
Changes in Physical Fitness Parameters in a Portuguese Sample of Adolescents during the COVID-19 Pandemic: A One-Year Longitudinal Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
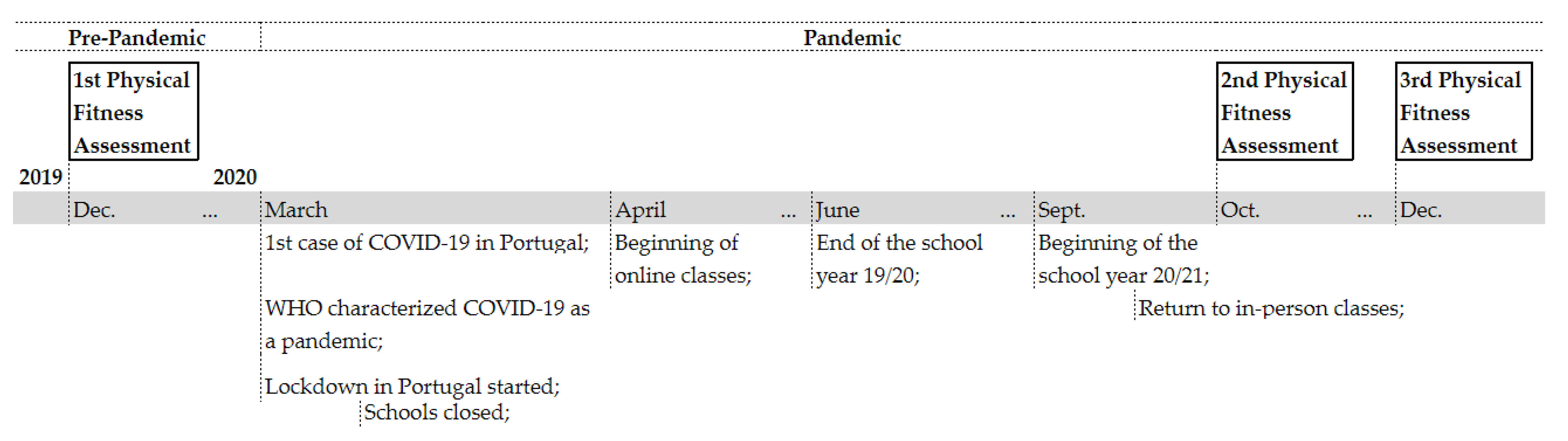
2.1. Sample and Setting
2.2. Material and Measurements
2.2.1. Sociodemographic Information
2.2.2. Physical Fitness
Anthropometric Measures and Body Composition
Aerobic Fitness
Neuromuscular Fitness
2.3. Statistical Analysis
3. Results
3.1. Overall Changes in Physical Fitness over Time
3.1.1. T1 vs. T2
3.1.2. T2 vs. T3
3.1.3. T1 vs. T3
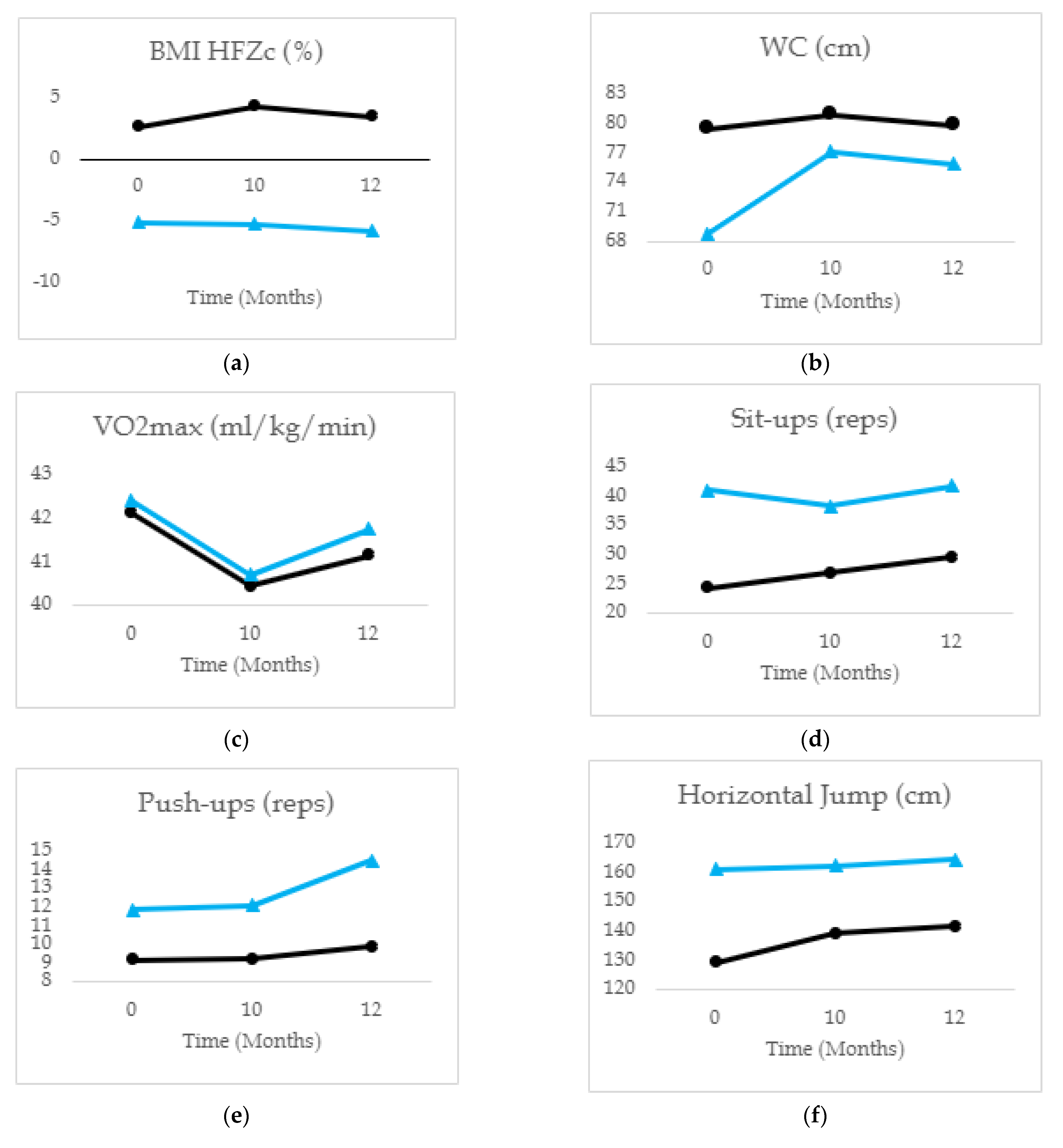
3.2. Physical Fitness Changes over Time in Early and Middle Adolescents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masanovic, B.; Gardasevic, J.; Marques, A.; Peralta, M.; Demetriou, Y.; Sturm, D.J.; Popovic, S. Trends in Physical Fitness Among School-Aged Children and Adolescents: A Systematic Review. Front. Pediatr. 2020, 8, 627529. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chi, G.; Wang, L.; Chen, S.; Yan, J.; Li, S. The Combinations of Physical Activity, Screen Time, and Sleep, and Their Associations with Self-Reported Physical Fitness in Children and Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 5783. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. (Ed.). Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151418-7.
- Silva, C.; Rosendo, D.; Magalhães, P.; Pereira, B.; Gonçalves, S.; Rice, E.; Rosário, P. Eating Behaviors in Children and Adolescents during the COVID-19 Pandemic: The Importance of Family Context. In A Closer Look at Children’s Health; Nova Science Publishers, Inc.: New York, NY, USA, 2022; pp. 47–89. [Google Scholar]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the Effects of Home Confinement on Children during the COVID-19 Outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Zhou, J.; Xie, X.; Guo, B.; Pei, R.; Pei, X.; Yang, S.; Jia, P. Impact of COVID-19 Lockdown on Physical Activity Among the Chinese Youths: The COVID-19 Impact on Lifestyle Change Survey (COINLICS). Front. Public Health 2021, 9, 592795. [Google Scholar] [CrossRef]
- Yang, S.; Guo, B.; Ao, L.; Yang, C.; Zhang, L.; Zhou, J.; Jia, P. Obesity and Activity Patterns before and during COVID-19 Lockdown among Youths in China. Clin. Obes. 2020, 10, e12416. [Google Scholar] [CrossRef]
- Tulchin-Francis, K.; Stevens, W.; Gu, X.; Zhang, T.; Roberts, H.; Keller, J.; Dempsey, D.; Borchard, J.; Jeans, K.; VanPelt, J. The Impact of the Coronavirus Disease 2019 Pandemic on Physical Activity in U.S. Children. J. Sport Health Sci. 2021, 10, 323–332. [Google Scholar] [CrossRef]
- Basterfield, L.; Burn, N.L.; Galna, B.; Batten, H.; Goffe, L.; Karoblyte, G.; Lawn, M.; Weston, K.L. Changes in Children’s Physical Fitness, BMI and Health-Related Quality of Life after the First 2020 COVID-19 Lockdown in England: A Longitudinal Study. J. Sport. Sci. 2022, 40, 1088–1096. [Google Scholar] [CrossRef]
- Rúa-Alonso, M.; Rial-Vázquez, J.; Nine, I.; Lete-Lasa, J.R.; Clavel, I.; Giráldez-García, M.A.; Rodríguez-Corral, M.; Dopico-Calvo, X.; Iglesias-Soler, E. Comparison of Physical Fitness Profiles Obtained before and during COVID-19 Pandemic in Two Independent Large Samples of Children and Adolescents: DAFIS Project. Int. J. Environ. Res. Public Health 2022, 19, 3963. [Google Scholar] [CrossRef]
- Tsoukos, A.; Bogdanis, G.C. The Effects of a Five-Month Lockdown Due to COVID-19 on Physical Fitness Parameters in Adolescent Students: A Comparison between Cohorts. Int. J. Environ. Res. Public Health 2022, 19, 326. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Casaña, J.; Ezzatvar, Y.; Casajús, J.A.; López-Sánchez, G.F.; Smith, L. Cardiorespiratory Fitness in Adolescents before and after the COVID-19 Confinement: A Prospective Cohort Study. Eur. J. Pediatr. 2021, 180, 2287–2293. [Google Scholar] [CrossRef] [PubMed]
- Wahl-Alexander, Z.; Camic, C.L. Impact of COVID-19 on School-Aged Male and Female Health-Related Fitness Markers. Pediatr. Exerc. Sci. 2021, 33, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Jarnig, G.; Kerbl, R.; van Poppel, M.N.M. Change in BMI and Fitness among Primary School Children in Austria: A 24-Month Follow-Up Study of 303 Children Measured before and during the Ongoing COVID-19 Pandemic. Sports 2022, 10, 78. [Google Scholar] [CrossRef]
- Allen, B.; Waterman, H. Stages of Adolescence. Available online: https://www.healthychildren.org/English/ages-stages/teen/Pages/Stages-of-Adolescence.aspx (accessed on 1 December 2022).
- Saint-Maurice, P.F.; Welk, G.J.; Bai, Y. The Healthy Fitness Zone Continuum Score as a Measure of Change in Body Mass Index of School-Aged Children and Adolescents, Georgia, 2012–2014. Public Health Rep. 2017, 132, 57S–64S. [Google Scholar] [CrossRef] [Green Version]
- Welk, G.J.; Laurson, K.R.; Eisenmann, J.C.; Cureton, K.J. Development of Youth Aerobic-Capacity Standards Using Receiver Operating Characteristic Curves. Am. J. Prev. Med. 2011, 41, S111–S116. [Google Scholar] [CrossRef] [PubMed]
- Plowman, S.A.; Meredith, M.D. (Eds.) Fitnessgram/Activitygram Reference Guide, 4th ed.; The Cooper Institute: Dallas, TX, USA, 2013. [Google Scholar]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The Multistage 20 Metre Shuttle Run Test for Aerobic Fitness. J. Sport. Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Fife-Schaw, C. Levels of Measurement. In Research Methods in Psychology; Breakwell, G.M., Hammond, S., Fife-Schaw, C., Smith, J.A., Eds.; Sage Publications, Inc.: New York, NY, USA, 2006; pp. 50–63. [Google Scholar]
- Cunha, J.; Silva, C.; Guimarães, A.; Sousa, P.; Vieira, C.; Lopes, D.; Rosário, P. No Children Should Be Left Behind During COVID-19 Pandemic: Description, Potential Reach, and Participants’ Perspectives of a Project Through Radio and Letters to Promote Self-Regulatory Competences in Elementary School. Front. Psychol. 2021, 12, 647708. [Google Scholar] [CrossRef]
- Jansen, E.; Thapaliya, G.; Aghababian, A.; Sadler, J.; Smith, K.; Carnell, S. Parental Stress, Food Parenting Practices and Child Snack Intake during the COVID-19 Pandemic. Appetite 2021, 161, 105–119. [Google Scholar] [CrossRef]
- Margaritis, I.; Houdart, S.; El Ouadrhiri, Y.; Bigard, X.; Vuillemin, A.; Duché, P. How to Deal with COVID-19 Epidemic-Related Lockdown Physical Inactivity and Sedentary Increase in Youth? Adaptation of Anses’ Benchmarks. Arch. Public Health 2020, 78, 52. [Google Scholar] [CrossRef]
- Rossi, L.; Behme, N.; Breuer, C. Physical Activity of Children and Adolescents during the COVID-19 Pandemic—A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in Children Living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Barone Gibbs, B.; Kline, C.E.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Marta, C.C.; Marinho, D.A.; Barbosa, T.M.; Izquierdo, M.; Marques, M.C. Physical Fitness Differences Between Prepubescent Boys and Girls. J. Strength Cond. Res. 2012, 26, 1756–1766. [Google Scholar] [CrossRef] [PubMed]
- Trandafir, L.M.; Russu, G.; Moscalu, M.; Miron, I.; Lupu, V.V.; Leon Constantin, M.M.; Cojocaru, E.; Lupu, A.; Frasinariu, O.E. Waist Circumference a Clinical Criterion for Prediction of Cardio-Vascular Complications in Children and Adolescences with Overweight and Obesity. Medicine 2020, 99, e20923. [Google Scholar] [CrossRef] [PubMed]
- Manna, I. Growth Development and Maturity in Children and Adolescent: Relation to Sports and Physical Activity. Am. J. Sport. Sci. Med. 2014, 2, 48–50. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 28 November 2022).


{kind=link}
{kind=link}
{kind=link}
| Participants | T1 | T2 | T3 | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Sex | ||||
| Girls | 305 (47.7) | 273 (47.5) | 280 (47.5) | |
| Boys | 335 (52.3) | 302 (52.5) | 310 (52.5) | |
| Subgroup | ||||
| Early Adolescents | 497 (77.7) | 360 (62.6) | 338 (57.3) | |
| Middle Adolescents | 143 (22.3) | 215 (37.4) | 252 (42.7) | |
| Pre-Pandemic | Pandemic | Bonferroni Pairwise Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 (December 2019) M (SD) | T2 (October 2020)M (SD) | T3 (December 2020) M (SD) | |||||||
| ηp2 | T1 vs. T2 | T2 vs. T3 | T1 vs. T3 | ||||||
| Body Composition | |||||||||
| BMI HFZc (%) (n = 519) | 1.14 (21.59) | 2.45 (21.90) | 1.68 (21.31) | F (1.376, 712.705) 3.864 * | 0.007 | * | * | ns | |
| WC (cm) (n = 148) | 75.39 (16.79) | 79.53 (11.97) | 78.36 (11.55) | F (1.267, 186.209) 13.301 *** | 0.083 | *** | * | ** | |
| Aerobic Fitness | |||||||||
| VO2max (ml/kg/min) (n = 506) | 42.15 (5.45) | 40.48 (5.19) | 41.24 (5.53) | F (1.675, 845.629) 73.620 *** | 0.127 | *** | *** | *** | |
| Neuromuscular Fitness | |||||||||
| Sit-ups (n = 411) | 27.55 (19.22) | 29.04 (19.97) | 31.85 (20.95) | F (1.784, 731.531) 15.087 *** | 0.035 | ns | *** | *** | |
| Push-ups (n = 427) | 9.65 (7.70) | 9.75 (7.17) | 10.74 (7.77) | F (1.643, 699.882) 8.447 *** | 0.019 | ns | *** | ** | |
| Horizontal Jump (n = 418) | 135.64 (31.32) | 143.73 (32.92) | 146.18 (33.84) | F (1.848, 770.637) 76.767 *** | 0.155 | *** | ** | *** | |
| 20 m Run (n = 468) | 4.34 (0.62) | 4.31 (0.57) | 4.30 (0.58) | F (1.516, 707.765) 1.722 (ns) | 0.004 | ns | ns | ns | |
| Sit and Reach (n = 439) | 18.23 (7.61) | 20.24 (8.05) | 20.64 (8.00) | F (1.634, 715.831) 896.436 *** | 0.104 | *** | ns | *** | |
| Pre-Pandemic | Pandemic | Bonferroni Pairwise Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 (Dec 2019) M (SD) | T2 (Oct 2020) M (SD) | T3 (Dec 2020) M (SD) | |||||||
| ηp2 | T1 vs. T2 | T2 vs. T3 | T1 vs. T3 | ||||||
| Body Composition | |||||||||
| BMI HFZc (%) (n = 519) | Early Adolescents (n = 421) | 2.61 (21.63) | 4.26 (21.53) | 3.43 (20.43) | F (1.377, 711.718) = 1.280 (ns) | 0.002 | * | * | ns |
| Middle Adolescents (n = 98) | −5.16 (20.35) | −5.32 (21.88) | −5.84 (22.11) | ns | ns | ns | |||
| WC (cm) (n = 148) | Early Adolescents (n = 90) | 79.56 (11.33) | 81.01 (10.35) | 79.90 (10.13) | F (1.289, 188.125) = 11.507 *** | 0.073 | ns | ns | ns |
| Middle Adolescents (n = 58) | 68.92 (21.37) | 77.24 (13.92) | 75.98 (13.20) | *** | ns | *** | |||
| Aerobic Fitness | |||||||||
| VO2max (ml/kg/min) (n = 506) | Early Adolescents (n = 416) | 42.10 (5.00) | 40.43 (4.52) | 41.14 (4.91) | F (1.673, 843.387) = 0.518 (ns) | 0.001 | *** | *** | *** |
| Middle Adolescents (n = 90) | 42.39 (7.18) | 40.69 (7.57) | 41.73 (7.81) | *** | *** | ns | |||
| Neuromuscular Fitness | |||||||||
| Sit-ups (n = 411) | Early Adolescents (n = 330) | 24.25 (16.95) | 26.81 (18.32) | 29.46 (19.81) | F (1.791, 732.593) = 4.207 * | 0.010 | * | *** | *** |
| Middle Adolescents (n = 81) | 40.96 (22.00) | 38.16 (23.63) | 41.60 (22.72) | ns | ns | ns | |||
| Push-ups (n = 427) | Early Adolescents (n = 344) | 9.13 (7.42) | 9.20 (6.52) | 9.84 (7.00) | F (1.633, 694.171) = 4.335 * | 0.010 | ns | * | ns |
| Middle Adolescents (n = 83) | 11.82 (8.45) | 12.06 (9.06) | 14.48 (9.53) | ns | *** | *** | |||
| Horizontal Jump (n = 418) | Early Adolescents (n = 330) | 128.95 (25.77) | 138.84 (29.47) | 141.35 (30.17) | F (1.866, 776.174) = 10.822 *** | 0.025 | *** | ** | *** |
| Middle Adolescents (n = 88) | 160.73 (37.20) | 162.08 (38.45) | 164.28 (40.35) | ns | ns | ns | |||
| 20 m Run (n = 468) | Early Adolescents (n = 375) | 4.42 (0.59) | 4.40 (0.55) | 4.39 (0.56) | F (1.516, 706.474) = 0.447 (ns) | 0.001 | ns | ns | ns |
| Middle Adolescents (n = 93) | 4.01 (0.62) | 3.95 (0.51) | 3.93 (0.49) | ns | ns | ns | |||
| Sit and Reach (n = 439) | Early Adolescents (n = 350) | 17.25 (7.23) | 20.32 (7.97) | 20.12 (7.94) | F (1.646, 719.336) = 36.725 *** | 0.078 | *** | ns | *** |
| Middle Adolescents (n = 89) | 22.05 (7.90) | 19.90 (8.39) | 22.66 (7.96) | *** | *** | ns | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, C.; Vilas, C.; Pereira, B.; Rosário, P.; Fuentes, S.; Magalhães, P. Changes in Physical Fitness Parameters in a Portuguese Sample of Adolescents during the COVID-19 Pandemic: A One-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2023, 20, 3422. https://doi.org/10.3390/ijerph20043422
Silva C, Vilas C, Pereira B, Rosário P, Fuentes S, Magalhães P. Changes in Physical Fitness Parameters in a Portuguese Sample of Adolescents during the COVID-19 Pandemic: A One-Year Longitudinal Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3422. https://doi.org/10.3390/ijerph20043422
Chicago/Turabian StyleSilva, Cátia, Catarina Vilas, Beatriz Pereira, Pedro Rosário, Sonia Fuentes, and Paula Magalhães. 2023. "Changes in Physical Fitness Parameters in a Portuguese Sample of Adolescents during the COVID-19 Pandemic: A One-Year Longitudinal Study" International Journal of Environmental Research and Public Health 20, no. 4: 3422. https://doi.org/10.3390/ijerph20043422