Abstract
The aim of this study was to assess the association of long-term exposure to particulate matter with aerodynamic diameter, PM2.5, PM10, NO2 and SO2 as well as CO, with lung adenocarcinoma (AD) in south-east Poland for the years from 2004 to 2014. The study group consisted of 4296 patients with lung adenocarcinoma and the level of selected pollutants. To analyse the data, a standard statistics for cohort data, that is a risk ratio (RR), was used. The dependencies occurring in the distribution of pollutants and cancer incidence were examined using Moran’s I correlation coefficient. The current study suggests that PM10, NO2 and SO2 exposure as an air pollutant may increase female lung adenocarcinoma incidence. In men, the increased risk of adenocarcinoma lung cancer is affected by SO2 and PM10. A high morbidity rate in urban areas and suburbs may be connected with commuting from moderately polluted living areas to highly polluted working areas.
Keywords:
air pollutants; morbidity; adenocarcinoma; lung cancer; Moran’s correlation; health impact 1. Introduction
Among the lung cancer risk factors, modified and non-modifiable factors can be distinguished. Cigarette smoking is an important risk factor in the aetiology of lung cancer. It has been well established throughout numerous epidemiological studies [1,2,3] and belongs to modifiable factors, such as passive smoking, and exposure to asbestos or radon. Among the non-modifiable factors, WHO indicates a personal or family history of lung cancer, previous lung radiotherapy and air pollution [4]. In the case of the latter, the risk is far less than the risk caused by smoking, but some researchers estimate that, worldwide, approximately five percent of all lung cancer deaths may be caused by outdoor air pollution [4]. There is scientific evidence of an increased incidence of respiratory, circulatory and cancer diseases due to exposure to various air pollutants, mainly to particles PM10, PM2.5 and their constituents [5,6,7,8] as well as to nitrogen dioxide (NO2) [9,10,11] or sulphur dioxide (SO2) [5,12]. Exogenous carbon monoxide (CO) is produced by the incomplete combustion of carbon-containing molecules. CO enters the circulatory system through the respiratory system, binding with haemoglobin in the blood, forming carboxyhaemoglobin (COHb); the affinity of haemoglobin for CO is much greater than for oxygen [13,14], which can cause hypoxia, despite the normal number of blood cells in the body [13,15]. Due to the fact that CO in the external environment is formed as a result of fuel combustion, it is one of the important elements of outdoor air pollution.
The most common types of lung cancer include squamous cell carcinoma (SCC), adenocarcinoma and small cell carcinoma (SCLC). Until the nineties of the twentieth century, SCC was the most common histologic subtype, particularly among men. Over the years, the situation has changed, causing an increase in the number of ADs and a simultaneous decrease in the number of cases of SCC. This trend has been observed in countries in North America, Europe and Asia [16,17]. However, the trend of the occurrence of lung cancer subtype depending on gender was maintained. Rates of AD relative to SCC and SCLC are greater in women [18]. As a result, the percentage of AD is increasing, and the incidence of lung cancer in women is also increasing.
Scientists from different parts of the world have conducted observations on the possible impact of long-term exposure to selected particles and gases of air pollutants on lung cancer and its variants [19,20,21,22,23,24,25]. Research is being conducted on the selective impact and the synergy effect between selected pollutants. Korean cohort studies observed a trend in the incidence of lung cancer, which has changed drastically in recent years. The first Korean study analysing the population of lung cancer patients, conducted in 1997, showed a significant prevalence of squamous cell carcinoma (44.7%) over adenoma (27.9%) [14]. In a re-examination ten years later, it turned out that the situation had changed drastically, as the majority of patients had the glandular type (48.8%). The second most common was squamous (27.2%). Studies have also shown differences in the incidence of lung cancer types depending on gender. The most common type of lung cancer in men is SCC and in women AD [26]. The increased affinity of the adenocarcinoma type in women has also been confirmed by other studies [27,28].
Most of the 50 most polluted cities in the European Union are located in Poland such as Cracow, Wroclaw or Warsaw [29]. Therefore, it is necessary to conduct observations and research on the levels of atmospheric air pollution and their harmful impact on public health, especially respiratory diseases.
The purpose of this project was to evaluate the effects of long-term exposure to outdoor air pollution PM2.5, PM10, NO2, and SO2 as well as CO at the place of residence on the morbidity of lung adenocarcinoma in south-east Poland.
Based on the aim of this work, the research questions were posed:
- (1)
- What is the incidence of adenocarcinoma of the lung in relation to gender?
- (2)
- Is there a relationship between the incidence of adenocarcinoma of the lung and the individual components of air pollution in the analysed area?
- (3)
- Is there a trend in the morbidity of adenocarcinoma cancer in a ten-year follow-up?
2. Materials and Methods
2.1. Lung Cancer and Pollution Data
To examine the relationship between long-term exposure to selected concentrations of air pollution at the place of residence and the incidence of lung adenocarcinoma, original pollution maps were created with the places of residence marked. The source of data on incidence was the report of morbidity of lung cancer from Clinical Voivodship Hospital number 1 in Rzeszów from 2004 to 2014. The number of all lung cancer cases registered in the indicated period was 10,993. Research group included 4296 patients with AD. The subjects were divided by gender, as in recent years there was a tendency to a higher incidence of AD in women [26,27,28,29,30]. The age was also divided. The source of data on SO2, NO2, PM10, PM2.5 and CO pollution was hourly data from pollution measuring stations located in the Podkarpackie Voivodship in 2005–2014 from the Voivodship Inspectorate for Environmental Protection. The lack of source data in small areas was supplemented based on the average annual values determined from the OS-1 report for a given area. An autoregressive model with an exogenous variable [28] was created for each station. The residences of patients with adenocarcinoma of the lung were superimposed on the spatial maps of air pollution created in this way. The results obtained made it possible to determine the level of influence of air pollutants considered selectively and their combinations on the incidence of lung adenocarcinoma of the province of lung in the Podkarpackie in the years 2004–2014.
2.2. Data Analysis
The dependencies occurring in the distribution of pollutants and cancer incidence were examined using Moran’s I correlation coefficient [31]. This coefficient allows to assess the spatial autocorrelation, that is the relationship between the value of variable in a given grid cell in relation to the value of the variable in the neighbouring grid cells. The use of Moran’s I statistics is used for the identification of spatial clusters. Moran’s I correlation coefficient is given by
where: —indices of spatial units; —row-standardized matrix of spatial weights; —the variable of interest, —mean of .
If Moran’s I is close to one, then units tend to form spatial clusters. Opposite value can be interpreted as high local variability of variable of interest. No spatial pattern is indicated by Moran’s I close to zero.
Spatial analysis was carried out under assumption of Queen contiguity [32] (more neighbourhoods); that is, two cells are neighbours if they have at least one common point.
Finally, we used a risk ratio (RR), which is the ratio of the incidence rate in the exposed group and the incidence rate in the control group [27]. The exposed group are inhabitants of an area of above-average levels of particular pollutants, that is PM2.5, PM10, NO2, SO2 and CO, respectively. Confidence interval for RR was calculated and it was tested if RR was significantly different from 1 [33].
3. Results
The region has many urbanised areas in the central and western part. The southern part is low urbanised due to mountains. The eastern part is dominated by woods and is located close to the state border. The next choropleth confirms the general expectation that cancer incidences are correlated with the pollutant level. Nevertheless, there are areas where there are cancer incidences but quite low levels of pollutants and vice versa. Therefore we applied several tools to quantify this phenomenon.
An analysis of the dependency between pollutants and cancer incidences was carried out in two ways: comparing the variables within a grid cell and comparing them with neighbouring grid cells. The places of residence of patients with lung adenocarcinoma were superimposed on the created spatial map of air pollution. The figure above shows the choropleth for NO2 (Figure 1). The map shows the area of the Podkarpackie Voivodeship, which is located in the south-eastern part of Poland, on a scale of 1:1,500,000. The area is divided into 21 counties and 4 cities.
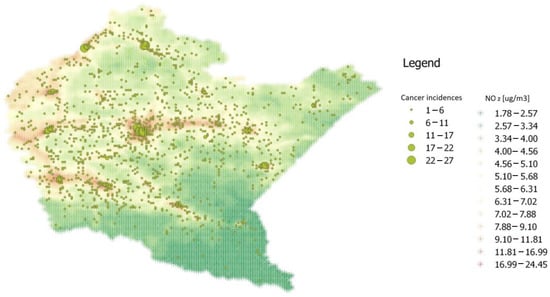
Figure 1.
Choropleth of cancer incidences and NO2 pollution levels.
The table below shows Moran’s I correlation coefficient and the p-value of its significance test (Table 1).

Table 1.
Moran I statistics for air pollution and cancer incidences.
For each analysed variable, there is a significant positive spatial autocorrelation but of low strength. Large grid clusters of low levels of pollutants in non-urban areas occur. Urban areas are very inhomogeneous with respect to the level of pollutants. Such a result is partially confirmed by the fact that the distribution of each pollutant reveals a high right-skewness and, in a case of cancer incidences, a very high right-skewness. Pollutants also reveal a much higher variability in urban areas in comparison to non-urban areas. The standard deviation of the pollutant level in urban areas is twice as much as in non-urban areas. Moreover, in the first case, the distribution has a heavy right tail (Figure 2).
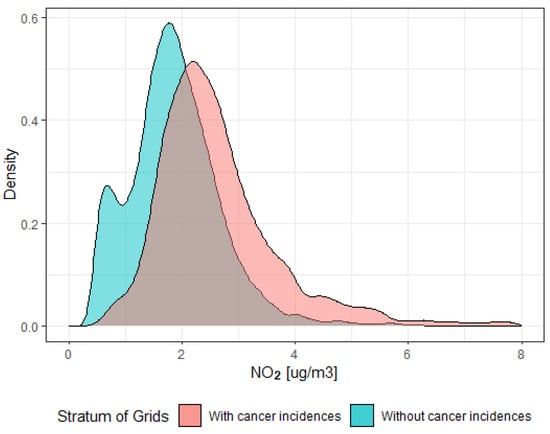
Figure 2.
Distribution of NO2 pollution level.
The study area was divided into below-average and above-average areas of pollution, respectively, for each pollution. In the next step, the people living in these areas were evaluated and broken down by age (below 75 and older) as well as by gender. The division into such age groups resulted from the median age of the people in the cancer incidence database.
In the group of patients under 75 years of age, the impact of air pollution on the incidence of AD of the lung was observed to a greater extent in women, especially in relation to SO2, NO2 and PM10. In contrast to women, no exposure to NO2 was observed in men (Table 2).
Table 2.
Risk ratio for the group below 75 years of age.
The analysis showed that the older group is exposed to the carcinogenic effects of all the analysed air pollutants, regardless of gender (Table 3).
Table 3.
Risk ratio for the group over 75 years of age.
4. Discussion
In 2013 the International Agency for Research on Cancer classified outdoor air pollution as carcinogenic to humans [34]. Worldwide, it has been estimated that 6% of all lung cancer deaths are attributable to ambient air pollution [35].
The subject of research all over the world is the analysis and attempt to determine the impact of long-term exposure to particulate matter in the air on the incidence of lung cancer [19,20,21,22,23,24,25]. The available results are not conclusive. Long-term observations of the impact of exposure to air pollution and their assessment as a carcinogen increase the value of research. This study assessed the relationship between long-term exposure to various air pollutants in the place of residence and the occurrence of lung adenocarcinoma in adult Poles in south-eastern Poland.
An analysis of pollutants was carried out in two ways: comparing within a grid cell and comparing with neighbouring grid cells with an accuracy of 1 km2. Several patterns of spatial distribution of pollutants were discovered with the use of the pollution model, standard and spatial correlation coefficient, and density estimation. There are large areas with a stable low level of all pollutants, mostly rural areas. Cancer incidences seem to not be connected with pollutants. Next there are urban areas with very unstable and high levels of pollutants, which quite quickly decreases the levels of pollutants in the suburbs. The third type are industrial areas with industries that spread pollution over a large neighbourhood. The impact of these pollutant sources on cancer incidences is visible in neighbouring rural areas. New industrial zones are being created in the study area. These observations and further research may influence the creation of a certain border zone separating rural areas adjacent to industrial areas, creating a potential protective zone, not inhabited by society.
AD is the most common histological type of lung cancer in the population [15], with higher rates of AD occurring in women, 189 cases [14,15]. Despite other factors influencing the disease, such as lifestyle, diet or climate change, a trend of increased incidence among women was also observed in the study group.
In the European Study of Cohorts for Air Pollution Effects, data were used from 17 cohort studies based in nine European countries, and the meta-analyses showed a statistically significant association between higher hazards of risk for lung cancer with higher exposures to PM2.5 and PM10. Higher results of PM2.5 and PM10 were stronger associated specifically with AD [36]. These studies confirmed the carcinogenic effect of PM10 particulate matter in the case of all respondents and PM2.5 only in the case of people over 75 years of age (Table 2 and Table 3).
Slightly different results were shown in the seven cohorts from Europe. The analysis showed that long-term exposure to PM2.5 in the place of residence can affect the growth of lung cancer morbidity [30]. These analyses verified the ten-year impact of exposure to selected air pollutants but did not show such a strong impact on the increase in the incidence of AD of the lung in the case of PM2.5. In the case of PM 2.5 for the cohort of men under the age of 75, the risk ratio was very close to 1; hence, it was not interpreted.
The contribution of traffic emissions to ambient air pollution is assessed as individual traffic-related pollutants such as NO2, PM2.5 and benzene. The NO2 level is often used as a marker for traffic-based air pollution [37,38]. In the European Study of Cohorts for Air Pollution Effects, the relationship between exposure to NO2 and the occurrence of lung cancer was not confirmed [36]. However, a more recent meta-analysis of 20 studies from different parts of the world reported consistent evidence for the association between NO2 and lung cancer. In Europe, there was a relative risk between exposure to NO2 and the morbidity of lung cancer [39]. Our previous work showed nitrogen dioxide to be a lung cancer carcinogen. Once NO2 is mixed with the other outdoor air pollution, it becomes more persistent in terms of explaining the appearance of cancers and could constitute the main cause of SCC [11]. For the cohort of men under the age of 75, the risk ratio was less than 1 in the case of NO2. Thus, an above-average level of NO2 did not lead to the higher risk of lung cancer. For all other pollutants and cohorts, the risk ratio was always greater than 1, indicating a higher risk of lung cancer for areas of above-average levels of pollutants.
The American Cancer Society Study and the Adventist Health Study indicate a strong relationship between SO2 exposure and increased lung cancer mortality [40,41,42]. This association was confirmed by studies conducted among non-smokers in California [42]. The results showed that lung cancer incidence was positively associated with interquartile range increases for SO2 in women. A particularly significant effect of SO2 on the incidence of lung adenocarcinoma in women was also confirmed by this study (Table 2 and Table 3).
Summing up the conducted causal analyses, it is worth emphasizing that scientific reports with such precise geolocation are rarely encountered, which increases the credibility of linking morbidity with its factors.
5. Conclusions
The provided scientific evidence may affect the health of the study population in the future in two ways. In terms of adenocarcinoma prophylaxis: by recommending more frequent check-ups in the risk areas of the Podkarpackie Voivodship with the highest concentrations of PM10, NO2 and SO2, and in particular in rural areas in close proximity to an industrial zone, or by recommending a change in residence due to a confirmed carcinogenic effect of the external environment. Thanks to the presented data and the created models enabling the identification of areas with the highest concentrations of selected pollutants, we can now identify those people most at risk of developing lung cancer, broken down by histological subtypes, gender and age.
The declining tendency in smoking points to the necessity of focusing on other risk factors. The analysis of these within the context of morbidity and mortality can help to develop more effective screening programs. The present study found significant associations between ambient air pollution and lung cancer.
The current study suggests that PM10, NO2 and SO2 exposure as air pollutants may increase female lung adenocarcinoma incidence. In men, the increased risk of adenocarcinoma lung cancer is affected by SO2 and PM10.
A high morbidity rate in urban areas and suburbs may be connected with commuting from moderately polluted living areas to highly polluted working areas.
Author Contributions
Conceptualization, J.G., M.C., M.C.-W. and S.W.; methodology, J.G., M.C.-W. and M.C.; software, M.C.-W.; validation, S.W.; formal analysis, M.C.-W. and S.W.; investigation, M.C.-W. and M.C.; resources, M.C.-W. and M.C.; writing—original draft preparation, J.G. and M.C.; writing—review and editing, M.C.-W visualization, M.C.-W. and S.W.; supervision, M.C.-W. and S.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bach, P.B.; Kattan, M.W.; Thornquist, M.D.; Kris, M.G.; Tate, R.C.; Barnett, M.J.; Hsieh, L.J.; Begg, C.B. Variations in lung cancer risk among smokers. J. Natl. Cancer Inst. 2003, 95, 470–478. [Google Scholar] [CrossRef]
- Vineis, P.; Airoldi, L.; Veglia, F.; Olgiati, L.; Pastorelli, R.; Autrup, H.; Dunning, A.; Garte, S.; Gormally, E.; Hainaut, P.; et al. Environmental tobacco smoke and risk of respiratory cancer and chronic obstructive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ 2005, 330, 277. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- World Health Organization. Outdoor Air Pollution Causes Cancer. Available online: http://www.cancer.org/cancer/news/world-health-organization-outdoor-air-pollution-causes-cancer (accessed on 10 November 2015).
- Hart, J.E.; Garshick, E.; Dockery, D.W.; Smith, T.J.; Ryan, L.; Laden, F. Long-term ambient multipollutant exposures and mortality. Am. J. Respir. Crit. Care Med. 2011, 183, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lepeule, J.; Laden, F.; Dockery, D.; Schwartz, J. Chronic exposure to fine particles and mortality: An extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environ. Health Perspect. 2012, 120, 965–970. [Google Scholar] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef]
- Chen, H.; Goldberg, M.S.; Villeneuve, P.J. A systematic review of the relation between long-term exposure to ambient air pollution and chronic diseases. Rev. Environ. Health 2008, 23, 243–297. [Google Scholar]
- Filleul, L.; Rondeau, V.; Vandentorren, S.; Le Moual, N.; Cantagrel, A.; Annesi-Maesano, I.; Charpin, D.; Declercq, C.; Neukirch, F.; Paris, C.; et al. Twenty five year mortality and air pollution: Results from the French PAARC survey. Occup. Environ. Med. 2005, 62, 453–460. [Google Scholar] [CrossRef]
- Bentayeb, M.; Wagner, V.; Stempfelet, M.; Zins, M.; Goldberg, M.; Pascal, M.; Larrieu, S.; Beaudeau, P.; Cassadou, S.; Eilstein, D.; et al. Association between long-term exposure to air pollution and mortality in France: A 25-year follow-up study. Environ. Int. 2015, 85, 5–14. [Google Scholar] [CrossRef]
- Gawełko, J.; Cierpiał-Wolan, M.; Bwanakare, S.; Czarnota, M. Association between Air Pollution and Squamous Cell Lung Cancer in South-Eastern Poland. Int. J. Environ. Res. Public Health 2022, 19, 11598. [Google Scholar] [CrossRef]
- Nyberg, F.; Gustavsson, P.; Järup, L.; Bellander, T.; Berglind, N.; Jakobsson, R.; Pershagen, G. Urban air pollution and lung cancer in Stockholm. Epidemiology 2000, 11, 487–495. [Google Scholar] [CrossRef]
- Toyoda, Y.; Nakayama, T.; Ioka, A.; Tsukuma, H. Trends in lung cancer incidence by histological type in Osaka, Japan. Jpn. J. Clin. Oncol. 2008, 38, 534–539. [Google Scholar] [CrossRef]
- Lortet-Tieulent, J.; Soerjomataram, I.; Ferlay, J.; Rutherford, M.; Weiderpass, E.; Bray, F. International trends in lung cancer incidence by histological subtype: Adenocarcinoma stabilizing in men but still increasing in women. Lung Cancer 2014, 84, 13–22. [Google Scholar] [CrossRef]
- Youlden, D.; Cramb, S.; Baade, P. The international epidemiology of lung cancer: Geographic distribution and secular trends. J. Thorac. Oncol. 2008, 3, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Moon, D.H.; Kwon, S.O.; Kim, S.Y.; Kim, W.J. Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 915. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.Y.; Huang, Y.C.; Su, S.Y.; Huang, J.Y.; Lai, C.H.; Lung, C.C.; Ho, C.C.; Liaw, Y.P. Cell type specificity of female lung cancer associated with sulfur dioxide from air pollutants in Taiwan: An ecological study. BMC Public Health 2012, 12, 4. [Google Scholar] [CrossRef]
- Lewis, D.R.; Check, D.P.; Caporaso, N.E.; Travis, W.D.; Devesa, S.S. US lung cancer trends by histologic type. Cancer 2014, 120, 2883–2892. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Franceschi, S.; La Vecchia, C.; Randimbison, L.; Te, V.C. Lung carcinoma trends by histologic type in Vaud and Neuchâtel, Switzerland, 1974–1994. Cancer 1997, 79, 906–914. [Google Scholar] [CrossRef]
- Tomášková, H.; Horáček, J.; Šlachtová, H.; Šplíchalová, A.; Riedlová, P.; Dalecká, A.; Jirák, Z.; Mad’ar, R. Analysis of Histopathological Findings of Lung Carcinoma in Czech Black Coal Miners in Association with Coal Workers’ Pneumoconiosis. Int. J. Environ. Res. Public Health 2022, 19, 710. [Google Scholar] [CrossRef] [PubMed]
- Linares, I.; Molina-Portillo, E.; Expósito, J.; Baeyens, J.A.; Suárez, C.; Sánchez, M.J. Trends in lung cancer incidence by histologic subtype in the south of Spain, 1985–2012: A population-based study. Clin. Transl. Oncol. 2016, 18, 489–496. [Google Scholar] [CrossRef]
- Meza, R.; Meernik, C.; Jeon, J.; Cote, M.L. Lung cancer incidence trends by gender, race and histology in the United States, 1973–2010. PLoS ONE 2015, 10, e0121323. [Google Scholar] [CrossRef]
- Lee, C.; Kang, K.H.; Koh, Y.; Chang, J.; Chung, H.S.; Park, S.K.; Yoo, K.; Song, J.S. Characteristics of lung cancer in Korea, 1997. Lung Cancer 2000, 30, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Jung, C.Y.; Cho, D.G.; Jeon, J.H.; Lee, J.E.; Ahn, J.S.; Kim, S.J.; Kim, Y.; Kim, Y.C.; Kim, J.E.; et al. Clinical Characteristics and Prognostic Factors of Lung Cancer in Korea: A Pilot Study of Data from the Korean Nationwide Lung Cancer Registry. Tuberc. Respir. Dis. 2019, 82, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Pauk, N.; Kubik, A.; Zatloukal, P.; Krepela, E. Lung cancer in women. Lung Cancer 2005, 48, 1–9. [Google Scholar] [CrossRef] [PubMed]
- World Bank Group. In the Spotlight. Air Quality in Poland, What Are the Issues and What Can be Done? 2019. Available online: https://documents1.worldbank.org/curated/en/426051575639438457/pdf/Air-Quality-in-Poland-What-are-the-Issues%02and-What-can-be-Done.pdf (accessed on 10 November 2022).
- Carneiro, I. Introduction to Epidemiology, 2nd ed.; Howard, N., Ed.; Open University Press: Berkshire, UK, 2011; p. 27. ISBN 978-0-335-24462-1. [Google Scholar]
- Shumway, R.H.; Stoffer, D.S.; Stoffer, D.S. Time Series Analysis and Its Applications: With R Examples, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2010; ISBN 144197864X. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef]
- Hvidtfeldt, U.A.; Severi, G.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bellander, T.; Boutron-Ruault, M.C.; Brandt, J.; Brunekreef, B.; Cesaroni, G.; et al. Long-term low-level ambient air pollution exposure and risk of lung cancer—A pooled analysis of 7 European cohorts. Environ. Int. 2021, 146, 106249. [Google Scholar] [CrossRef]
- Moran, P.A.P. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17. [Google Scholar] [CrossRef]
- Lloyd, C. Spatial Data Analysis: An Introduction for GIS Users; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Szklo, M.; Nieto, F.J. Epidemiology: Beyond the basics, 4th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2019; p. 488. ISBN 9781284116595. [Google Scholar]
- Straif, K.; Cohen, A.; Samet, J. IARC Scientific Publication No. 161: Air Pollution and Cancer; International Agency for Research on Cancer: Lyon, France, 2013.
- World Health Organization. Burden of Disease from Ambient Air Pollution for 2012; World Health Organization: Geneva, Switzerland, 2014.
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Brook, J.R.; Burnett, R.T.; Dann, T.F.; Cakmak, S.; Goldberg, M.S.; Fan, X.; Wheeler, A.J. Further interpretation of the acute effect of nitrogen dioxide observed in Canadian time-series studies. J. Expo. Sci. Environ. Epidemiol. 2007, 17 (Suppl. S2), S36–S44. [Google Scholar] [CrossRef]
- Valavanidis, A.; Fiotakis, K.; Vlachogianni, T. Airborne particulate matter and human health: Toxicological assessment and importance of size and composition of particles for oxidative damage and carcinogenic mechanisms. J. Environ. Sci. Health C Environ. Carcinog. Ecotoxicol. Rev. 2008, 26, 339–362. [Google Scholar] [CrossRef]
- Hamra, G.B.; Laden, F.; Cohen, A.J.; Raaschou-Nielsen, O.; Brauer, M.; Loomis, D. Lung cancer and exposure to nitrogen dioxide and traffic: A systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Abbey, D.E.; Nishino, N.; McDonnell, W.F.; Burchette, R.J.; Knutsen, S.F.; Lawrence Beeson, W.; Yang, J.X. Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am. J. Respir. Crit. Care Med. 1999, 159, 373–382. [Google Scholar] [CrossRef]
- Beeson, W.L.; Abbey, D.E.; Knutsen, S.F. Long-term concentrations of ambient air pollutants and incident lung cancer in California adults: Results from the AHSMOG study. Environ. Health Perspect. 1998, 106, 813–822. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).