
Spatial Accessibility and Equity Evaluation of Medical Facilities Based on Improved 2SFCA: A Case Study in Xi’an, China

Abstract
:1. Introduction
2. Methods and Data Source
2.1. Accessibility Measurements: Two-Step Floating Catchment Area (2FSCA)
2.2. Optimize the Two-Step Floating Catchment Area
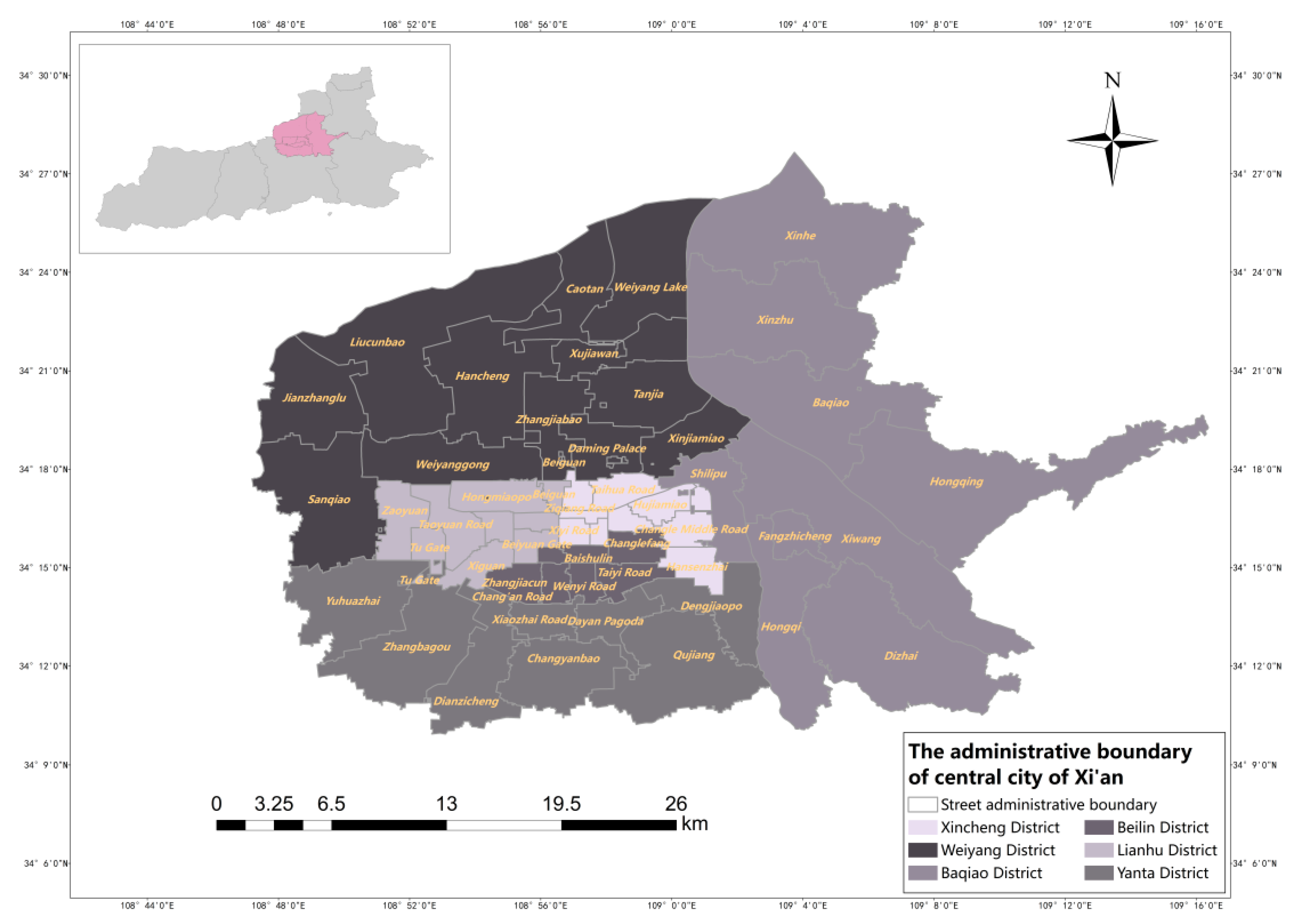
2.3. Overview of the Study Area
2.4. Data acquisition and Preprocessing
2.4.1. Medical Facility Data
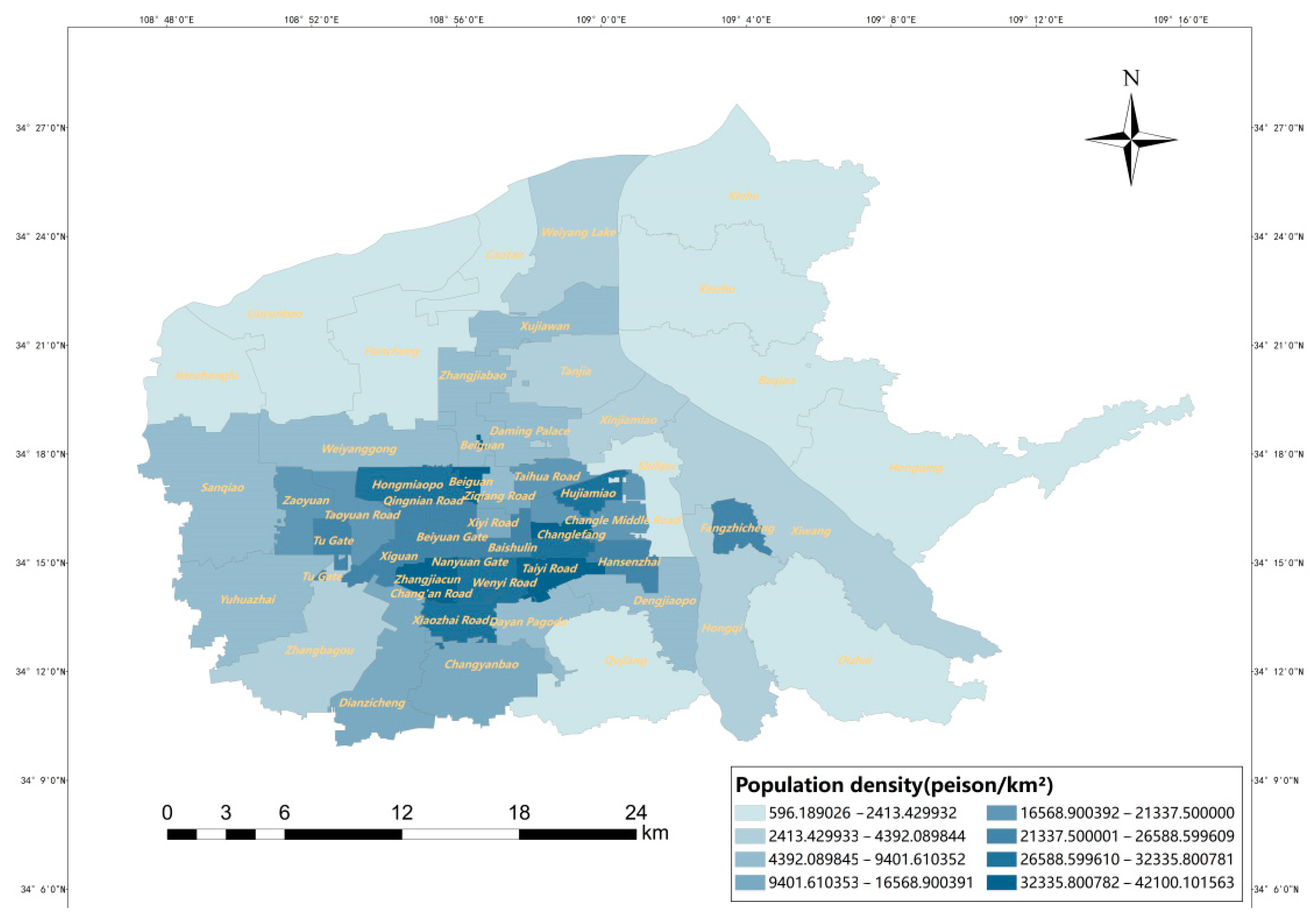
2.4.2. Population Data
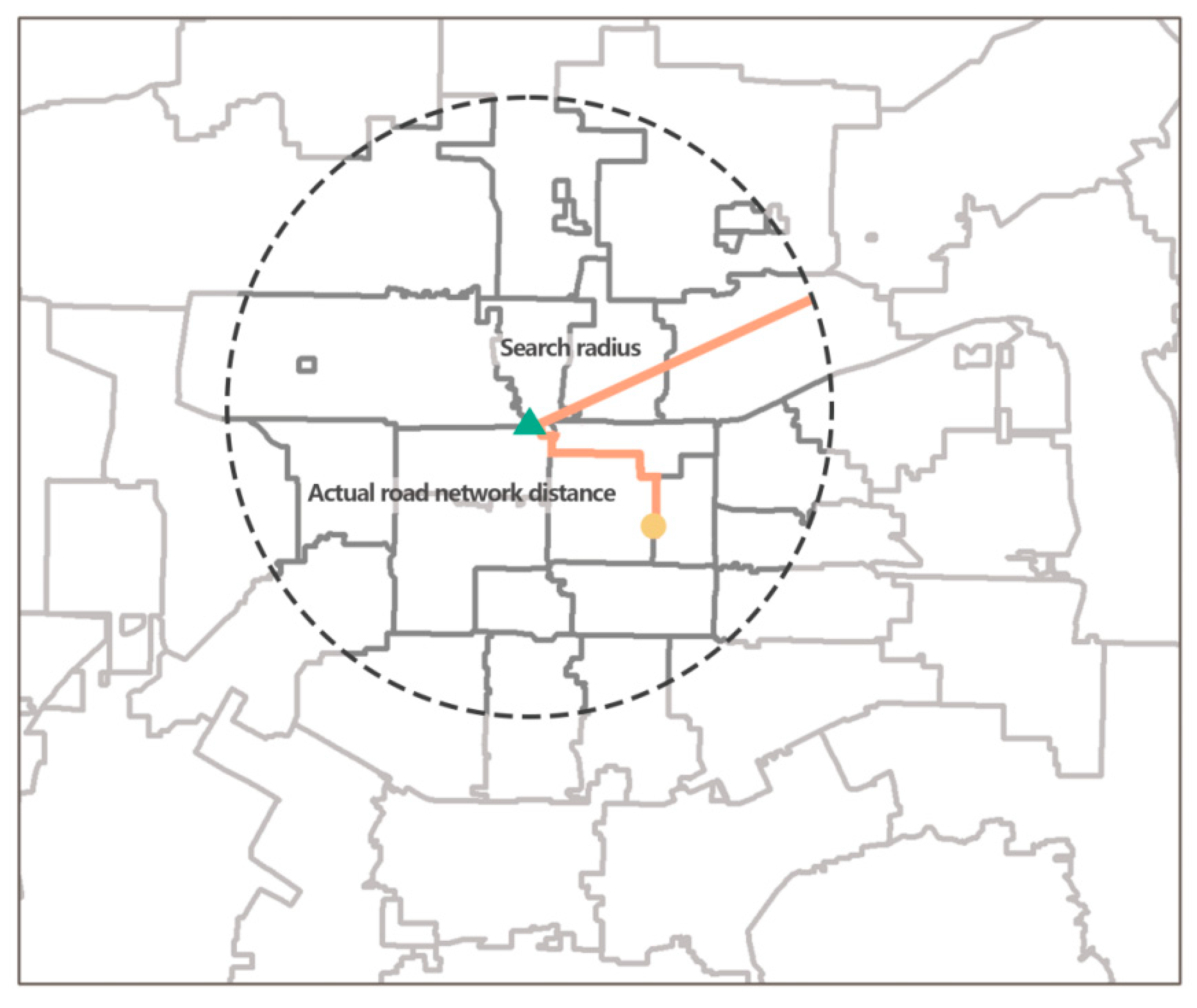
2.4.3. Obtaining Actual Transportation Costs
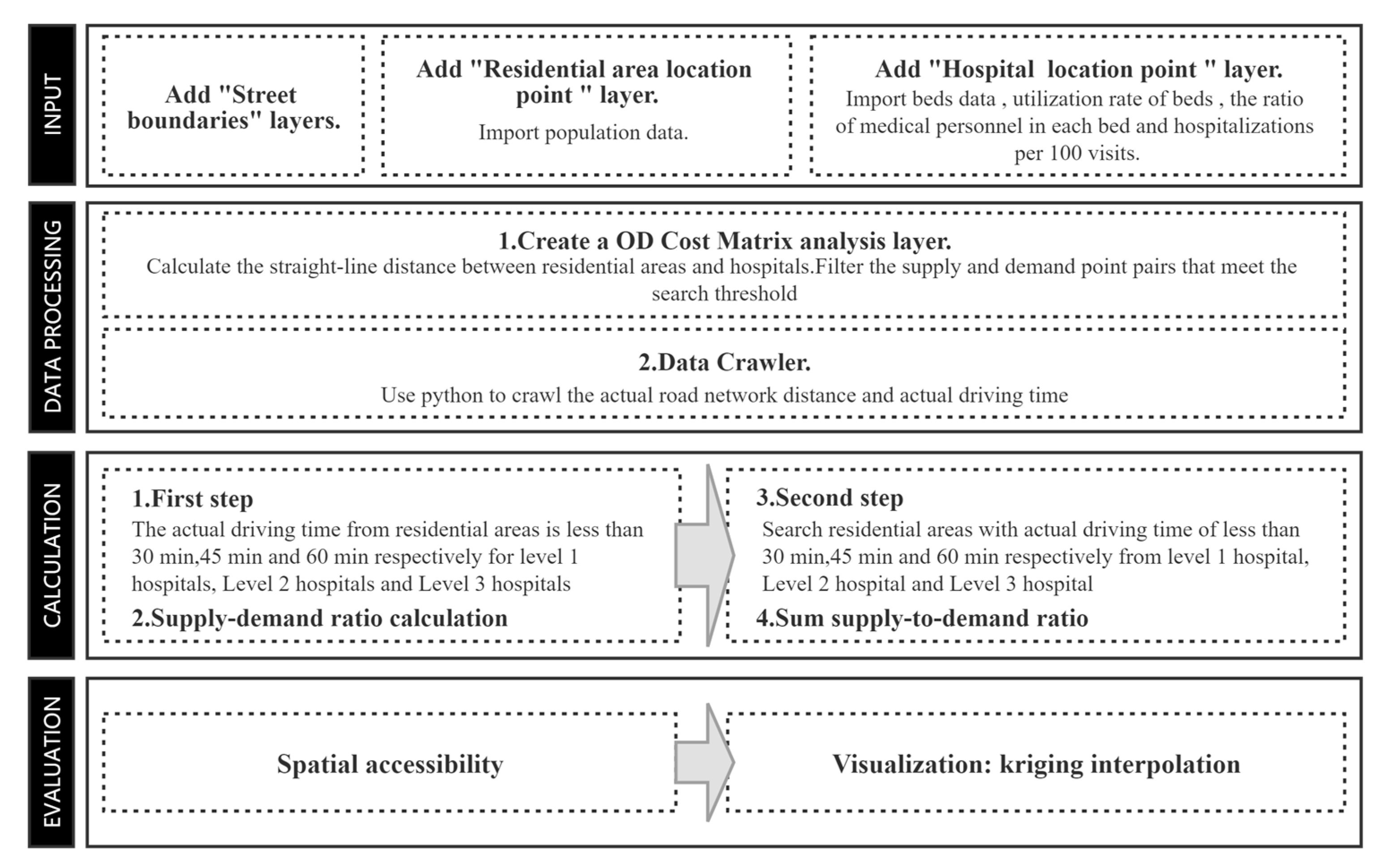
2.5. Technical Process
3. Results
3.1. Case Study
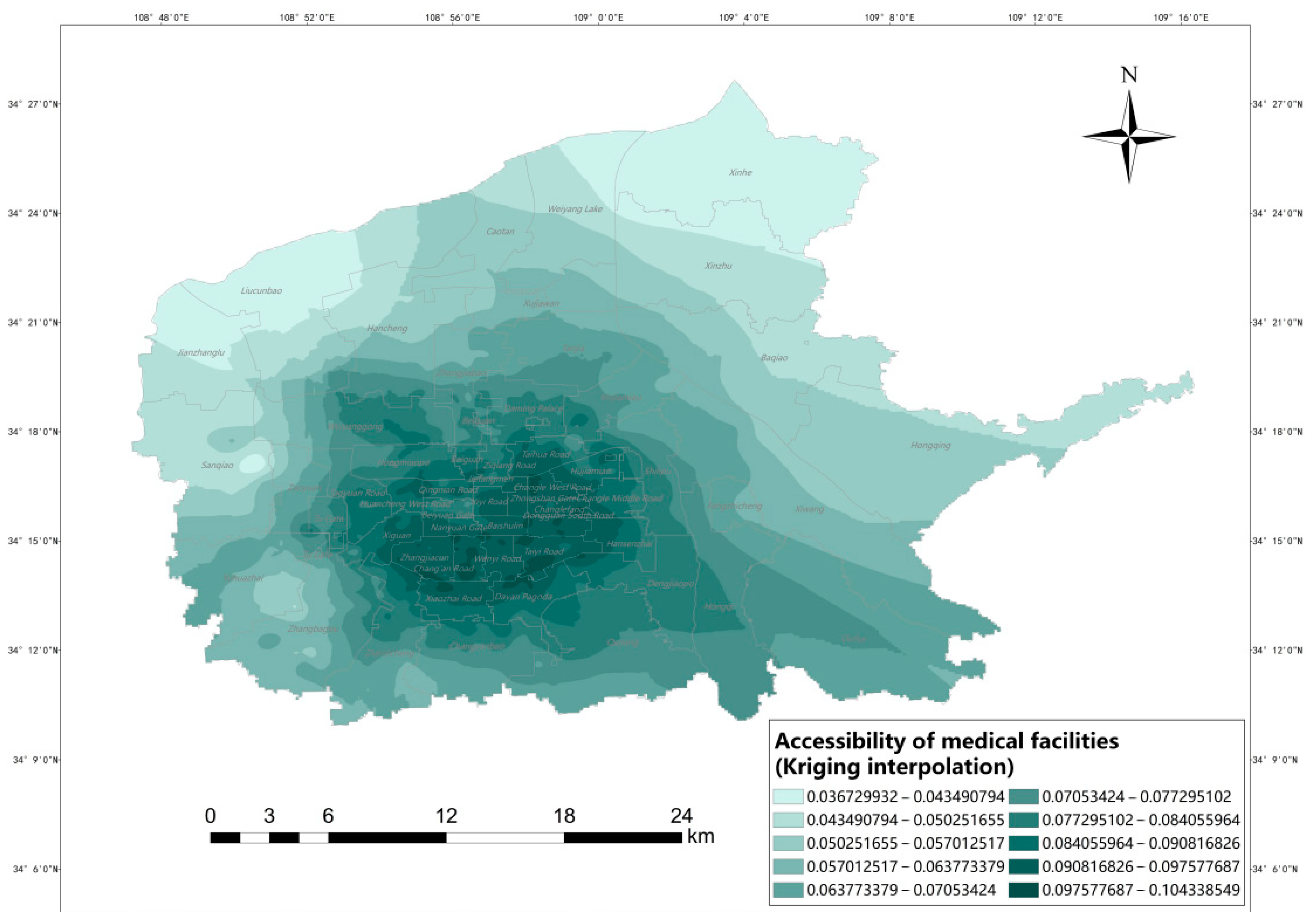
3.1.1. Analysis of Accessibility from a Spatial Perspective
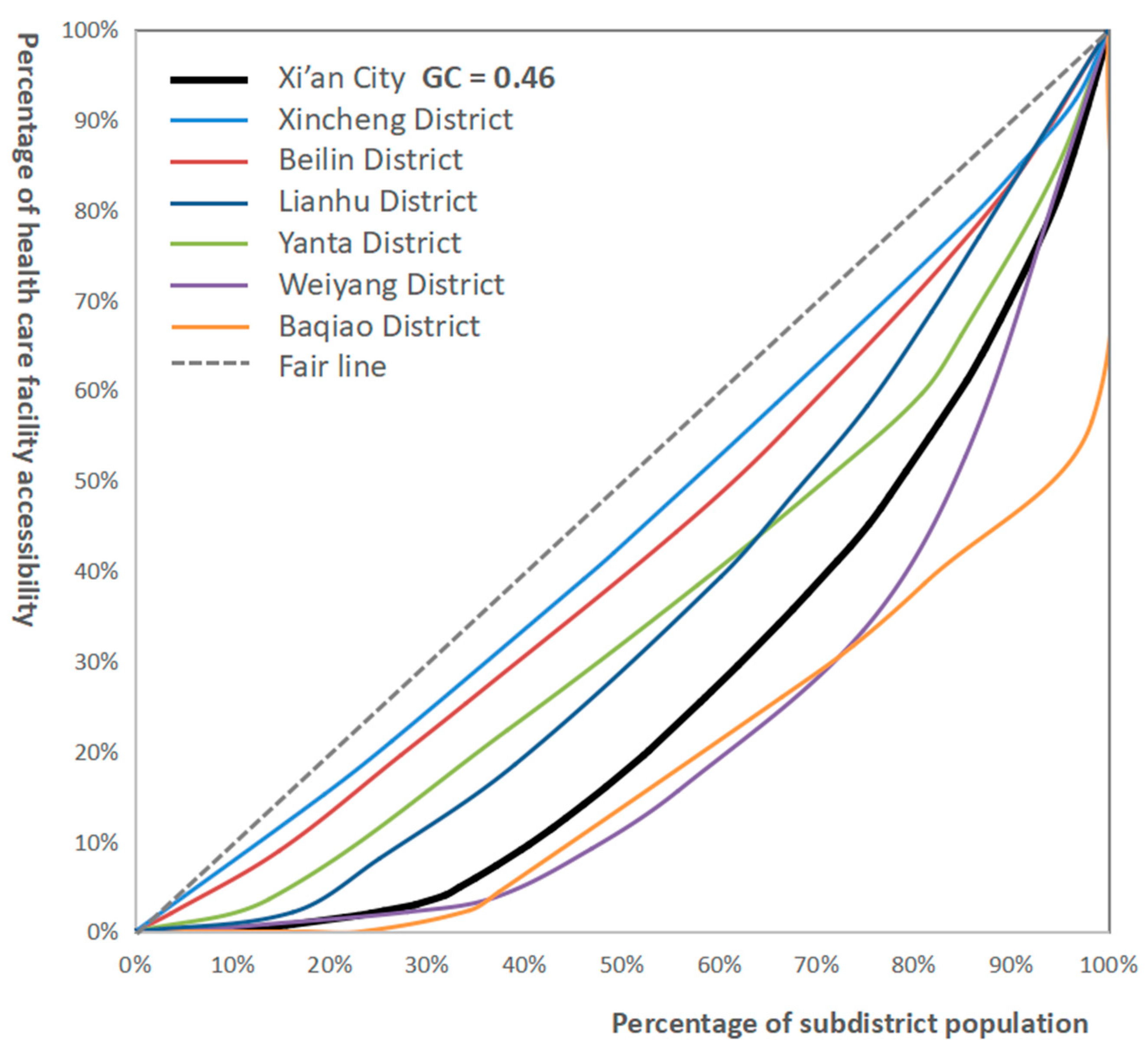
3.1.2. Analyzing Accessibility from a Data Perspective
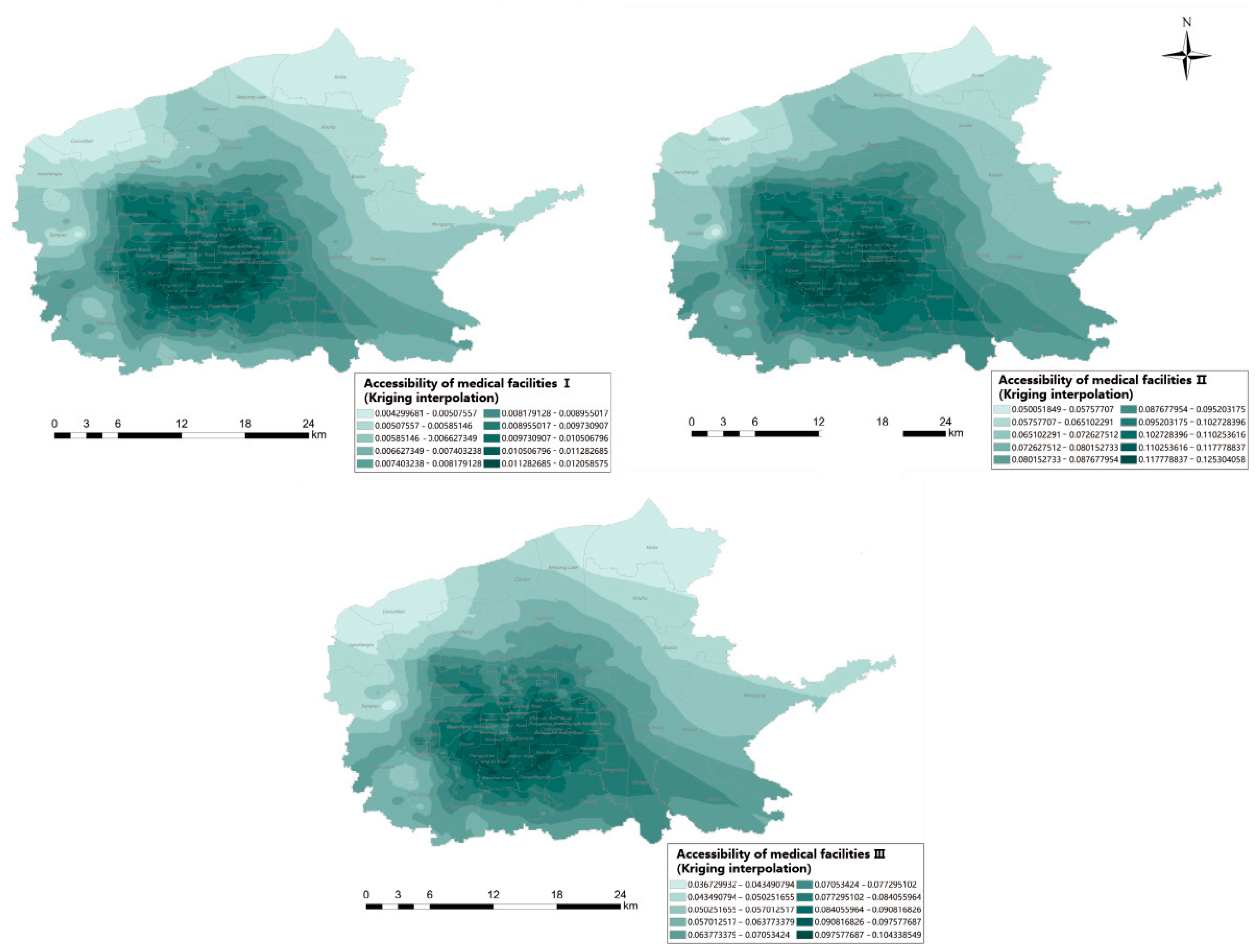
3.2. Model Comparison
4. Discussion
4.1. Advantages of the Improved Model
4.2. Shortcomings of the Improved Model
4.3. Policy Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.Q. Study on the Accessibility of Medical Facilities in the Main City of Xi’an. Master’s Thesis, Northwest Normal University, Lanzhou, China, 2021. [Google Scholar]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Appl. Geogr. 2014, 54, 182–188. [Google Scholar] [CrossRef]
- Cromley, E.K.; Shannon, G.W. Locating ambulatory medical care facilities for the elderly. Health Serv. Res. 1986, 21, 499–514. [Google Scholar] [PubMed]
- Hu, R.S.; Dong, S.C.; Hu, H. A two-step mobile search method for spatial accessibility analysis of medical services: The case of Donghai County, Jiangsu Province. Adv. Geogr. Sci. 2012, 31, 1600–1607. [Google Scholar]
- Hansen, W.G. How Accessibility Shapes Land Use. J. Am. Inst. Plan. 1959, 25, 73–76. [Google Scholar] [CrossRef]
- Song, Z.N.; Chen, W.; Zhang, G.X.; Zhang, L. Spatial accessibility of public service facilities and its metrics. Prog. Geogr. 2010, 29, 1217–1224. [Google Scholar]
- Yang, W.L.; Chen, N.; Wang, H.M.; Yang, W.X.; Xia, C.P. Research on accessibility of medical facilities in central Shanghai based on improved 2SFCA. Geomat. World 2020, 27, 75–79. [Google Scholar]
- Tao, Y.H.; Shen, Y. Spatial differences in accessibility of medical facilities and their influencing factors—A comparison based on household and mobile populations in Shanghai. Prog. Geogr. 2018, 37, 1075–1085. [Google Scholar]
- Li, Z.K.; Bu, P.; Fang, J.; Ma, K.S.; Chen, A.M. Evaluation of accessibility of medical services based on improved gravity model. Econ. Geogr. 2018, 38, 83–88. [Google Scholar]
- Tian, L.L.; Zhang, J.; Wang, F.H.; Li, X.; Zheng, W.S.; Luo, J. Study on the spatial optimization of rural public medical resources under the orientation of equity and efficiency: The case of Xiantao City, Hubei Province. Sci. Geogr. Sin. 2019, 39, 1455–1463. [Google Scholar]
- Mark, G. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Dai, D.; Wang, F. Geographic disparities in accessibility to food stores in southwest Mississippi. Environ. Plan. B Plan. Des. 2011, 38, 659–677. [Google Scholar] [CrossRef]
- Luo, W.; Whippo, T. Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health Place 2012, 18, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.L.; Cheng, Y.; Dai, T.Q. Evaluation of spatial accessibility of elderly facilities in Beijing. Adv. Geogr. Sci. 2014, 33, 616–624. [Google Scholar]
- Jamtsho, S.; Corner, R.; Dewan, A. Spatio-Temporal Analysis of Spatial Accessibility to Primary Health Care in Bhutan. ISPRS Int. J. Geo-Inf. 2015, 4, 1584–1604. [Google Scholar] [CrossRef] [Green Version]
- Wan, N.; Zou, B.; Sternberg, T. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Luo, J. Integrating the Huff Model and Floating Catchment Area Methods to Analyze Spatial Access to Healthcare Services. Trans. GIS 2014, 18, 436–448. [Google Scholar] [CrossRef]
- Tian, M.; Yuan, L.; Guo, R.; Wu, Y.; Liu, X. Evaluations of Spatial Accessibility and Equity of Multi-Tiered Medical System: A Case Study of Shenzhen, China. Int. J. Environ. Res. Public Health 2022, 19, 3017. [Google Scholar] [CrossRef]
- Fransen, K.; Neutens, T.; De Maeyer, P.; Deruyter, G. A commuter-based two-step floating catchment area method for measuring spatial accessibility of daycare centers. Health Place 2015, 32, 65–73. [Google Scholar] [CrossRef]
- Tao, Z.; Wang, Q. Facility or Transport Inequality? Decomposing Healthcare Accessibility Inequality in Shenzhen, China. Int. J. Environ. Res. Public Health 2022, 19, 6897. [Google Scholar] [CrossRef]
- Xing, J.D.; Ng, S. Analyzing spatiotemporal accessibility patterns to tertiary healthcare services by integrating total travel cost into an improved E3SFCA method in Changsha, China. Cities 2022, 122, 103541. [Google Scholar] [CrossRef]
- Wu, J.; Zhou, Q. Analysis of the current status of spatio-temporal accessibility research. Mapp. Sci. 2018, 43, 58–64. [Google Scholar]
- Ji, Z.R.; Shu, C.F.; Huang, Q. Spatial accessibility of medical facilities based on GIS. Geospat. Inf. 2018, 16, 10–13. [Google Scholar]
- Radke, J.; Mu, L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Ann. GIS 2000, 6, 105–112. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Xuan, R.L.; Yang, L.Y. Hospital development from the perspective of hospital service radius. Chin. J. Hosp. Stat. 2006, 13, 267–269. [Google Scholar]
- Rich, R.C. Neglected Issues in the Study of Urban Service Distributions: A Research Agenda. Urban Stud. 1979, 16, 143–156. [Google Scholar] [CrossRef]
- Yeeun, K.; Young-Ji, B.; Hwasoo, Y. Enhancing healthcare accessibility measurements using GIS: A case study in Seoul, Korea. PLoS ONE 2018, 13, e0194849. [Google Scholar]
- Wang, Q. Accessibility Analysis of Medical Services in Shanghai Based on Improved Two-Step Moving Search Method. Master’s Thesis, Wuhan University, Wuhan, China, 2019. [Google Scholar]
- Tao, Z.L.; Cheng, Y. Research progress of two-step mobile search method and its extended form. Prog. Geogr. 2016, 35, 589–599. [Google Scholar]
- Yu, J.X.; Zhang, X.Q. Research on spatial accessibility of medical facilities based on service radius: An example from the main urban area of Xi’an. J. Shaanxi Norm. Univ. (Nat. Sci. Ed.) 2017, 45, 78–84. [Google Scholar]
- Liu, J.S.; Chen, H.; Yang, B.Y.; Wang, W.; Xiang, Y.; Zhao, C. Comparison of interpolation methods for annual mean precipitation in Hebei Province. Acta Ecol. Sin. 2009, 29, 3493–3500. [Google Scholar]
- Wu, T.Y.; Xia, Q.T.; Chen, Z. Spatial accessibility of elderly institutions based on improved potential model: An example from Fengxian District, Shanghai. J. East China Norm. Univ. 2022, 2022, 85–96. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interpolation Method | Corresponding Parameter | MEAN | RMSE |
|---|---|---|---|
| Trend | Linear | −0.045 | 5.384 |
| IDW | The power of the distance is 2 | 0.085 | 5.132 |
| Splines | Regular spline function | 0.064 | 4.536 |
| Kriging | Ordinary Kriging | −0.037 | 4.324 |
| Gini | 0–0.2 | 0.2–0.3 | 0.3–0.4 | 0.4–0.5 | 0.5–1 |
|---|---|---|---|---|---|
| Equity | Absolutely fair | Relatively fair | Relatively reasonable | A bit unfair | Very unfair |
| Administrative District | Gini Coefficient | Administrative District | Gini Coefficient |
|---|---|---|---|
| Xincheng District | 0.11 | Beilin District | 0.16 |
| Weiyang District | 0.55 | Lianhu District | 0.29 |
| Baqiao District | 0.62 | Yanta District | 0.29 |
| Different Models | Average Value | Minimum Value | Maximum Value | Standard Deviation |
|---|---|---|---|---|
| Ai (Before optimization) | 0.009880532 | 0 | 0.012077138 | 0.001442719 |
| Ai (Consider the Comprehensive supply quantity) | 0.106521123 | 0 | 0.125540356 | 0.012593554 |
| Ai (Consider the Comprehensive supply quantity and probability functions) | 0.083444099 | 0 | 0.104378067 | 0.012279903 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, L.; Zhao, Y.; Lyu, H.; Chen, S.; Tu, Y.; Huang, S. Spatial Accessibility and Equity Evaluation of Medical Facilities Based on Improved 2SFCA: A Case Study in Xi’an, China. Int. J. Environ. Res. Public Health 2023, 20, 2076. https://doi.org/10.3390/ijerph20032076
Liu L, Zhao Y, Lyu H, Chen S, Tu Y, Huang S. Spatial Accessibility and Equity Evaluation of Medical Facilities Based on Improved 2SFCA: A Case Study in Xi’an, China. International Journal of Environmental Research and Public Health. 2023; 20(3):2076. https://doi.org/10.3390/ijerph20032076
Chicago/Turabian StyleLiu, Linggui, Yi Zhao, Han Lyu, Sining Chen, Yuheng Tu, and Shuyun Huang. 2023. "Spatial Accessibility and Equity Evaluation of Medical Facilities Based on Improved 2SFCA: A Case Study in Xi’an, China" International Journal of Environmental Research and Public Health 20, no. 3: 2076. https://doi.org/10.3390/ijerph20032076