
Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
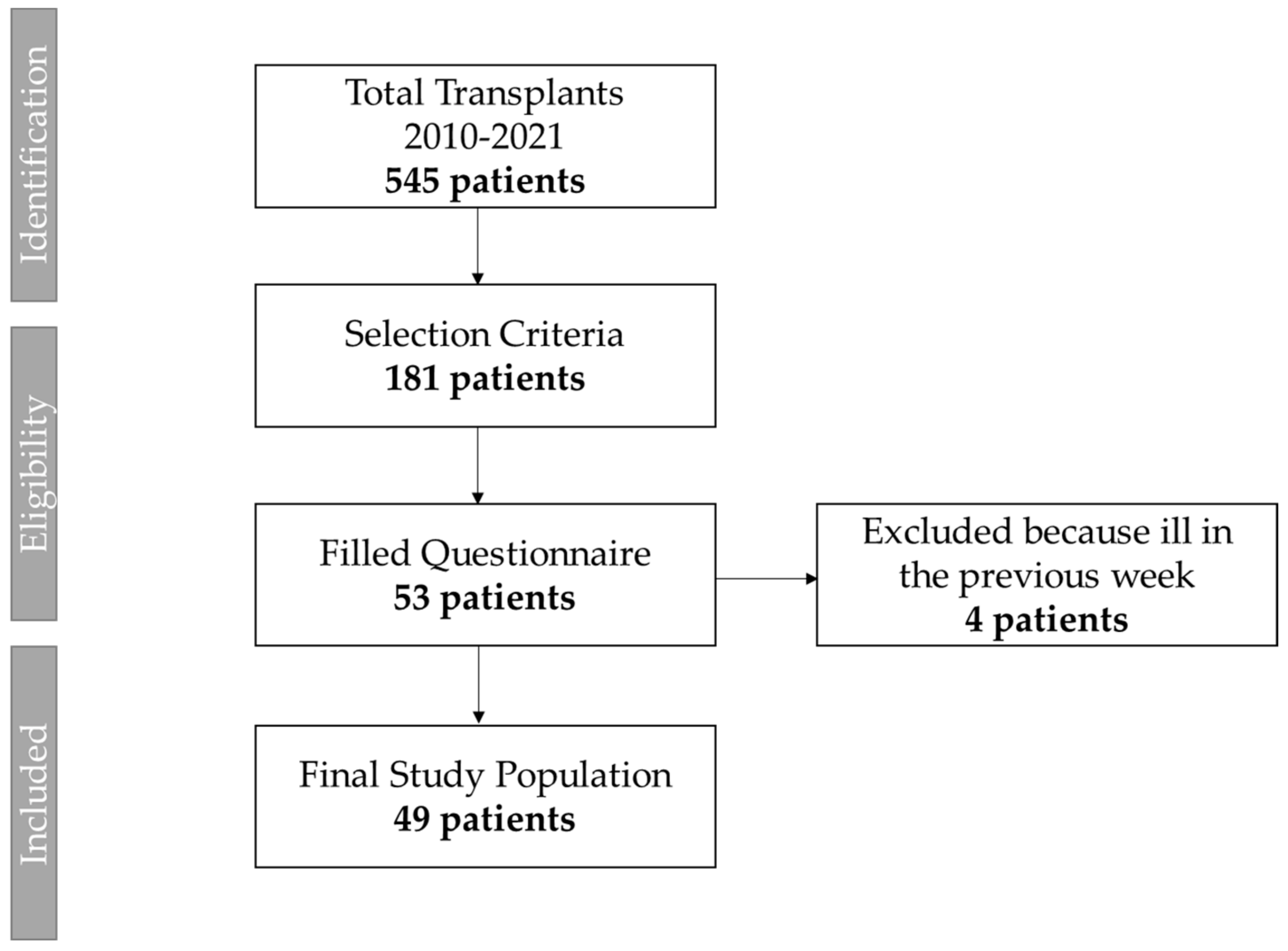
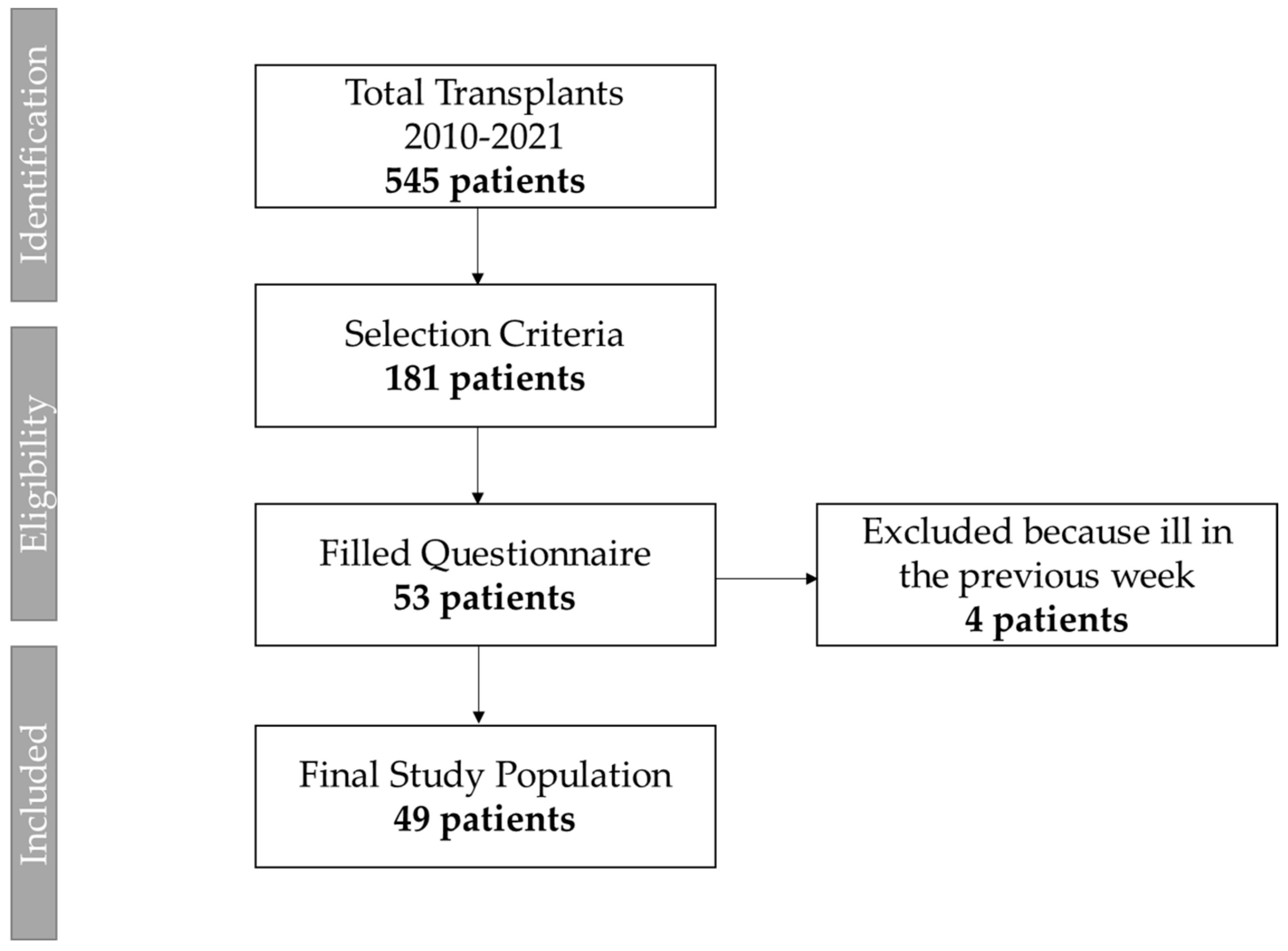
2.2. Participants
- Age between 8 and 18 years old;
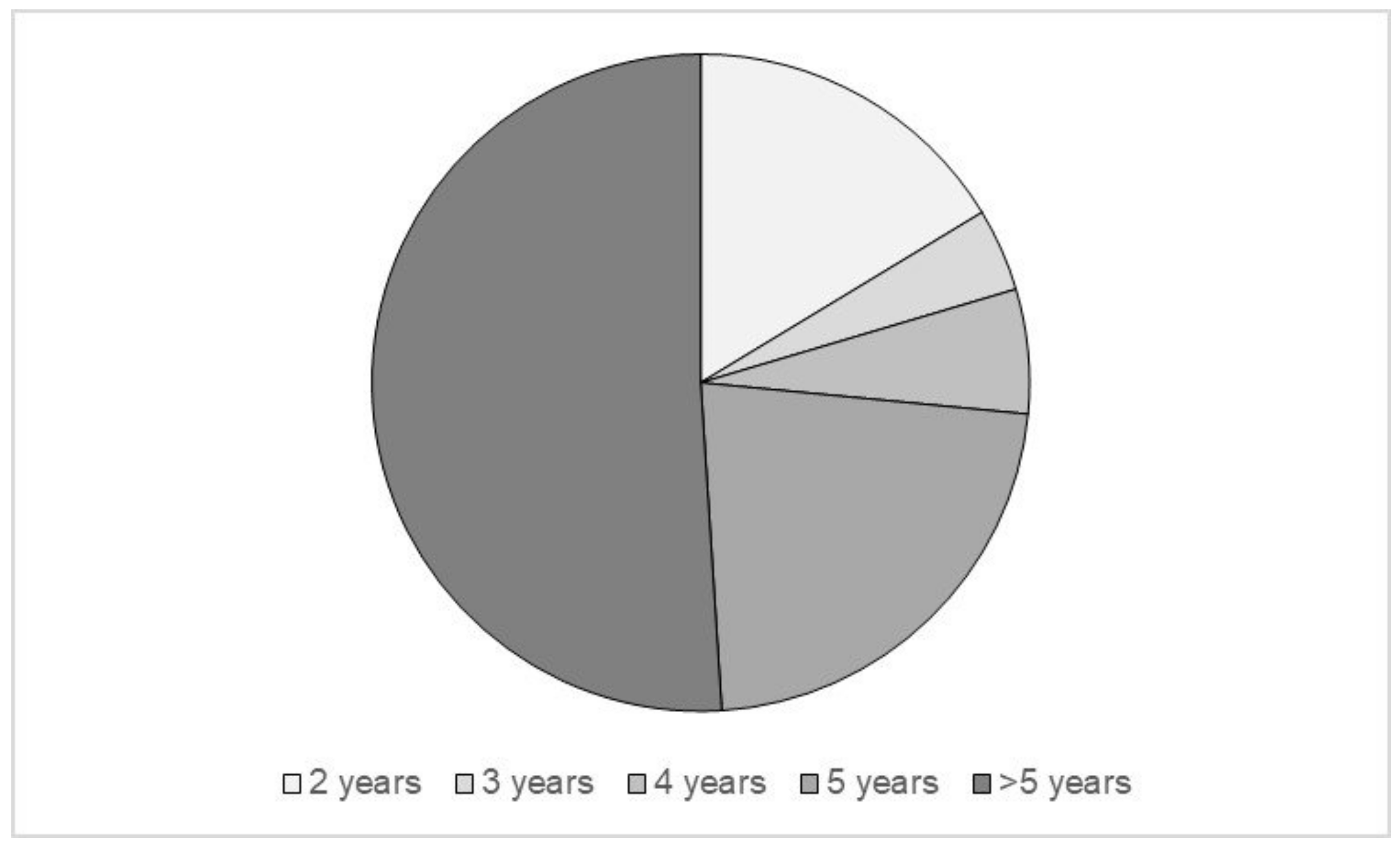
- At least 2 years after the intervention (range 2–5 or more years);
- Stable clinical condition.
- Exclusion criteria were
- Patients unable to complete the questionnaire due to age and/or psycho-physical limitations;
- Patients with a history of congenital heart disease, even if corrected and cured.
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Müller, P.C.; Kabacam, G.; Vibert, E.; Germani, G.; Petrowsky, H. Current status of liver transplantation in Europe. Int. J. Surg. 2020, 82S, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Karam, V.; Cailliez, V.O.; Grady, J.G.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)—50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, Y.; Wang, X.; Yang, H.; Zhong, S. Survival and Complication of Liver Transplantation in Infants: A Systematic Review and Meta-Analysis. Front. Pediatr. 2021, 9, 628771. [Google Scholar] [CrossRef] [PubMed]
- Boenink, R.; Astley, M.E.; Huijben, J.A.; Stel, V.S.; Kerschbaum, J.; Ots-Rosenberg, M.; Åsberg, A.A.; Lopot, F.; Golan, E.; Castro de la Nuez, P.; et al. The ERA Registry Annual Report 2019: Summary and age comparisons. Clin. Kidney J. 2021, 15, 452–472. [Google Scholar] [CrossRef] [PubMed]
- Tsai, E.; Ettenger, R. Kidney Transplantation in Children. In Handbook of Kidney Transplantation; Danovitch, G.M., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Hebert, S.A.; Swinford, R.D.; Hall, D.R.; Au, J.K.; Bynon, J.S. Special Considerations in Pediatric Kidney Transplantation. Adv. Chronic Kidney Dis. 2017, 24, 398–404. [Google Scholar] [CrossRef]
- Cuenca, A.G.; Yeh, H. Improving patients outcomes following pediatric liver transplant: Current perspectives. Transpl. Res. Risk Manag. 2019, 11, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Miloh, T.; Barton, A.; Wheeler, J.; Pham, Y.; Hewitt, W.; Keegan, T.; Sanchez, C.; Bulut, P.; Goss, J. Immunosuppression in pediatric liver transplant recipients: Unique aspects. Liver Transplant. 2017, 23, 244–256. [Google Scholar] [CrossRef] [Green Version]
- Blondet, N.M.; Healey, P.J.; Hsu, E. Immunosuppression in the pediatric transplant recipient. Semin. Pediatr. Surg. 2017, 26, 193–198. [Google Scholar] [CrossRef]
- Yanik, E.L.; Smith, J.M.; Shiels, M.S.; Clarke, C.A.; Lynch, C.F.; Kahn, A.R.; Koch, L.; Pawlish, K.S.; Engels, E.A. Cancer risk after pediatric solid organ transplantation. Pediatrics 2017, 139, e20163893. [Google Scholar] [CrossRef] [Green Version]
- Kitchlu, A.; Dixon, S.; Dirk, J.S.; Chanchlani, R.; Vasilevska-Ristovska, J.; Borges, K.; Dipchand, A.I.; Ng, V.L.; Hebert, D.; Solomon, M.; et al. Elevated risk of cancer after solid organ transplant in childhood. Transplantation 2019, 103, 588–596. [Google Scholar] [CrossRef]
- Brar, S.; Dixon, S.N.; Paterson, J.M.; Dirk, J.; Hahn, E.; Kim, S.J.; Ng, V.; Solomon, M.; Vasilevska-Ristovska, J.; Banh, T.; et al. Incidence of cardiovascular disease and mortality in childhood solid organ transplant recipients: A population-based study. Pediatr. Nephrol. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Memaran, N.; Borchert-Mörlins, B.; Schmidt, B.M.W.; Sugianto, R.I.; Wilke, H.; Blöte, R.; Baumann, U.; Bauer, E.; von Wick, A.; Junge, N.; et al. High Burden of Subclinical Cardiovascular Target Organ Damage After Pediatric Liver Transplantation. Liver Transpl. 2019, 25, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Harambat, J.; Cochat, P. Growth after renal transplantation. Pediatr. Nephrol. 2009, 24, 1297–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Bruton, A.; Matute-Llorente, Á.; González-Agüero, A.; Casajús, J.A.; Vicente-Rodríguez, G. Plyometric exercise and bone health in children and adolescents: A systematic review. World J. Pediatr. 2017, 13, 112–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuberger, J.; Armstrong, M.J.; Fisher, J.; Mark, P.; Schmidtke, K.; Sharif, A.; Vlaev, I. Sport and Exercise in Improving Outcomes After Solid Organ Transplantation: Overview From a UK Meeting. Transplantation 2019, 103, S1–S11. [Google Scholar] [CrossRef]
- Roi, G.S.; Stefoni, S.; Mosconi, G.; Brugin, E.; Burra, P.; Ermolao, A.; Granito, M.; Macini, P.; Mastrosimone, S.; Nacchia, F.; et al. Physical activity in solid organ transplant recipients: Organizational aspects and preliminary results of the Italian project. Transplant. Proc. 2014, 46, 2345–2349. [Google Scholar] [CrossRef]
- Mosconi, G.; Cuna, V.; Tonioli, M.; Totti, V.; Roi, G.S.; Sarto, P.; Stefoni, S.; Trerotola, M.; Costa, A.N. Physical activity in solid organ transplant recipients: Preliminary results of the Italian project. Kidney Blood Press. Res. 2014, 39, 220–227. [Google Scholar] [CrossRef]
- Totti, V.M.; Tamè, M.; Burra, P.; Mosconi, G.; Roi, G.S.; Sella, G.; Ermolao, A.; Ferrarese, A.; Sgarzi, S.; Savino, G.; et al. Physical Condition, Glycemia, Liver Function, and Quality of Life in Liver Transplant Recipients After a 12-Month Supervised Exercise Program. Transplant. Proc. 2019, 51, 2952–2957. [Google Scholar] [CrossRef]
- Chambers, J.H.; Zerofsky, M.; Lustig, R.H.; Rosenthal, P.; Perito, E.R. Diet and Exercise in Pediatric Liver Transplant Recipients: Behaviors and Association with Metabolic Syndrome. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 81–88. [Google Scholar] [CrossRef]
- Thorsteinsdottir, H.; Diseth, T.H.; Lie, A.; Tangeraas, T.; Matthews, I.; Åsberg, A.; Bjerre, A. Small effort, high impact: Focus on physical activity improves oxygen uptake (VO2peak), quality of life and mental health after pediatric renal transplantation. Pediatr. Transplant. 2018, 22, e13242. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.; Donen, R.M. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual. Ph.D. Thesis, College of Kinesiology, University of Saskatchewan, Saskatoon, SK, Canada, 2004. [Google Scholar]
- Gobbi, E.; Elliot, C.; Varnier, M.; Carraro, A. Psychometric Properties of the Physical Activity Questionnaire for Older Children in Italy: Testing the Validity among a General and Clinical Pediatric Population. PLoS ONE 2016, 11, e0156354. [Google Scholar] [CrossRef] [PubMed]
- Lui, S.; de Souza, A.; Sharma, A.; Fairbairn, J.; Schreiber, R.; Armstrong, K.; Blydt-Hansen, T. Physical activity and its correlates in a pediatric solid-organ transplant population. Pediatr. Transplant. 2020, 24, e13745. [Google Scholar] [CrossRef] [PubMed]
- Hamiwka, L.A.; Cantell, M.; Crawford, S.; Clark, C.G. Physical activity and health related quality of life in children following kidney transplantation. Pediatr. Transplant. 2009, 13, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C.; So, S.; DeAngelis, M.; Ghent, E.; Southmayd, D.; Carpenter, C. Physical activity experiences in children post-liver transplant: Developing a foundation for rehabilitation interventions. Pediatr. Transplant. 2018, 22, e13179. [Google Scholar] [CrossRef] [PubMed]
- Voss, C.; Ogunleye, A.A.; Sandercock, G.R. Physical Activity Questionnaire for children and adolescents: English norms and cut-off points. Pediatr. Int. 2013, 55, 498–507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 25 November 2020).
- Palermi, S.; Sacco, A.M.; Belviso, I.; Romano, V.; Montesano, P.; Corrado, B.; Sirico, F. Guidelines for Physical Activity-A Cross-Sectional Study to Assess Their Application in the General Population. Have We Achieved Our Goal? Int. J. Environ. Res. Public Health 2020, 17, 3980. [Google Scholar] [CrossRef]
- Akber, A.; Portale, A.A.; Johansen, K.L. Pedometer-assessed physical activity in children and young adults with CKD. Clin. J. Am. Soc. Nephrol. 2012, 7, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Tudor-LockTudor-Locke, C.; Craig, C.L.; Beets, M.W.; Belton, S.; Cardon, G.M.; Duncan, S.; Hatano, Y.; Lubans, D.R.; Olds, T.S.; Raustorp, A.; et al. How many steps/day are enough for children and adolescents? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 78. [Google Scholar] [CrossRef] [Green Version]
- Masajtis-Zagajewska, A.; Muras, K.; Nowicki, M. Effects of a Structured Physical Activity Program on Habitual Physical Activity and Body Composition in Patients with Chronic Kidney Disease and in Kidney Transplant Recipients. Exp. Clin. Transplant. 2019, 17, 155–164. [Google Scholar] [CrossRef]
- Roi, G.S.; Mosconi, G.; Totti, V.; Angelini, M.L.; Brugin, E.; Sarto, P.; Merlo, L.; Sgarzi, S.; Stancari, M.; Todeschini, P.; et al. Renal function and physical fitness after 12-mo supervised training in kidney transplant recipients. World J. Transplant. 2018, 8, 13–22. [Google Scholar] [CrossRef]
- Chinapaw, M.J.; Mokkink, L.B.; Van Poppel, M.N.M.; van Mechelen, W.; Terwee, C.B. Physical Activity Questionnaires for Youth. Sport. Med. 2010, 40, 539–563. [Google Scholar] [CrossRef] [PubMed]
- Crocker, P.R.E.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sport. Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.L.; Upton, D. Psychometric properties of the physical activity questionnaire for older children (PAQ-C) in the UK. Psychol. Sport Exerc. 2014, 15, 280–287. [Google Scholar] [CrossRef]
- Voss, C.; Harris, K.C. Physical activity evaluation in children with congenital heart disease. Heart 2017, 103, 1408–1412. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.; Faulkner, R.A. Validation of the Physical Activity Questionnaire for Older Children. Pediatr. Exerc. Sci. 1997, 9, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Venetsanou, F.; Emmanouilidou, K.; Soutos, K.; Sotiriou, S.A.; Bastida, L.; Moya, A.; Kambas, A. Towards a Functional Approach to the Assessment of Daily Life Physical Activity in Children: Are the PAQ-C and Fitbit Flex-2 Technically Adequate? Int. J. Environ. Res. Public Health 2020, 17, 8503. [Google Scholar] [CrossRef]
- Bervoets, L.; Van Noten, C.; Van Roosbroeck, S.; Hansen, D.; Van Hoorenbeeck, K.; Verheyen, E.; Van Hal, G.; Vankerckhoven, V. Reliability and Validity of the Dutch Physical Activity Questionnaires for Children (PAQ-C) and Adolescents (PAQ-A) Arch. Public Health 2014, 72, 47. [Google Scholar]
- Schmidt, M.D.; Cleland, V.J.; Thomson, R.J.; Dwyer, T.; Venn, A.J. A comparison of subjective and objective measures of physical activity and fitness in identifying associations with cardiometabolic risk factors. Ann. Epidemiol. 2008, 18, 378–386. [Google Scholar] [CrossRef]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P.R. Subjective versus Objective Measure of Physical Activity: A Systematic Review and Meta-Analysis of the Convergent Validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public Health 2021, 18, 3413. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Question | Response Scored 1 | Response Scored 2 | Response Scored 3 | Response Scored 4 | Response Scored 5 |
|---|---|---|---|---|---|
| 1. Physical activity in your spare time: Have you done any of the following activities in the past 7 days (last week)? If yes, how many times? | No | 1–2 | 3–4 | 5–6 | 7 times or more |
| 2. In the last 7 days, during your physical education (PE) classes, how often were you very active (playing hard, running, jumping, throwing)? | I don’t do PE | Hardly ever | Sometimes | Quite often | Always |
| 3. In the last 7 days, what did you do most of the times at the access? | Sat down (talking, reading, doing schoolwork) | Stood around or walked around | Ran or played a little bit | Ran around and played quite a bit | Ran and played hard most of the time |
| 4. In the last 7 days, what did you normally do at lunch (besides eating lunch)? | Sat down (talking, reading, doing schoolwork) | Stood around or walked around | Ran or played a little bit | Ran around and played quite a bit | Ran and played hard most of the time |
| 5. In the last 7 days, on how many days right after school, did you do sports, dance, or play games in which you were very active? | None | 1 time last week | 2 or 3 times last week | 4 times last week | 5 times last week |
| 6. In the last 7 days, on how many evenings did you do sports, dance, or play games in which you were very active? | None | 1 time last week | 2 or 3 times last week | 4 or 5 last week | 6 or 7 times last week |
| 7. On the last weekend, how many times did you do sports, dance, or play games in which you were very active? | None | 1 time | 2 or 3 times | 4 or 5 times | 6 or more times |
| 8. Which one of the following describes you best for the last 7 days? | All or most of my free time was spent doing things that involve little physical effort | I sometimes (1–2 times last week) did physical things in my free time (e.g., played sports, went running, swimming, bike riding, did aerobics) | I often (3–4 times last week) did physical things in my free time | I quite often (5–6 times last week) did physical things in my free time | I very often (7 or more times last week) did physical things in my free time |
| 9. Mark how often you did physical activity (like playing sports, games, doing dance, or any other physical activity) for each day last week | None | Little bit | Medium | Often | Very often |
| 10. Were you sick last week, or did anything prevent you from doing your normal physical activities? | Non-evaluable score | Non-evaluable score | Non-evaluable score | Non-evaluable score | Non-evaluable score |
| Mean ± SD/Number | |
|---|---|
| Male | 21 |
| Female | 28 |
| Age (years) | 13.3 ± 3.5 |
| Body Mass Index (kg/m2) | 20 ± 3.6 |
| Liver Transplantation | 32 |
| Kidney Transplantation | 15 |
| Combined Liver + Kidney Transplantation | 2 |
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| Question 2 (PE classes) | 33% | 0% | 20% | 24% | 22% |
| Question 3 (recess) | 37% | 37% | 12% | 14% | 0% |
| Question 4 (lunch time) | 53% | 27% | 8% | 12% | 0% |
| Question 5 (afternoon) | 16% | 14% | 45% | 10% | 14% |
| Question 6 (evening) | 45% | 14% | 29% | 6% | 6% |
| Question 7 (weekend) | 41% | 31% | 14% | 8% | 6% |
| Question 8 (self-perception) | 24% | 27% | 24% | 16% | 8% |
| Mean | 36% | 21% | 22% | 13% | 8% |
| St. Dev. | 12% | 12% | 12% | 6% | 8% |
| Variables | n | Mean | S.D. | Min | 0.25 | Mdn | 0.75 | Max |
|---|---|---|---|---|---|---|---|---|
| Male | 21 | 2.51 | 0.89 | 1.00 | 1.90 | 2.30 | 3.10 | 4.40 |
| Female | 28 | 2.34 | 0.86 | 1.00 | 1.80 | 2.30 | 2.70 | 4.10 |
| <14 years old | 27 | 2.54 | 0.86 | 1.10 | 1.80 | 2.60 | 3.10 | 4.40 |
| ≥14 years old | 22 | 2.26 | 0.87 | 1.00 | 1.80 | 2.30 | 2.30 | 4.10 |
| Liver Tx | 32 | 2.54 | 0.95 | 1.00 | 1.80 | 2.55 | 3.25 | 4.40 |
| Kidney Tx | 15 | 2.17 | 0.68 | 1.00 | 1.80 | 2.00 | 2.50 | 3.40 |
| Combined LTx + KTx | 2 | 2.30 | 0.0 | 2.30 | 2.30 | 2.30 | 2.30 | 2.30 |
| <5 years from Tx | 24 | 2.40 | 0.85 | 1.00 | 1.80 | 2.30 | 3.10 | 4.40 |
| ≥5 years from Tx | 25 | 2.43 | 0.90 | 1.00 | 1.80 | 2.30 | 2.90 | 4.10 |
| Underweight | 18 | 2.67 | 0.80 | 1.30 | 2.00 | 2.70 | 3.10 | 4.40 |
| Normal weight | 26 | 2.32 | 0.94 | 1.00 | 1.50 | 2.30 | 2.90 | 4.10 |
| Overweight | 5 | 2.02 | 0.43 | 1.50 | 1.80 | 1.90 | 2.30 | 2.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tranchita, E.; Cafiero, G.; Giordano, U.; Guzzo, I.; Labbadia, R.; Palermi, S.; Cerulli, C.; Candusso, M.; Spada, M.; Ravà, L.; et al. Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move. Int. J. Environ. Res. Public Health 2023, 20, 990. https://doi.org/10.3390/ijerph20020990
Tranchita E, Cafiero G, Giordano U, Guzzo I, Labbadia R, Palermi S, Cerulli C, Candusso M, Spada M, Ravà L, et al. Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move. International Journal of Environmental Research and Public Health. 2023; 20(2):990. https://doi.org/10.3390/ijerph20020990
Chicago/Turabian StyleTranchita, Eliana, Giulia Cafiero, Ugo Giordano, Isabella Guzzo, Raffaella Labbadia, Stefano Palermi, Claudia Cerulli, Manila Candusso, Marco Spada, Lucilla Ravà, and et al. 2023. "Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move" International Journal of Environmental Research and Public Health 20, no. 2: 990. https://doi.org/10.3390/ijerph20020990
APA StyleTranchita, E., Cafiero, G., Giordano, U., Guzzo, I., Labbadia, R., Palermi, S., Cerulli, C., Candusso, M., Spada, M., Ravà, L., Gentili, F., Drago, F., & Turchetta, A. (2023). Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move. International Journal of Environmental Research and Public Health, 20(2), 990. https://doi.org/10.3390/ijerph20020990