Abstract
Introduction: Understanding the specific geospatial variations in childhood stunting is essential for aligning appropriate health services to where new and/or additional nutritional interventions are required to achieve the Sustainable Development Goals (SDGs) and national targets. Objectives: We described local variations in the prevalence of childhood stunting at the second administrative level and its determinants in Nigeria after accounting for the influence of geospatial dependencies. Methods: This study used the 2018 national Nigeria Demographic and Health Survey datasets (NDHS; N = 12,627). We used a Bayesian geostatistical modelling approach to investigate the prevalence of stunting at the second administrative level and its proximal and contextual determinants among children under five years of age in Nigeria. Results: In 2018, the overall prevalence of childhood stunting in Nigeria was 41.5% (95% credible interval (CrI) from 26.4% to 55.7%). There were striking variations in the prevalence of stunting that ranged from 2.0% in Shomolu in Lagos State, Southern Nigeria to 66.4% in Biriniwa in Jigawa State, Northern Nigeria. Factors positively associated with stunting included being perceived as small at the time of birth and experience of three or more episodes of diarrhoea in the two weeks before the survey. Children whose mothers received a formal education and/or were overweight or obese were less likely to be stunted compared to their counterparts. Children who were from rich households, resided in households with improved cooking fuel, resided in urban centres, and lived in medium-rainfall geographic locations were also less likely to be stunted. Conclusion: The study findings showed wide variations in childhood stunting in Nigeria, suggesting the need for a realignment of health services to the poorest regions of Northern Nigeria.
1. Introduction
Childhood malnutrition is a major global health concern that affects the growth and development of children and has long-lasting impacts into adulthood [1,2]. The causes of malnutrition are multi-faceted and interconnected, and include poverty, poor hygiene, limited access to nutritious food and healthcare, and infectious diseases [2,3,4,5]. Addressing malnutrition is important for improving health outcomes and breaking the cycle of poverty worldwide.
The United Nations General Assembly endorsed the Sustainable Development Goals (SDGs, including SDG-2.2: to end all forms of malnutrition by 2030) in 2015 [6]. The World Health Organisation member states endorsed the Global Nutrition Targets (GNTs; Target 1: to reduce the number of children under 5 who are stunted by 40% before 2025) in 2012 [7]. These efforts aim to identify priority areas for action and serve as catalysts for global change [6,8]. However, current reports indicate that an estimated 144 million children under 5 are stunted globally [9,10], and no African country (including Nigeria) is on track to achieve the SDGs and GNTs [10].
Nigeria is a multi-ethnic and culturally diverse country in the sub-Saharan region of West Africa, with an estimated population of over 210 million people [11]. In the past two decades, the country has made steady economic progress, with an increase in Growth Domestic Product (GDP) per capita income from USD 568 in 2000 to USD 2085 in 2021 [12]. Despite this economic growth, more than 40% of Nigerians still live in poverty, and childhood malnutrition (that is, stunting, wasting, and underweight) remains a huge public health challenge [13]. Recent reports have indicated that childhood malnutrition accounts for one out of three cases of mortality of children aged under 5 in Nigeria [13,14].
For the past two decades, there have been global, national, and subnational efforts to improve childhood malnutrition in Nigeria. Some of the programmes include the Millennium Development Goals [15], Nigeria’s National Policy on Food and Nutrition (MBNP, 2016) [16], and the Child Development Grant Programme in Northern Nigeria [17]. Many socioeconomic, agricultural, and health programmes have contributed to reducing the prevalence of childhood stunting in Nigeria (from 42.4% in 2003 to 36.8% in 2018) [13]. However, in 2021, the United Nations Children’s Fund (UNICEF) reported that approximately 12 million children were stunted in Nigeria, and the country accounted for 8% of the world’s stunted children [18].
Previously published studies conducted in Nigeria have shown that low maternal involvement in household decision making [19], a lack of parental formal education [20,21], child gender (male) [20,21], perceived birth size (small birth size) [22], low maternal body mass index (BMI, <18.5 kg/m2) [21], and household wealth (poorer households) [19,20,22] were associated with childhood stunting. Other significant factors included childhood diarrhoea [20,22], less-frequent antenatal visits [21], short breastfeeding duration (≤12 months) [19,22], and overcrowding [21]. While the previous studies provide a relevant description of the factors associated with stunting in Nigeria, the studies have limitations. Firstly, childhood malnutrition (including stunting) is often described as a geospatial public health issue [23]. In Nigeria, geography-specific variations in stunting have not been fully described, nor has there been an exploration of environmental and climatic factors (including temperature, rainfall, aridity, and urbanisation) associated with stunting in Nigeria. Secondly, none of the previous studies described detailed subnational estimates of stunting in Nigeria, as national data can often mask within-country geographic distribution [24]. Finally, understanding the geospatial variations in stunting can be the catalyst required to draw the attention of policy decision makers and public health experts to this chronic issue of stunting in Nigeria [25]. This measure can also increase efforts that aim to scale-up nutrition-specific interventions for Nigerian children and subsequently reduce malnutrition.
In 2020, the Federal Government of Nigeria launched the revised National Health Promotion Policy (NHP) [26], and it aims to deliver healthcare that is preventive, promotive, protective, restorative, and rehabilitative for every citizen, including improvement in childhood malnutrition. Findings from the current study would help determine high-priority geographic locations for targeted interventions needed to address Nigeria’s childhood stunting issue [26]. Furthermore, this study will be important in tracking progress at the subnational level in achieving the global nutritional agenda, including the SDGs [6] and GNTs [7] in Nigeria. The present study aims to (i) describe the prevalence of childhood stunting at the second administrative level in Nigeria, and (ii) to examine proximal and contextual factors associated with childhood stunting after accounting for the influence of geospatial dependencies.
2. Materials and Methods
2.1. Data Sources
The study was based on nationally representative data, the 2018 Nigeria Demographic and Health Survey (NDHS, N = 12,627). The National Population Commission (NPC) and the National Malaria Elimination Programme (NMEP) of the Federal Ministry of Health, Nigeria, implemented the survey. The 2018 NDHS was funded by the United States Agency for International Development (USAID), the Global Fund, Bill and Melinda Gates Foundation (BMGF), the United Nations Population Fund (UNFPA), and the World Health Organisation (WHO), with technical assistance from the Inner City Fund (ICF) International [13].
The Nigerian government structure is divided into 36 states and the Federal Capital Territory, Abuja. Each state is subdivided into a total of 774 local government areas (LGAs), and each LGA is divided into wards (the lowest administrative unit) [13]. The sample for the 2018 NDHS was selected using a two-stage stratified cluster sampling method, using 36 states and the Federal Capital Territory as urban and rural strata. In the first stage, 1400 Enumeration Areas (EAs) were randomly selected in each sampling stratum with probability proportional to EA size, and a complete household census was conducted to identify the number of households in each selected EA. In the second stage, an equal-probability systematic random sampling technique was applied to select a fixed number of 30 households per EAs. Out of 42,121 eligible women aged 15–49 years, 41,821 responded to the survey, a response rate of 99.3% [13].
The 2018 NDHS recorded information on maternal and child anthropometry, including height and weight measurements for children aged 0–59 months. To improve the quality of anthropometric measurements, the 2018 NDHS implemented data quality assurance procedures, including a subsequent day re-measurement of the height and weight of 10% of a random sample of the children. This study included 12,627 under-5 children in 1377 clusters with valid geographic coordinates and anthropometric data. The detailed methodology for the 2018 NDHS survey has been reported elsewhere [13].
The 2018 NDHS collected geographic coordinates using Global Positioning System (GPS) receivers for each cluster. To keep the confidentiality of respondents in these clusters, GPS coordinates were displaced (geo-masking) by 10 km for rural clusters and 2 km for urban clusters [27]. The NDHS also has information on climatic and demographic factors obtained from publicly available remote sensing raster and vector data sources [27]. During extraction, circular buffers of 2 km for urban points and 10 km for rural points were considered to compensate for displacements in the GPS coordinates of each cluster and differences in the pixel size of data sources [27]. Detailed procedures for extracting DHS geo-covariates were published in the DHS manual [27].
2.2. Outcome Variable
The study’s outcome variable was stunting, which was measured using height-for-age z-scores (HAZ) according to the WHO Child Growth Standards [28]. Height or length was measured using a Shorr measuring Board® (Weigh and Measure, LLC, Olney, MD, USA) [13,29]. Children were considered stunted if their HAZ score was less than −2.0 standard deviations from the median of the WHO reference population for age. The stunting status was dichotomised as “stunted” (1) or “not stunted” (0), in line with the 2018 NDHS report [13] and previously published studies [22,30].
2.3. Explanatory Variables
Using a conceptual framework adapted from the UNICEF [31] and WHO [32] frameworks for undernutrition [32] and used in past studies from LMICs [22,30], we broadly grouped explanatory variables into proximal and contextual factors (Figure 1) [31,32]. For this study, child morbidity (including diarrhoea and acute respiratory infection (ARI)) was included as an immediate proximal factor, given the immediate pathophysiological relationships with stunting, where infection can lead to poor nutrient intake, absorption, or utilisation (Table 1) [31,32].
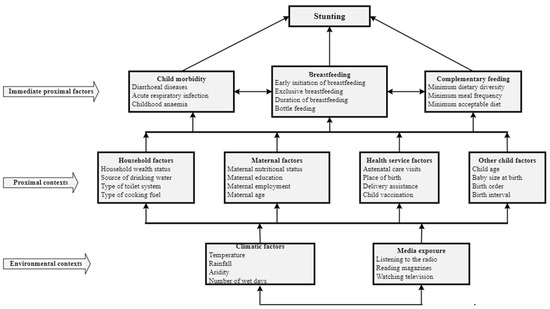
Figure 1.
Conceptual framework for proximal and contextual determinants of stunting among children under five years of age (adapted from UNICEF 2013 [26] and WHO 2017 [27]).

Table 1.
Definition of proximal and contextual factors associated with childhood stunting among children under five years.
As shown in Table 1, proximal contextual factors included maternal factors (i.e., maternal education, nutritional status, employment status, and maternal age), household factors (i.e., household wealth, household toilet system, source of drinking water, and type of cooking fuel), health service factors (i.e., frequency of antenatal care (ANC) visits and place of birth), and child factors (i.e., birth size, child age, and birth order of the child). Environmental contextual factors included exposure to media, while climatic factors were daytime land surface temperature (DLST), aridity, rainfall, and urbanization [33,34]. We selected climatic factors based on recent studies which demonstrated increasing evidence of the impact of poverty and crop production on stunting. Climate-related data were obtained from publicly available remote sources [27].
2.4. Analytical Strategy
The overall analytical framework and strategy for the describing the prevalence of childhood stunting at the second administrative level while examining relevant proximal and contextual factors associated with childhood stunting have been described in detail elsewhere [30].
In summary, frequencies and percentages of proximal and contextual factors were calculated to describe the study participants. The prevalence of stunting was calculated to understand the magnitude of childhood stunting in relation to the proximal and contextual factors. To adjust for sampling weights, clustering, and stratification, all descriptive analyses, including frequencies, percentages, and prevalence, were performed using the “svydesign” function from the “survey” package in R (R Core Team, Austria) [35].
We used a five-staged analytical strategy to implement the Bayesian geostatistical modelling, as reported in detail elsewhere [30]. In stage one, data on environmental and climatic factors were linked with household survey data using a ‘cluster id’ as a unique identifier. Both the geo-covariates and the household survey data have their associated cluster-level geocoordinates. In stage two, model selection was conducted using the Watanabe–Akaike information criterion (WAIC) and deviance information criterion (DIC). We excluded maternal employment, maternal age, delivery assistance, birth order, vaccination status, birth interval media exposure (radio, television, and magazine), and climatic factors (proximity to water bodies and enhanced vegetation index) from the final model.
In stage three, by assuming childhood stunting as a continuous process in space (continuity only refers to the space domain, not the measurement scale), we implemented the stochastic partial differential equation approach (SPDE) using the R-INLA package to fit a spatial model and predict childhood stunting at unsampled locations. The spatial autocorrelation was adjusted using the Matérn covariance matrix by assuming a stationary and isotropic structure (where the correlation between two observation points only depends on their distance) [36]. As geostatistical data (point-referenced data) do not have explicit neighbouring between points, an artificial set of vertices called a mesh was created to represent the neighbouring structure (Figure S1). The observed locations (NDHS clusters) and mesh vertices (that were weighted based on their distance from the observed locations) were mapped using a projector matrix ‘A’ [36].
In stage four, the study used Bayesian geostatistical models to analyse the relationship between stunting and proximal and contextual factors. Bayesian inference was chosen for its ability to consider prior information, make predictions for unsampled locations, provide credible intervals (CrIs), and handle complex models such as spatial and spatiotemporal models [36]. In the prediction model of the prevalence of stunting in high-resolution grids [30,37], the model used proximal and contextual factors with available raster surfaces, including maternal education, ANC visits, place of birth, type of toilet system, source of drinking water, aridity, number of wet days, DLST, and altitude. In stage five, model validation was conducted by grouping the total dataset into a “training set” (75% of the sample) and a “test set” (the remaining 25% of clusters) based on previously published studies [30,38,39]. Figure S2 is presented to show the correlation between the observed and predicted values as model validation. ORs with corresponding 95% CrIs were calculated and reported as the measure of association between proximal and contextual factors and stunting.
3. Results
3.1. Prevalence of Childhood Stunting
The overall national prevalence of childhood stunting was 41.5% (95% CrI: 26.4%, 55.7%). The highest prevalence of stunting reported was in Biriniwa in Jigawa State, Northern Nigeria (p = 66.4%; 95% CrI: 26.3%, 91.7%), followed by Yusufari in Yobe State (p = 66.3%; 95% CrI: 24.4%, 92.1%), while the lowest prevalence was observed in Shomolu in Lagos State Southern Nigeria (p = 2.0%; 95% CrI: 0.5%, 7.6%) (Table 1, Figure 2 and Figure 3). First and second administrative level prevalence estimates are presented in Tables S1 and S2.
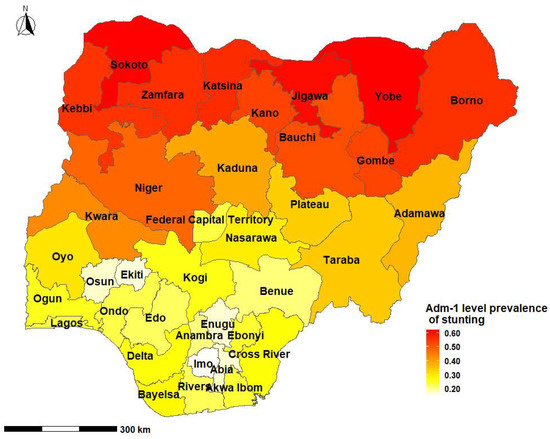
Figure 2.
Prevalence of childhood stunting in Nigeria by states and the Federal Capital Territory, 2018.
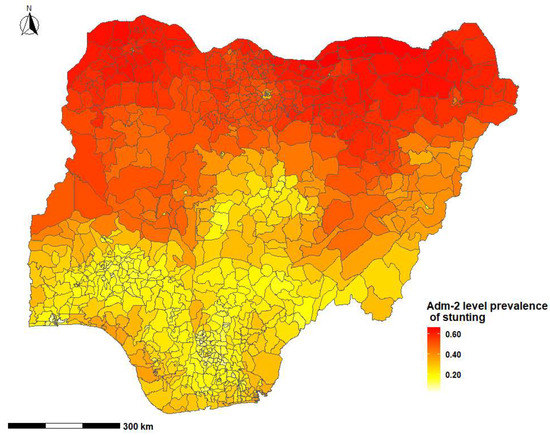
Figure 3.
Prevalence of childhood stunting across the second administrative level in Nigeria by Local Government Councils, 2018.
Children who were perceived by their mothers to be very small at birth had a higher prevalence of stunting, while those who were very large at birth had a lower prevalence of stunting (52.4% vs. 28.2%). Children who experienced three episodes of diarrhoea before the survey had a higher prevalence of stunting compared to those who did not experience episodes of diarrhoea (50.0% vs. 34.6%) (Table 2).
Table 2.
Prevalence of stunting over proximal and contextual determinants among children under five years of age in Nigeria, 2018 NDHS (n = 12,627).
3.2. Determinants of Childhood Stunting
The magnitude of associations between proximal and contextual factors and stunting was similar for both spatial and non-spatial models. Children who were perceived to be small at the time of birth were more likely to be stunted compared to those who were perceived to be very large at birth (aOR = 1.64; 95% CrI: 1.35, 1.99 for small size and aOR = 2.39; 95% CrI: 1.80, 3.17 for very small size). Children who experienced three episodes of diarrhoea in the two weeks before the survey were more likely to be stunted compared to those who did not experience diarrhoea (aOR = 1.35; 95% CrI: 1.18, 1.54) (Table 3).
Table 3.
Proximal and contextual determinants of childhood stunting among children under five years in Nigeria, 2018 NDHS (n = 12,627).
Children whose mothers were overweight or obese were less likely to be stunted compared to mothers with normal weight (aOR = 0.79; 95% CrI: 0.69, 0.89 for overweight and aOR = 0.63; 95% CrI: 0.52, 0.76 for obese). Children whose mothers attained secondary or higher schooling were less likely to be stunted compared to those whose mothers did not attain any schooling (aOR = 0.69; 95% CrI: 0.60, 0.80), while children who resided in rich households were less likely to be stunted compared to those who resided in poor households (aOR = 0.75; 95% CrI: 0.64, 0.8) (Table 3).
Children who resided in households with a clean type of cooking fuel were less likely to be stunted compared to those resided in household with no clean type of cooking fuel (aOR = 0.79; 95% CrI: 0.67, 0.92). Residing in a medium rainfall geographic area (142–1199 mm rainfall) was negatively associated with childhood stunting compared to a low rainfall geographic area (aOR = 0.78; 95% CrI: 0.64, 0.96), while children who resided in urban centres (cities) were less likely to be stunted compared to those who resided in rural villages (aOR = 0.69; 95% CrI: 0.59, 0.82). Children from the North-eastern Nigeria region were more likely to be stunted compared to those who resided in the North-central region (aOR = 1.81; 95% CrI: 1.26, 2.57) (Table 3).
4. Discussion
This study showed striking sub-national and regional variations in the prevalence of stunting in Nigeria. Biriniwa in Jigawa State in Northern Nigeria had the highest prevalence of stunting, while Shomolu in Lagos State in Southern Nigeria had the lowest prevalence of stunting. Factors that were positively associated with stunting included perceived birth size (small at birth) and three episodes of diarrhoea in the two weeks before the survey. Children whose mothers received formal education and/or were overweight or obese were less likely to be stunted compared to compared to those who were not.
The availability of appropriate regional estimates of malnutrition is essential in order to provide the appropriate health services to the relevant population [25]. Consistent with past studies conducted in Ethiopia [30] and Rwanda [40], the current study showed wide geospatial variations of childhood stunting in Nigeria. Our findings demonstrated a high prevalence of childhood stunting in Northern Nigeria. This high burden of stunting is multifactorial, and could be attributed to the complex interplay of low education and literacy rate, poverty, inadequate health service utilisations, food insecurity, and activities of the Boko Haram (terrorist) Organisation in Northern Nigeria [13]. National nutrition programmes in Nigeria must not only be holistic but should also consider the specific geopolitical locations with the highest burden of malnutrition.
Diarrhoeal disease is the second leading cause of deaths of children aged under 5 globally (attributable to 525,000 deaths yearly), and most of these deaths are related to frequent episodes of diarrhoea each year [41]. Our study showed that children who reported three diarrhoeal episodes in the two weeks before the survey were more likely to be stunted compared to their counterparts. This finding is similar to a prior Nigerian study, which showed a positive association between diarrhoeal episodes and stunting [22]. Diarrhoeal disease leads to childhood malnutrition in the following pathways: (i) through reduced appetite and increased catabolism; (ii) impaired intestinal absorption due to the altered barrier and mucosal inflammation [42]; and (iii) displacements of essential nutrients (e.g., minerals and vitamins) for the immune response [22,42]. Our findings suggest the need to promote national policies and investments that support case management of common childhood illnesses (including diarrhoea) and their complications, as well as to increase access to safe drinking water and sanitation in Nigeria.
Maternal nutritional intake during pregnancy negatively affects the division and replication of cells in the embryo and the development of the foetus in later stages of pregnancy, with subsequent impacts on the birth size, nutritional status, and development of the baby [43]. Consistent with this evidence and previously published studies conducted in Ethiopia [30] and Tanzania [44], children whose mothers perceived them as small or very small in size at the time of delivery were more likely to be stunted compared to their counterparts. Poor fat and protein absorption, difficulties in initiating breastfeeding, infections, and hospitalisations [45] are associated with small-birth-size children. This association possibly explains the relationship between small-birth-size children and stunting. Our findings suggest the need for interventions to improve the nutritional status of women before and during pregnancy to eliminate the intergenerational influence of malnutrition.
Past studies have showed the protective effect of living in improved socioeconomic neighbourhoods on the nutritional status of children [1,46]. Studies from Ethiopia [30] and Tanzania [44] showed that higher socioeconomic households were associated with a lower risk of childhood stunting. There are several reasons for the protective effect of improved socioeconomic status on childhood malnutrition, including: (i) it increases the household decision-making power of women (including a decision on food purchases) [47]; (ii) it has positive impacts on household income and food purchasing power [48]; and (iii) it improves the healthcare-seeking behaviours of parents for timely vaccination and treatment of the sick child [49]. Improvement of programmes that target disadvantaged socioeconomic neighbours in Northern Nigeria and urban slums in Southern Nigeria would help to improve the nutritional status of Nigerian children.
This study showed that children who resided in geographic locations with medium rainfall were less likely to be stunted, consistent with findings from Ethiopia [50]. Extreme rainfall and climatic variability have negative implications on crop production, household food security, and malnutrition. This is particularly common in sub-Saharan African countries (including Nigeria), where crop production is predominantly based on rain-fed agriculture [51,52]. The effect of climate variability on food production is not only prominent in sub-Saharan African countries, but the utilisation of adaptation and resilient mechanisms (such as agricultural irrigation) is inadequate [51,52]. Our findings suggest the need for adaptation measures that sustainably increase water availability (e.g., irrigation) for crop production and diversification of agriculture production (e.g., crops, livestock, and fisheries) to subsequently improve the nutritional status of Nigerian children.
Research on urban–rural disparities of malnutrition showed that urban children (apart from those living in urban slums) generally have improved nutritional status compared to rural children [53,54]. These studies also showed that urban children have better access to food, good housing, employment opportunities for parents, access to health services, and basic amenities (e.g., electricity, water, and sanitation) [53]. Findings from the current study showed that children who resided in urban cities (apart from those residing in the slums) were less likely to be stunted compared to their counterparts. The finding is similar to evidence from a Tanzanian study [44]. However, a study conducted in Zambia [55] showed a positive association between urban children and stunting. Although the present study showed that urban children had a lower risk of stunting, there is also a need for further research on urban–rural disparities and its determinants to examine the proximal and contextual factors separately.
Strengths and Limitations of the Study
The study has the following limitations. First, the inference of causality between the measured exposure variables and the outcome (stunting) is challenging given the use of a cross-sectional dataset. Nevertheless, the study findings are consistent with results from other studies that used cross-sectional data or more robust study designs. Additionally, the analyses of some study factors (e.g., climatic factors) can only be performed with data obtained from observational study designs. Second, unobserved potential confounders, including food insecurity and social networks, may affect the results of our findings. Nevertheless, climatic factors (e.g., aridity, rainfall, and temperature) can be proxy indicators for agricultural production and food security [33]. Finally, non-differential misclassification bias due to the displacement of GPS coordinates is possible. However, we used a circular buffer while extracting geo-covariates from each cluster [27]. Despite these limitations, the study has strengths. The national representativeness of the DHS data increases the generalisability of the findings. The study used Bayesian inference to utilise its superior strength in spatial modelling and the production of small-surface-area estimates. Additionally, we investigated the association between environmental and climatic factors with stunting, and these results provided detailed understanding of the public health issues relating to childhood malnutrition in Nigeria.
5. Conclusions
The study showed wide variations in stunting prevalence across the second-level administrative regions in Nigeria, where Biriniwa in Jigawa State in Northern Nigeria had the highest prevalence of stunting, and Shomolu in Lagos State in Southern Nigeria reported the lowest prevalence. Children who were perceived to be small, those who experienced diarrhoea, and those living in disadvantaged areas in the north or urban slums in the south were more at risk of being stunted. The results highlight the importance of investing and implementing targeted health and socioeconomic policies to reduce childhood illnesses (such as diarrhoea) and access to safe water and sanitation in Nigeria. Targeting disadvantaged neighborhoods in Northern Nigeria and urban slums in Southern Nigeria through programmes can improve child nutrition. Further research is also needed to investigate the urban–rural disparities in stunting and its determinants by urban–rural status specifically.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph20043250/s1, Figure S1: An artificially created mesh to represent the neighboring structure of the study region; Figure S2: Correlation between observed and fitted values for stunting; Table S1: Prevalence of childhood stunting across the first administrative level of Nigeria, 2022; Table S2: Prevalence of childhood stunting across the second administrative level of Nigeria (local government councils), 2022.
Author Contributions
Conceptualization and data curation: K.Y.A.; methodology: K.Y.A., F.A.O., A.G.R., S.M.H., K.E.A. and B.O.O.; validation: K.Y.A., F.A.O., A.G.R., S.M.H., K.E.A. and B.O.O.; software and formal analysis, K.Y.A.; writing—original draft preparation, K.Y.A.; writing—review and editing F.A.O., A.G.R., S.M.H., K.E.A. and B.O.O.; visualization, K.Y.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, because this study was based on secondary data analysis.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Datasets are available at https://www.dhsprogram.com/data/ (accessed on 15 November 2021).
Acknowledgments
The authors are grateful to Measure DHS/ICF International for providing the data for analysis.
Conflicts of Interest
The authors declare that they have no competing interest. F.A.O. is an Advisory board and Editorial member for the International Journal of Environmental Research and Public Health (IJERPH) and does not have any role in the journal review and decision-making process for this manuscript.
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef] [PubMed]
- Kirolos, A.; Blacow, R.M.; Parajuli, A.; Welton, N.J.; Khanna, A.; Allen, S.J.; McAllister, D.A.; Campbell, H.; Nair, H. The impact of childhood malnutrition on mortality from pneumonia: A systematic review and network meta-analysis. BMJ Glob. Health 2021, 6, e007411. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2019, 395, 75–88. [Google Scholar] [CrossRef]
- Siddiqui, F.; Salam, R.A.; Lassi, Z.S.; Das, J.K. The Intertwined Relationship Between Malnutrition and Poverty. Front. Public Health 2020, 8, 453. [Google Scholar] [CrossRef] [PubMed]
- SDG-UN. Transforming Our World: The 2030 Agenda for Sustainable Development; UN: New York, NY, USA, 2015.
- World Health Assembly. United Nations Decade of Action on Nutrition (2016–2025); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- WHO. Global Targets 2025: To Improve Maternal, Infant and Young Child Nutrition. Available online: https://www.who.int/nutrition/global-target-2025/en/ (accessed on 13 July 2020).
- Development Initiatives. 2020 Global Nutrition Report: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020. [Google Scholar]
- WHO. Global Targets 2025 Tracking Tool to Improve Maternal, Infant and Young Child Nutrition; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- The World Bank. Population, Total—Nigeria. 2022. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=NG (accessed on 29 August 2022).
- Macrotrends. Nigeria Economic Growth 1960–2022. 2022. Available online: https://www.macrotrends.net/countries/NGA/nigeria/economic-growth-rate (accessed on 24 August 2022).
- National Population Commission (NPC) [Nigeria]; ICF. Nigeria Demographic and Health Survey 2018; NPC: Abuja, Nigeria; ICF: Rockville, MD, USA, 2019.
- United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME). Levels and Trends in Child Mortality: Report 2020, Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; United Nations Children’s Fund: New York, NY, USA, 2020.
- United Nations. The Millennium Development Goals Report 2015; United Nations: New York, NY, USA, 2015.
- Ministry of Budget and National Planning. National Policy on Food and Nutrition in Nigeria; Ministry of Budget and National Planning: Abuja, Nigeria, 2016.
- Oxford Policy Management. Child Development Cash Transfer Helps Reduce Stunting Rates in Northern Nigeria. 2019. Available online: https://www.opml.co.uk/blog/child-development-cash-transfer-helps-reduce-stunting-rates-in-northern-nigeria (accessed on 29 August 2022).
- UNICEF; WHO; World Bank Group. Levels and Trends in Child Malnutrition; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Agu, N.; Emechebe, N.; Yusuf, K.; Falope, O.; Kirby, R.S. Predictors of early childhood undernutrition in Nigeria: The role of maternal autonomy. Public Health Nutr. 2019, 22, 2279–2289. [Google Scholar] [CrossRef]
- Ezeh, O.K.; Abir, T.; Zainol, N.R.; Al Mamun, A.; Milton, A.H.; Haque, R.; Agho, K.E. Trends of Stunting Prevalence and Its Associated Factors among Nigerian Children Aged 0–59 Months Residing in the Northern Nigeria, 2008–2018. Nutrients 2021, 13, 4312. [Google Scholar] [CrossRef]
- Adeyemi, O.; Toure, M.; Covic, N.; Bold, M.V.D.; Nisbett, N.; Headey, D. Understanding drivers of stunting reduction in Nigeria from 2003 to 2018: A regression analysis. Food Secur. 2022, 14, 995–1011. [Google Scholar] [CrossRef]
- Akombi, B.J.; Agho, K.E.; Hall, J.J.; Merom, D.; Astell-Burt, T.; Renzaho, A.M.N. Stunting and severe stunting among children under-5 years in Nigeria: A multilevel analysis. BMC Pediatr. 2017, 17, 15. [Google Scholar] [CrossRef]
- Local Burden of Disease Child Growth Failure Collaborators. Mapping child growth failure across low- and middle-income countries. Nature 2020, 577, 231–234. [Google Scholar] [CrossRef]
- Horton, R. Offline: In defence of precision public health. Lancet 2018, 392, 1504. [Google Scholar] [CrossRef]
- Arnold, C. Is precision public health the future—Or a contradiction? Nature 2022, 601, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Health Nigeria. National Health Promotion Policy; Federal Ministry of Health, Nigeria: Abuja, Nigeria, 2019.
- Mayala, B.; Fish, T.D.; Eitelberg, D.; Dontamsetti, T. The DHS Program Geospatial Covariate Datasets Manual, 2nd ed.; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization; United Nations Children’s Fund (WHO/UNICEF). Recommendations for Data Collection, Analysis and Reporting on Anthropometric Indicators in Children under 5 Years Old; WHO/UNICEF: Geneva, Switzerland, 2019. [Google Scholar]
- Ahmed, K.; Agho, K.; Page, A.; Arora, A.; Ogbo, F.; on behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). Mapping Geographical Differences and Examining the Determinants of Childhood Stunting in Ethiopia: A Bayesian Geostatistical Analysis. Nutrients 2021, 13, 2104. [Google Scholar] [CrossRef]
- UNICEF. Improving Child Nutrition: The Achievable Imperative for Global Progress; UNICEF: New York, NY, USA, 2013. [Google Scholar]
- WHO. Childhood Stunting: Contexts, Causes and Consequences; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Kinyoki, D.K.; Berkley, J.A.; Moloney, G.M.; Odundo, E.O.; Kandala, N.-B.; Noor, A.M. Environmental predictors of stunting among children under-five in Somalia: Cross-sectional studies from 2007 to 2010. BMC Public Health 2016, 16, 654. [Google Scholar] [CrossRef]
- Gething, P.W.; Tatem, A.J.; Bird, T.; Burgert, C. Creating Spatial Interpolation: Surfaces with DHS Data DHS Spatial Analysis Reports No. 11; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Team, R.C. R Core TeamR: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Moraga, P. Geospatial Health Data: Modeling and Visualization with R-INLA and Shiny; Chapman & Hall/CRC Biostatistics Series; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Burgert-Brucker, C.R.; Domtamsetti, T.; Marshall, A.M.; Gething, P. Guidance for Use of The DHS Program Modeled Map Surfaces; DHS Spatial Analysis Reports No. 14; ICF International: Rockville, MD, USA, 2016. [Google Scholar]
- Kang, S.Y.; Battle, K.E.; Gibson, H.S.; Ratsimbasoa, A.; Randrianarivelojosia, M.; Ramboarina, S.; Zimmerman, P.A.; Weiss, D.J.; Cameron, E.; Gething, P.W.; et al. Spatio-temporal mapping of Madagascar’s Malaria Indicator Survey results to assess Plasmodium falciparum endemicity trends between 2011 and 2016. BMC Med. 2018, 16, 71. [Google Scholar] [CrossRef] [PubMed]
- Adigun, A.B.; Gajere, E.N.; Oresanya, O.; Vounatsou, P. Malaria risk in Nigeria: Bayesian geostatistical modelling of 2010 malaria indicator survey data. Malar. J. 2015, 14, 156. [Google Scholar] [CrossRef]
- Uwiringiyimana, V.; Osei, F.; Amer, S.; Veldkamp, A. Bayesian geostatistical modelling of stunting in Rwanda: Risk factors and spatially explicit residual stunting burden. BMC Public Health 2022, 22, 159. [Google Scholar] [CrossRef] [PubMed]
- WHO. Diarrhoeal Disease. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease (accessed on 6 September 2022).
- Humphrey, J.H. Child undernutrition, tropical enteropathy, toilets, and handwashing. Lancet 2009, 374, 1032–1035. [Google Scholar] [CrossRef]
- Cortés-Albornoz, M.C.; García-Guáqueta, D.P.; Velez-Van-Meerbeke, A.; Talero-Gutiérrez, C. Maternal Nutrition and Neurodevelopment: A Scoping Review. Nutrients 2021, 13, 3530. [Google Scholar] [CrossRef]
- Chirande, L.; Charwe, D.; Mbwana, H.; Victor, R.; Kimboka, S.; Issaka, A.I.; Baines, S.K.; Dibley, M.J.; Agho, K.E. Determinants of stunting and severe stunting among under-fives in Tanzania: Evidence from the 2010 cross-sectional household survey. BMC Pediatr. 2015, 15, 165. [Google Scholar] [CrossRef]
- Hviid, A.; Melbye, M. The Impact of Birth Weight on Infectious Disease Hospitalization in Childhood. Am. J. Epidemiol. 2006, 165, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Lamb, K.E.; Costa, C.; Cutumisu, N.; Ellaway, A.; Kamphuis, C.B.M.; Mentz, G.; Pearce, J.; Santana, P.; Santos, R.; et al. Neighbourhood socioeconomic disadvantage and fruit and vegetable consumption: A seven countries comparison. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Makoka, D.; Masibo, P.K. Is there a threshold level of maternal education sufficient to reduce child undernutrition? Evidence from Malawi, Tanzania and Zimbabwe. BMC Pediatr. 2015, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E.; Lancet Nutrition Interventions Review Group and Maternal and Child Nutrition Study Group. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Abuya, B.A.; Onsomu, E.O.; Kimani, J.K.; Moore, D. Influence of Maternal Education on Child Immunization and Stunting in Kenya. Matern. Child Health J. 2010, 15, 1389–1399. [Google Scholar] [CrossRef]
- Hagos, S.; Lunde, T.; Mariam, D.H.; Woldehanna, T.; Lindtjørn, B. Climate change, crop production and child under nutrition in Ethiopia; a longitudinal panel study. BMC Public Health 2014, 14, 884. [Google Scholar] [CrossRef]
- Olayide, O.E.; Tetteh, I.K.; Popoola, L. Differential impacts of rainfall and irrigation on agricultural production in Nigeria: Any lessons for climate-smart agriculture? Agric. Water Manag. 2016, 178, 30–36. [Google Scholar] [CrossRef]
- Hasegawa, T.; Sakurai, G.; Fujimori, S.; Takahashi, K.; Hijioka, Y.; Masui, T. Extreme climate events increase risk of global food insecurity and adaptation needs. Nat. Food 2021, 2, 587–595. [Google Scholar] [CrossRef]
- Mussa, R. A matching decomposition of the rural–urban difference in malnutrition in Malawi. Health Econ. Rev. 2014, 4, 11. [Google Scholar] [CrossRef]
- Fotso, J.-C. Urban–rural differentials in child malnutrition: Trends and socioeconomic correlates in sub-Saharan Africa. Health Place 2007, 13, 205–223. [Google Scholar] [CrossRef]
- Mzumara, B.; Bwembya, P.; Halwiindi, H.; Mugode, R.; Banda, J. Factors associated with stunting among children below five years of age in Zambia: Evidence from the 2014 Zambia demographic and health survey. BMC Nutr. 2018, 4, 51. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).