
Evidence of Use of Whole-Body Vibration in Individuals with Metabolic Syndrome: A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
,  , , ,
, , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Level of Evidence of the Selected Publications
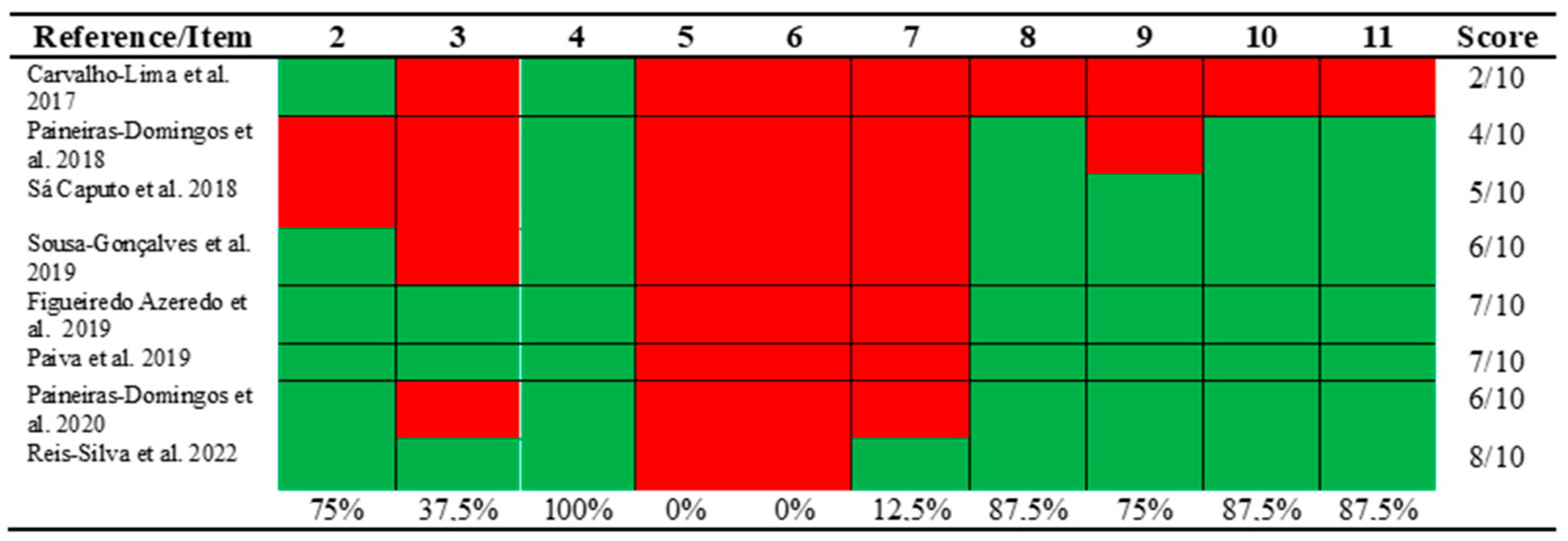
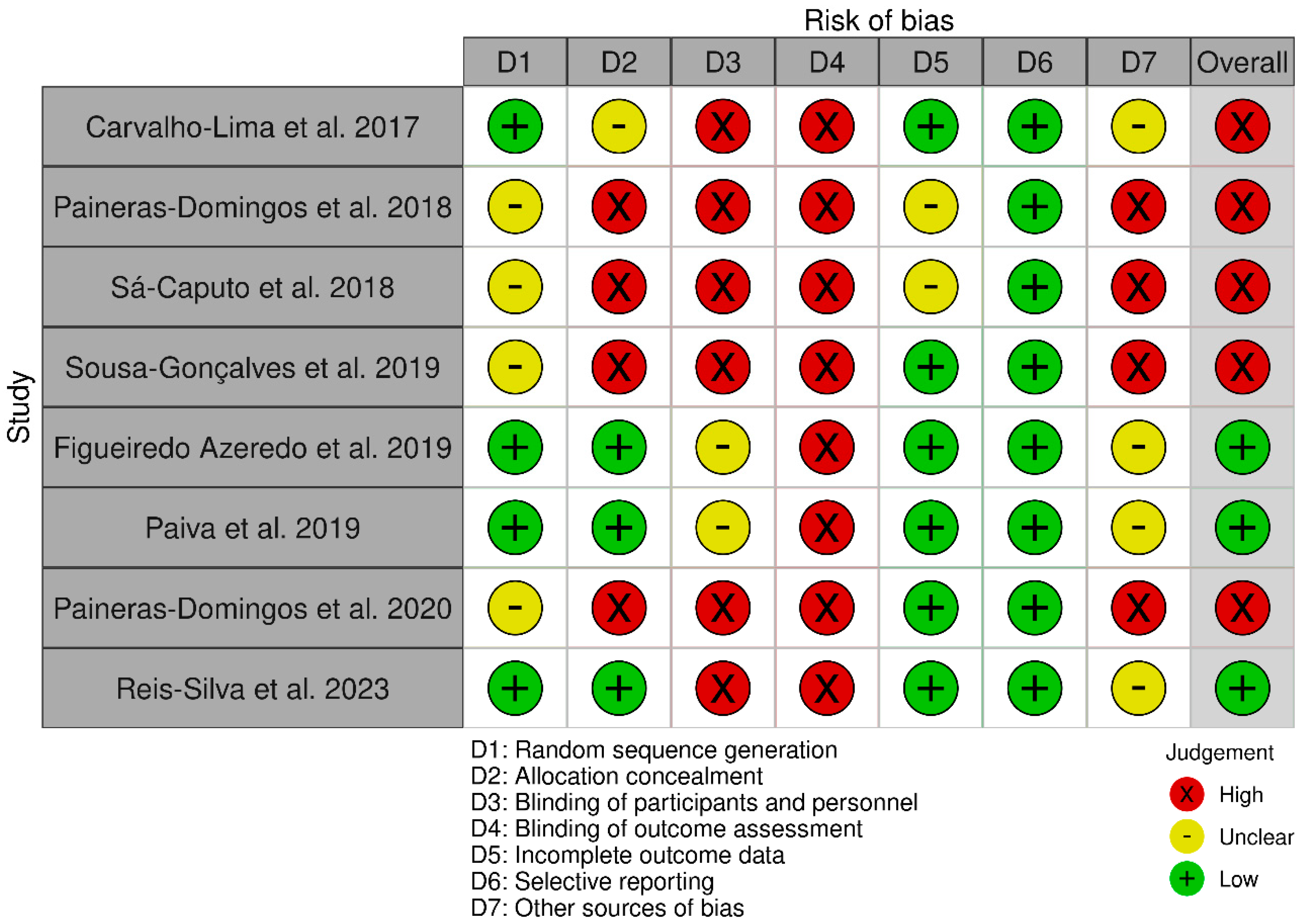
2.6. Methodological Quality and Risk of Bias
2.7. Statistical Analysis
3. Results
3.1. Results of the Systematic Review
3.2. Results of the Meta-Analysis
4. Discussion
4.1. Strengths
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sousa-Gonçalves, C.; Paineiras-Domingos, L.L.; Teixeira-Silva, Y.; Amadeu, T.; Lírio, A.P.; Francisca-Santos, A.; De Souza, L.F.F.; Pereira, M.J.; Melo-Oliveira, M.E.; Meirelles, A.; et al. Evaluation of Whole-Body Vibration Exercise on Neuromuscular Activation Through Electromyographic Pattern of Vastus Lateralis Muscle and on Range of Motion of Knees in Metabolic Syndrome: A Quasi-Randomized Cross-Over Controlled Trial. Appl. Sci. 2019, 9, 4997. [Google Scholar] [CrossRef] [Green Version]
- Motamed, S.; Mazidi, M.; Safarian, M.; Ghayour-Mobarhan, M.; Moohebati, M.; Ebrahimi, M.; Azarpazhooh, M.R.; Heidari-Bakavoli, A.; Esmaily, H.; Baghestani, A.; et al. Macronutrient intake and physical activity levels in individuals with and without metabolic syndrome: An observational study in an urban population. ARYA Atheroscler. 2019, 15, 136–145. [Google Scholar] [CrossRef]
- Carriere, I.; Peres, K.; Ancelin, M.L.; Gourlet, V.; Berr, C.; Barberger-Gateau, P.; Bouillon, K.; Kivimaki, M.; Ritchie, K.; Akbaraly, T. Metabolic syndrome and disability: Findings from the prospective three-city study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Frisman, G.H.; Kristenson, M. Psychosocial status and health related quality of life in relation to the metabolic syndrome in a Swedish middle-aged population. Eur. J. Cardiovasc. Nurs. J. Work. Group Cardiovasc. Nurs. Eur. Soc. Cardiol. 2009, 8, 207–215. [Google Scholar] [CrossRef]
- Slagter, S.N.; van Vliet-Ostaptchouk, J.V.; van Beek, A.P.; Keers, J.C.; Lutgers, H.L.; van der Klauw, M.M.; Wolffenbuttel, B.H. Health-Related Quality of Life in Relation to Obesity Grade, Type 2 Diabetes, Metabolic Syndrome and Inflammation. PLoS ONE 2015, 10, e0140599. [Google Scholar] [CrossRef]
- Lian, Y.; Yuan, Q.; Wang, G.; Tang, F. Association between sleep quality and metabolic syndrome: A systematic review and meta-analysis. Psychiatry Res. 2019, 274, 66–74. [Google Scholar] [CrossRef]
- Bollinger, L.M. Potential contributions of skeletal muscle contractile dysfunction to altered biomechanics in obesity. Gait Posture 2017, 56, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Hung, C.Y.; Li, C.M.; Lin, Y.H.; Wang, T.G.; Tsai, K.S.; Han, D.S. Reduced flexibility associated with metabolic syndrome in community-dwelling elders. PLoS ONE 2015, 10, e0117167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sa-Caputo, D.C.; Paineiras-Domingos, L.L.; Oliveira, R.; Neves, M.F.T.; Brandao, A.; Marin, P.J.; Sanudo, B.; Furness, T.; Taiar, R.; Bernardo-Filho, M. Acute Effects of Whole-Body Vibration on the Pain Level, Flexibility, and Cardiovascular Responses in Individuals With Metabolic Syndrome. Dose Response 2018, 16, 1559325818802139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadducci, A.V.; de Cleva, R.; de Faria Santarém, G.C.; Silva, P.R.S.; Greve, J.M.D.; Santo, M.A. Muscle strength and body composition in severe obesity. Clinics 2017, 72, 272–275. [Google Scholar] [CrossRef]
- Hwang, H.J.; Kim, S.H. The association among three aspects of physical fitness and metabolic syndrome in a Korean elderly population. Diabetol. Metab. Syndr. 2015, 7, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briggs, M.S.; Spees, C.; Bout-Tabaku, S.; Taylor, C.A.; Eneli, I.; Schmitt, L.C. Cardiovascular risk and metabolic syndrome in obese youth enrolled in a multidisciplinary medical weight management program: Implications of musculoskeletal pain, cardiorespiratory fitness, and health-related quality of life. Metab. Syndr. Relat. Disord. 2015, 13, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golbidi, S.; Mesdaghinia, A.; Laher, I. Exercise in the metabolic syndrome. Oxidative Med. Cell. Longev. 2012, 2012, 349710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paley, C.A.; Johnson, M.I. Abdominal obesity and metabolic syndrome: Exercise as medicine? BMC Sport. Sci. Med. Rehabil. 2018, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, L.C.; Chiang, S.L.; Tzeng, W.C.; Lee, M.S.; Hung, Y.J.; Lin, C.H. Active Physical Activity Patterns Are Associated With Improved Quality of Life and Depression Status in Taiwanese Women With Metabolic Syndrome. J. Cardiovasc. Nurs. 2019, 34, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.J. Is vibration exercise a useful addition to a weight management program? Scand. J. Med. Sci. Sport. 2012, 22, 705–713. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Seixas, A.; Taiar, R.; Bernardo-Filho, M. Vibration Therapy for Health Promotion. In Complementary Therapies; Bernardo-Filho, M., Taiar, R., Sá-Caputo, D.C., Seixas, A., Eds.; IntechOpen: Rijeka, Croatia, 2022; Chapter 12. [Google Scholar] [CrossRef]
- Rauch, F.; Sievanen, H.; Boonen, S.; Cardinale, M.; Degens, H.; Felsenberg, D.; Roth, J.; Schoenau, E.; Verschueren, S.; Rittweger, J. Reporting whole-body vibration intervention studies: Recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J. Musculoskelet. Neuronal Interact. 2010, 10, 193–198. [Google Scholar]
- Carvalho-Lima, R.P.; Sa-Caputo, D.C.; Moreira-Marconi, E.; Dionello, C.; Paineiras-Domingos, L.L.; Sousa-Goncalves, C.R.; Morel, D.S.; Frederico, E.H.; Neves, M.F.; Oliveira, R.; et al. Quality of Life of Patients with Metabolic Syndrome Is Improved after Whole Body Vibration Exercises. Artic. Afr. J. Tradit. Complement. Altern. Med. 2017, 14, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo Azeredo, C.; de Castro de Paiva, P.; Azeredo, L.; Reis da Silva, A.; Francisca-Santos, A.; Liane Paineiras-Domingos, L.; Lírio Pereira da Silva, A.; Leite Bernardes-Oliveira, C.; Pessanha-Freitas, J.; Moura-Fernandes, M.; et al. Effects of Whole-Body Vibration Exercises on Parameters Related to the Sleep Quality in Metabolic Syndrome Individuals: A Clinical Trial Study. Appl. Sci. 2019, 9, 5183. [Google Scholar] [CrossRef] [Green Version]
- Paineiras-Domingos, L.L.; da Cunha Sa-Caputo, D.; Reis, A.S.; Francisca Santos, A.; Sousa-Goncalves, C.R.; Dos Anjos, E.M.; Dos Santos Pereira, M.J.; Sartorio, A.; Bernardo-Filho, M. Assessment Through the Short Physical Performance Battery of the Functionality in Individuals With Metabolic Syndrome Exposed to Whole-Body Vibration Exercises. Dose Response 2018, 16, 1559325818794530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paineiras-Domingos, L.L.; Sá-Caputo, D.D.C.; Francisca-Santos, A.; Reis-Silva, A.; Carvalho-Lima, R.P.; Neves, M.F.T.; Xavier, V.L.; Quinart, H.; Boyer, F.C.; Sartorio, A.; et al. Can whole body vibration exercises promote improvement on quality of life and on chronic pain level of metabolic syndrome patients? A pseudorandomized crossover study. J. Appl. Physiol. 2020, 128, 934–940. [Google Scholar] [CrossRef]
- Paiva, P.C.; Figueiredo, C.A.; Reis-Silva, A.; Francisca-Santos, A.; Paineiras-Domingos, L.L.; Martins-Anjos, E.; Melo-Oliveira, M.E.S.; Lourenco-Revelles, G.M.G.; Moreira-Marconi, E.; Guedes-Aguiar, E.O.; et al. Acute and Cumulative Effects With Whole-Body Vibration Exercises Using 2 Biomechanical Conditions on the Flexibility and Rating of Perceived Exertion in Individuals With Metabolic Syndrome: A Randomized Clinical Trial Pilot Study. Dose Response 2019, 17, 1559325819886495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sa-Caputo, D.; Paineiras-Domingos, L.L.; Francisca-Santos, A.; Dos Anjos, E.M.; Reis, A.S.; Neves, M.F.T.; Oigman, W.; Oliveira, R.; Brandao, A.; Machado, C.B.; et al. Whole-body vibration improves the functional parameters of individuals with metabolic syndrome: An exploratory study. BMC Endocr. Disord. 2019, 19, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis-Silva, A.; Coelho-Oliveira, A.C.; Martins-Anjos, E.; Moura-Fernandes, M.C.; Mulder, A.; Xavier, V.L.; Mendonça, V.A.; Lacerda, A.C.R.; Paineiras-Domingos, L.L.; Taiar, R.; et al. Impact of Two Whole-Body Vibration Exercise Protocols on Body Composition of Patients with Metabolic Syndrome: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 436. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Costantino, G.; Montano, N.; Casazza, G. When should we change our clinical practice based on the results of a clinical study? Searching for evidence: PICOS and PubMed. Intern. Emerg. Med. 2015, 10, 525–527. [Google Scholar] [CrossRef]
- Merlin, T.; Weston, A.; Tooher, R. Extending an evidence hierarchy to include topics other than treatment: Revising the Australian ‘levels of evidence’. BMC Med. Res. Methodol. 2009, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G.J.B. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munera, M.; Bertucci, W.; Duc, S.; Chiementin, X. Transmission of whole body vibration to the lower body in static and dynamic half-squat exercises. Sport. Biomech. 2016, 15, 409–428. [Google Scholar] [CrossRef]
- Pessoa, M.F.; Brandão, D.C.; Sá, R.B.; Barcelar, J.M.; Rocha, T.D.S.; Souza, H.C.M.; Dornelas de Andrade, A. Vibrating Platform Training Improves Respiratory Muscle Strength, Quality of Life, and Inspiratory Capacity in the Elderly Adults: A Randomized Controlled Trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Zhang, G.; Wang, Y.; Wang, X.; Zhou, H.; Li, H.; Chen, L. The effect of whole body vibration on health-related quality of life in patients with chronic conditions: A systematic review. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2019, 28, 2859–2870. [Google Scholar] [CrossRef]
- Rubio-Arias, J.Á.; Martínez-Aranda, L.M.; Andreu-Caravaca, L.; Sanz, G.; Benito, P.J.; Ramos-Campo, D.J. Effects of whole-body vibration training on body composition, cardiometabolic risk, and strength in the population who are overweight and obese: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 2442–2453. [Google Scholar] [CrossRef]
- Beavers, K.M.; Hsu, F.C.; Houston, D.K.; Beavers, D.P.; Harris, T.B.; Hue, T.F.; Kim, L.J.; Koster, A.; Penninx, B.W.; Simonsick, E.M.; et al. The role of metabolic syndrome, adiposity, and inflammation in physical performance in the Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 617–623. [Google Scholar] [CrossRef] [Green Version]
- Lamari, N.; Marino, L.C.; Cordeiro, J.A.; Pellegrini, A.M. Flexibilidade anterior do tronco no adolecente após o pico da velocidade de crescimento em estatura. Acta Ortopédica Bras. 2007, 15, 25–29. [Google Scholar] [CrossRef]
- Gay, A.; Parratte, S.; Salazard, B.; Guinard, D.; Pham, T.; Legré, R.; Roll, J.P. Proprioceptive feedback enhancement induced by vibratory stimulation in complex regional pain syndrome type I: An open comparative pilot study in 11 patients. Jt. Bone Spine 2007, 74, 461–466. [Google Scholar] [CrossRef]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Wang, W.; Zheng, J.; Chen, S.; Qiao, J.; Wang, X. Whole Body Vibration Exercise for Chronic Musculoskeletal Pain: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 2167–2178. [Google Scholar] [CrossRef] [PubMed]
- Kessler, N.J.; Hong, J. Whole body vibration therapy for painful diabetic peripheral neuropathy: A pilot study. J. Bodyw. Mov. Ther. 2013, 17, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Alavinia, S.M.; Omidvar, M.; Craven, B.C. Does whole body vibration therapy assist in reducing fat mass or treating obesity in healthy overweight and obese adults? A systematic review and meta-analyses. Disabil. Rehabil. 2021, 43, 1935–1947. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country | Demographics | Aim | Results | Level of Evidence |
|---|---|---|---|---|---|---|
| Carvalho-Lima et al., 2017 [20] | A Randomized Clinical Trial | Brazil/Spain | n = 21 (7 men/14 women) (i) CG: n = 7; (ii) WBVE1: n = 7; (iii) WBVE2: n = 7; Age 66.65 ± 2.90 years. | Evaluate the effect of WBVE on the quality of the life of individuals with MSy through the WHOQOL-BREF questionnaire. | WBVE in a protocol (one or two times per week) with a progressive and increased frequency improves the quality of life of patients with MSy in different domains of the WHOQOL-BREF. | II |
| Paineiras-Domingos et al., 2018 [22] | Pseudo-randomized controlled trial study | Brazil/Italy | n = 39 (i) WBVEeG: n = 22 (ii) CG: n = 17; Age 47 to 69 years. | Evaluate functionality through SPPB in individuals with MSy after WBVE. | WBVE is a feasible physical activity for individuals with Msy. Through the adhesion to this type of aerobic activity, some functional parameters such as balance, gait, and lower limb strength are improved. Consequently, a better quality of life can be offered to these individuals, contributing to what is advocated as intervention strategy in this syndrome: a change to a better lifestyle. | III-1 |
| Sá-Caputo et al., 2018 [9] | Pseudo-randomized controlled Trial | Brazil/France/Spain/Australia | n = 44 (i) CG: n = 15 Age 58.20 ± 9.11 years BM 87.43 ± 18.02 kg (ii) WBVE exercise: n = 29 Age 61.10 ± 8.39 years, BM 83.65 ± 16.27 kg | Assess the acute effect of WBVE exercise, with low frequency (5 Hz), on the pain level, trunk flexibility, and cardiovascular responses ([BP] and [HR]) in individuals with Msy. | WBVE exposure with low frequency (5 Hz) is responsible in inducing physiological parameters that contribute to decrease the PL and to increase the flexibility as well as to maintain cardiovascular responses (HR and BP) in individuals with Msy. | III-1 |
| Sousa-Gonçalves et al., 2019 [1] | Quasi-randomized and cross-over controlled trial study | Brazil/France/Italy | n = 39 (i) CG: n = 17 Age 58.1 ± 2.07 years, BM 88.8 ± 4.08 kg (ii) TG: n = 22 Age 60.7 ± 1.91 years, BM:83.1 ± 3.65 kg. | Analyze the effects of WBVE on Msy individuals’ neuromuscular activation using the sEMG pattern RMS of the VL muscle and on the ROM of the knees. | WBVE can be a modality of exercise to increase the neuromuscular activity of the VL muscle using a 5-week protocol. An increase in ROM of the knees in individuals with Msy was not observed with the same protocol. WBVE appears to be an adequate strategy to improve neuromuscular activity in individuals with Msy, overweight, and obesity, being a potential opportunity for the management of physical impairment in these individuals. Nevertheless, further additional studies with larger samples and more prolonged periods of WBVE exposure are needed to confirm our preliminary findings. | III-1 |
| Figueiredo-Azeredo et al., 2019 [21] | Cross-sectional and randomized study | Brazil//France/Italy | n = 19 (i) GFF: n = 9 (ii) GVF: n = 10 Age 58.79 ± 12.55 years Height: 1.62 ± 0.09 m BM: 86.27 ± 15.03 kg | Investigate the effect of WBVE exercise on parameters related to the sleep quality in MSy individuals. | WBVE intervention was capable of interfering with physiological mechanisms with effects on the WC and HR, leading to the improvement of the quality of sleep in MSy individuals. WBVE exercise might be an important clinical intervention for the management of some factors associated with poor quality of sleep (FFG and VFG) and in the daytime sleepiness in MSy individuals with variable frequencies (5–16 Hz). | II |
| Paiva et al., 2019 [24] | Randomized clinical trial pilot study | Brazil/France/Italy/New Zealand | n = 19 patients Age 58.79 ± 12.55 years Height: 1.62 ± 0.09 m BM: 86.27 ± 15.03 kg | Evaluate the acute and cumulative effects from 6 weeks of WBVE exercise using 2 biomechanical conditions [FF] and [VF]) on flexibility and RPE in MSy individuals. | WBVE exercise improved the flexibility and decreased the RPE in MSy individuals. These findings suggest that WBVE exercise can be incorporated into physical activities for MSy individuals. | II |
| Paineiras-Domingos et al., 2020 [23] | Pseudo-randomized crossover study | Brazil/France/Italy | n = 33 patients (i) WBVEeG, n = 17, (15 women/02 men) Age 61.1 ± 8.4 years (ii) CG, n = 16,(14 women/02 men) Age 58.2 ± 9.1 years | Evaluate the effects of WBVE on quality of life and chronic pain in individuals MSy. | WBVE in MSy individuals is capable significantly (i) to promote na improvement of QoL considering the physical and psychological domains, as accumulative effect and (ii) to reduce CPL in the acute interventions in the first and in the last sessions. Therefore, WBVE would represent a suitable and useful physical activity that could be included in health programs for MSy individuals, following the WHO recommendations. | III-1 |
| Reis-Silva et al., 2022 [26] | Randomized controlled trial | Brazil/France/Italy | n = 22 patients (16 women/6 men), FFG-WBVE (n = 12; median age = 50.50 years and BMI = 31.95 kg/m2) VFG-WBVE (n = 10; median age = 57.50 years and BMI = 32.50 kg/m2) | Investigate the effects of two 6-week WBVE protocols on body composition in patients with MSy. | 6-weeks of VFG-WBVE, performed actively, can positively modify body composition in individuals with MSy. The improvement in fat mass, on the left and right arms and trunk, is clinically noteworthy, since the reduction of this fat tissue can contribute to improvements in metabolic health and reduce the cardiovascular risk factor. | II |
| Study | WBVE Intervention | Parameters | Type of Vibrating Platform | Positioning | Time WBVE |
|---|---|---|---|---|---|
| Carvalho-Lima et al., 2017 [20] | 10 weeks WBVE1 one time per week; WBVE2 twice times per week. | CG: platform turn off; WBVE1/WBVE2: Peak-to-peak displacements of (2.5, 5.0, and 7.5 mm), frequency progressively 5 Hz–14 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | 1 session/week: sat in a chair placed in in front of the platform with flexion of the knees. Their feet were on the platform base in three positions. (5 Hz). 2–10 session/week: squat position and the frequency was progressively increased by one unit for each session (6 Hz–14 Hz). | The work time was 1 min with 1 min rest in each peak-to-peak. This sequence was repeated two more times in each session. |
| Paineiras-Domingos et al., 2018 [22] | 10 sessions | CG: platform turn off. WBVEeG: Peak-to-peak displacements of 2.5, 5.0, and 7.5 mm, frequencies ranged from 5 up to 14 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | 1 session: seated on a chair in front of the platform with hands kept on their knees and feet positioned on the base of the platform. (5 Hz). 2–10 session: standing on the base of the platform with a squat, static position (knees flexed at 130°). (6–14 Hz). | The work time was 1 min with 1 min rest in each peak-to-peak. (3 min in each amplitude, with a resting period of 1 min) (total time: 18 min/session) |
| Sá-Caputo et al., 2018 [9] | 1 session | CG: platform turn off. WBVE exercise group: Peak-to-peak displacements of 2.5, 5.0, and 7.5 mm, frequency 5 Hz and corresponding to peak accelerations of 0.12, 0.25, and 0.35 g, respectively. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | Sitting in a chair with feet on the platform with knees flexed. | 3 bouts (1 min each). The session consisted of 9-min bout of work interspersed with 1-min passive rest period between each bout (total time: 17 min). |
| Sousa-Gonçalves et al., 2019 [1] | 5 weeks (twice a week) 10 sessions | CG: platform turn off.; TG: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5–14 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | 1 session: Seated on a chair placed in front of the platform with a 130° knee flexion. Their feet, shoeless, were placed on the base of the platform, alternately in three positions. 2–10 session: Standing on the base of the platform in a squat, static position (130° knee flexion), and the frequency was progressively increased by 1 unit per session. (6–14 Hz). | The working time in each position was 1 min followed by 1 min of rest. This sequence was performed three times. |
| Figueiredo-Azeredo et al., 2019 [21] | 6 weeks (twice a week) | FFG: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5 Hz. WBVE Group: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5–16 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | Squat position, barefoot and with (130° knee flexion). Dynamic and static squats interspersed sessions. | FFG performed 60 s of vibration (10 s of vibration and 110 s of non-vibration) and 60 s of non-vibration in each bout and WBVE Group performed 60 s of vibration and 60 s of non-vibration in each bout. From 1 to 4 weeks were performed 3 bouts in each session, (total time:18 min); From 5 to 8 weeks, were performed 4 bouts in each session (total time: 24 min); From 9 to 12 weeks were performed 5 bouts in each session, (total time:30 min). |
| Paiva et al., 2019 [24] | 6 weeks (twice a week) 12 sessions | FF-WBVE: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5 Hz. VF-WBVE: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5–16 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | Dynamic and static squats interspersed sessions (start 1st with static squat). | FF-WBVE: 10 s plus 50 s with the vibration machine turned off (1 min) in the squat position and rested for 1 min. Performed 3 times in the first and second weeks (total time:18 min). In the third and fourth weeks, the sequence was performed 4 times (total time:24 min) and in the fifth and sixth weeks, 5 times (total time: 30 min). VF-WBVE: 1 min with the vibration machine turned on and rested for 1 min. Performed 3 times in the first week (total time of 18 min), 5 Hz (1th session), and 6 Hz (2th session); in the second week (total time:18 min), 7 Hz (3th session) and 8 Hz (4th session); in the third week (total time: 24 min), 9 Hz (5th session) and 10 Hz (6th session); in the fourth week (total time:24 min), 11 Hz (7th session) and 12 Hz (8th session); in the fifth week (total time:30 min), 13 Hz (9th session) and 14 Hz (10th session); and in the sixth week (total time: 30 min), 15 Hz (11th session) and 16 Hz (12th session). |
| Paineiras-Domingos et al., 2020 [23] | 10 weeks 10 sessions | CG: platform turn off. WBVEeG: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5–14 Hz. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | 1 session: Seated on a chair placed in front of the platform with a 130° knee flexion. Their feet, shoeless, were placed on the base of the platform, alternately in three positions. 2–10 session: Standing on the base of the platform in a squat, static position (130° knee flexion), and the frequency was progressively increased by 1 unit per session. (6–14 Hz). | Work time was 1 min and 1 min rest in each position. This procedure was done three times with the total time WBVE exercise: 18 min. |
| Reis-Silva et al., 2022 [26] | 6 weeks, twice a week (12 sessions) | FFG-WBVE: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency 5 Hz in all sessions. VFG-WBVE: Peak to peak displacements of 2.5, 5.0, and 7.5 mm) and with a frequency of 5–16 Hz with an increase of 1 Hz at each session. | Side Alternating vibrating Platform. (Novaplate Fitness Evolution, DAF Produtos Hospitalares Ltd.a., São Paulo, Brazil) | The patient was positioned barefoot, in a semi-squat position with 130° knee flexion controlled by a goniometer, trunk erect, hands lightly resting on the side bar of the platform, relaxed shoulders, and head in a neutral position. The WBVE was performed statically or dynamically (in alternating sessions). | FFG-WBVE: the individual performed 1 min of WBVE (10 s with vibration and 50 s without vibration- semi squat position) and 1 min of rest) in 2.5, 5.0 and 7.5 mm PPD. This sequence was performed 3 times from the 1st to the 4th session (18 min of total time); 4 times from the 5th to the 8th session (24 min of total time) and 5 times from the 9 to the 12th session (30 min of total time). VFG-WBVE: the individual performed 1 min of WBVE (semi squat position) and 1 min of rest in 2.5-, 5.0- and 7.5-mm PPD. This sequence was performed 3 times from the 1st to the 4th session (18 min of total time); 4 times from the 5th to the 8th session (24 min of total time) and 5 times from the 9 to the 12th session (30 min of total time). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho-Oliveira, A.C.; Monteiro-Oliveira, B.B.; Gonçalves de Oliveira, R.; Reis-Silva, A.; Ferreira-Souza, L.F.; Lacerda, A.C.R.; Mendonça, V.A.; Sartorio, A.; Taiar, R.; Bernardo-Filho, M.; et al. Evidence of Use of Whole-Body Vibration in Individuals with Metabolic Syndrome: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3765. https://doi.org/10.3390/ijerph20043765
Coelho-Oliveira AC, Monteiro-Oliveira BB, Gonçalves de Oliveira R, Reis-Silva A, Ferreira-Souza LF, Lacerda ACR, Mendonça VA, Sartorio A, Taiar R, Bernardo-Filho M, et al. Evidence of Use of Whole-Body Vibration in Individuals with Metabolic Syndrome: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(4):3765. https://doi.org/10.3390/ijerph20043765
Chicago/Turabian StyleCoelho-Oliveira, Ana Carolina, Bruno Bessa Monteiro-Oliveira, Raphael Gonçalves de Oliveira, Aline Reis-Silva, Luiz Felipe Ferreira-Souza, Ana Cristina Rodrigues Lacerda, Vanessa A. Mendonça, Alessandro Sartorio, Redha Taiar, Mario Bernardo-Filho, and et al. 2023. "Evidence of Use of Whole-Body Vibration in Individuals with Metabolic Syndrome: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 4: 3765. https://doi.org/10.3390/ijerph20043765