.13 b | 9.502 (<0.001) | Group | |
| 3.555 (p = 0.034) | ||||||
| Exercise fun | Baseline | 17.57 ± 8.78 | 21.42 ± 8.21 | 16.04 ± 9.55 | 2.309 (0.107) | Time |
| 8.571 (p < 0.001) | ||||||
| After 4 weeks | 29.61 ± 5.47 a | 18.88 ± 6.65 b | 15.35 ± 10.28 b | 33.731 (<0.001) | G*T | |
| 12.373 (p < 0.001) | ||||||
| After 8 weeks | 32.83 ± 4.61 a | 18.92 ± 7.10 b | 16.00 ± 10.50 b | 40.554 (<0.001) | Group | |
| 14.052 (p < 0.001) | ||||||
| Immersion | Baseline | 30.00 ± 7.20 | 32.54 ± 8.61 | 28.57 ± 8.42 | 1.454 (0.241) | Time |
| 7.163 (p = 0.002) | ||||||
| After 4 weeks | 42.91 ± 5.49 a | 29.38 ± 7.57 b | 26.87 ± 9.64 b | 39.187 (<0.001) | G*T | |
| 14.629 (p < 0.001) | ||||||
| After 8 weeks | 45.91 ± 5.95 a | 29.13 ± 6.84 b | 27.65 ± 8.90 b | 52.346 (<0.001) | Group | |
| 21.219 (p < 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, E.-Y.; Kim, Y.-S.; Lee, Y.-J.; Hur, M.-H. Virtual Reality Exercise Program Effects on Body Mass Index, Depression, Exercise Fun and Exercise Immersion in Overweight Middle-Aged Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 900. https://doi.org/10.3390/ijerph20020900
Seo E-Y, Kim Y-S, Lee Y-J, Hur M-H. Virtual Reality Exercise Program Effects on Body Mass Index, Depression, Exercise Fun and Exercise Immersion in Overweight Middle-Aged Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):900. https://doi.org/10.3390/ijerph20020900
Chicago/Turabian StyleSeo, Eun-Young, Yeon-Suk Kim, Yu-Jin Lee, and Myung-Haeng Hur. 2023. "Virtual Reality Exercise Program Effects on Body Mass Index, Depression, Exercise Fun and Exercise Immersion in Overweight Middle-Aged Women: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 2: 900. https://doi.org/10.3390/ijerph20020900