
Evaluation of the Lebanese Adults’ Knowledge Regarding Autism Spectrum Disorder
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment
2.2. Data Collection Instrument
2.2.1. Socio-Demographic Characteristics
2.2.2. ASD Knowledge
2.2.3. Beliefs about ASD
2.3. Ethical Considerations
2.4. Data Analysis
3. Results
3.1. Participants’ Demographic Characteristics
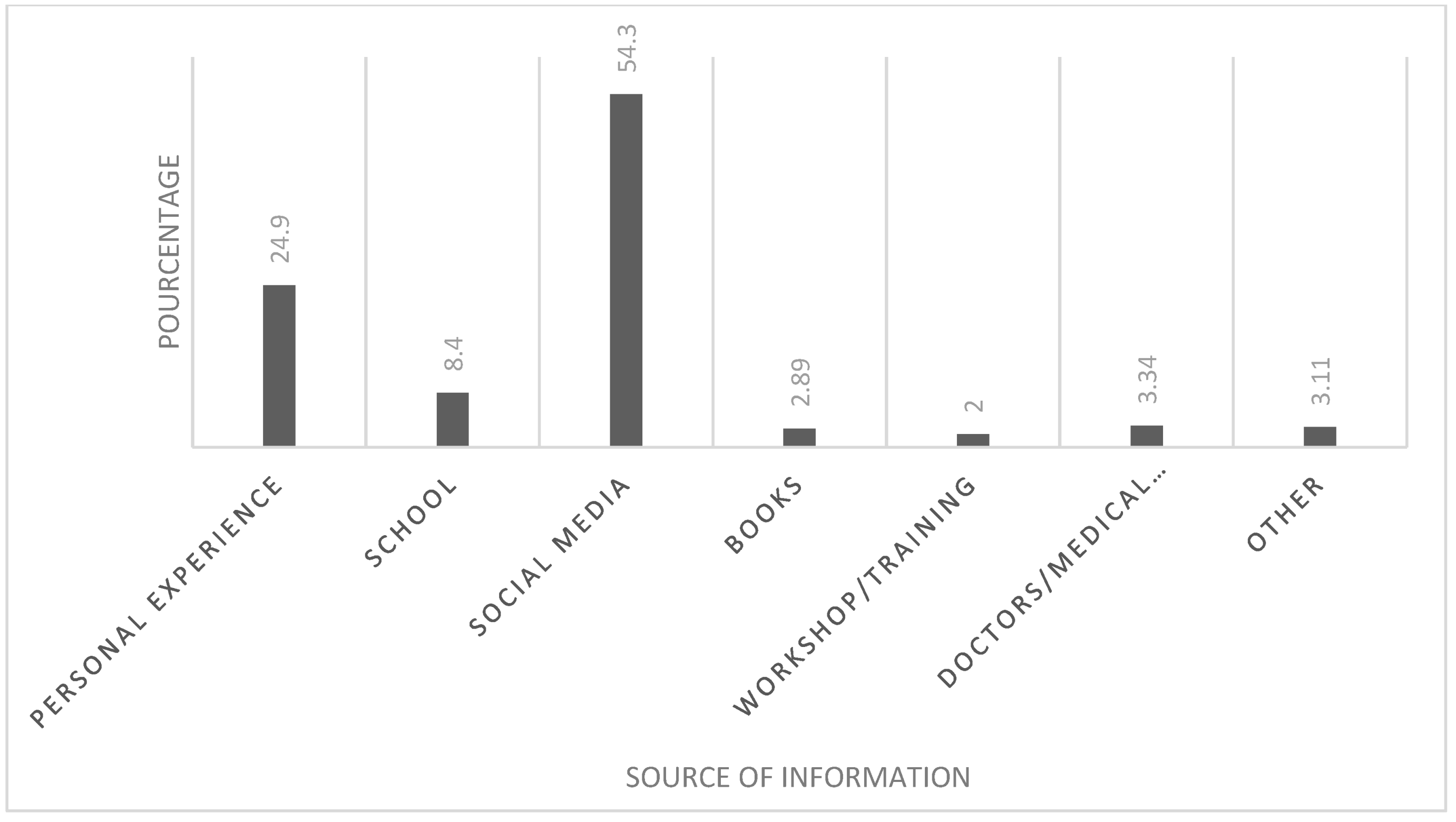
3.2. Perceived Knowledge among Participants and Their Source of Information
3.3. Actual Knowledge about ASD
3.3.1. Current State of ASD Knowledge and Beliefs
3.3.2. Participants’ Knowledge Score and Their Predictors
Total Scores and Subscales
Factors Associated with ASD Knowledge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Schuck, R.K.; Flores, R.E.; Fung, L.K. Brief Report: Sex/Gender Differences in Symptomology and Camouflaging in Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 49, 2597–2604. [Google Scholar] [CrossRef] [PubMed]
- Al-Mamri, W.; Idris, A.B.; Dakak, S.; Al-Shekaili, M.; Al-Harthi, Z.; Alnaamani, A.M.; Alhinai, F.I.; Jalees, S.; Al Hatmi, M.; El-Naggari, M.A.; et al. Revisiting the Prevalence of Autism Spectrum Disorder among Omani Children. Sultan Qaboos Univ. Med. J. 2019, 19, e305–e309. [Google Scholar] [CrossRef]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global Prevalence of Autism: A Systematic Review Update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Richa, S.; Khoury, R.; JRouhayem, J.; Chammay, R.; Kazour, F.; Bou Khalil, R.; Kheir, W.; Choueifaty, D.; Kouba-Hreich, E.; Gerbaka, B.; et al. Estimating the Prevalence of Autism Spectrum Disorder in Lebanon. Encephale 2020, 46, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Anwar, M.S.; Tahir, M.; Nusrat, K.; Khan, M.R. Knowledge, Awareness, and Perceptions Regarding Autism Among Parents in Karachi, Pakistan. Cureus 2018, 10, e3299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.E.; Locke, K.D. Lay Beliefs about Autism Spectrum Disorder among the General Public and Childcare Providers. Autism 2015, 19, 553–561. [Google Scholar] [CrossRef] [Green Version]
- Babatin, A.M.; Alzahrani, B.S.; Jan, F.M.; Alkarimi, E.H.; Jan, M.M. The Availability of Services for Children with Autism Spectrum Disorder in a Saudi Population. Neurosciences 2016, 21, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Elder, J.H.; Kreider, C.M.; Brasher, S.N.; Ansell, M. Clinical Impact of Early Diagnosis of Autism on the Prognosis and Parent–Child Relationships. Psychol. Res. Behav. Manag. 2017, 10, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Gabbay-Dizdar, N.; Ilan, M.; Meiri, G.; Faroy, M.; Michaelovski, A.; Flusser, H.; Menashe, I.; Koller, J.; Zachor, D.A.; Dinstein, I. Early Diagnosis of Autism in the Community Is Associated with Marked Improvement in Social Symptoms within 1–2 Years. Autism 2022, 26, 1353–1363. [Google Scholar] [CrossRef]
- Alharbi, K.A.; Alharbi, A.A.; Al-Thunayyan, F.S.; Alsuhaibani, K.A.; Alsalameh, N.S.; Alhomaid, M.H.; Albahouth, I.S.; Hamid, P.F. School’s Teachers Knowledge About Autism in Al-Badayacity, Al-Qassim Region, Kingdom of Saudi Arabia. Mater. Socio-Med. 2019, 31, 4–9. [Google Scholar] [CrossRef]
- Golson, M.E. Current State of Autism Knowledge in the General Population of the United States. Res. Autism Spectr. Disord. 2022, 8. [Google Scholar] [CrossRef]
- Alyami, H.S.; Naser, A.Y.; Alyami, M.H.; Alharethi, S.H.; Alyami, A.M. Knowledge and Attitudes toward Autism Spectrum Disorder in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 3648. [Google Scholar] [CrossRef]
- Alsehemi, M.A.; Abousaadah, M.M.; Sairafi, R.A.; Jan, M.M. Public Awareness of Autism Spectrum Disorder. Neurosci. J. 2017, 22, 213–215. [Google Scholar] [CrossRef] [Green Version]
- Nohra, J.; Sacre, Y.; Abdel-Nour, A.; Mannan, H. Evaluation of Knowledge, Attitudes, and Practices Related to Osteoporosis and Correlates of Perceived High Risk among People Living in Two Main Districts of Lebanon. J. Osteoporos. 2022, 2022, 1188482. [Google Scholar] [CrossRef]
- Kim, J.Y.; Son, M.J.; Son, C.Y.; Radua, J.; Eisenhut, M.; Gressier, F.; Koyanagi, A.; Carvalho, A.F.; Stubbs, B.; Solmi, M.; et al. Environmental Risk Factors and Biomarkers for Autism Spectrum Disorder: An Umbrella Review of the Evidence. Lancet Psychiatry 2019, 6, 590–600. [Google Scholar] [CrossRef] [Green Version]
- Gerges, P.; Bitar, T.; Hawat, M.; Alameddine, A.; Soufia, M.; Andres, C.R.; Hleihel, W. Risk and Protective Factors in Autism Spectrum Disorders: A Case Control Study in the Lebanese Population. Int. J. Environ. Res. Public Health 2020, 17, 6323. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Y.A.; Ahmad, M.N.; Ahmad, N.; Zakaria, N.H. Social Media for Knowledge-Sharing: A Systematic Literature Review. Telemat. Inform. 2019, 37, 72–112. [Google Scholar] [CrossRef]
- Conn, R.; Bhugra, D. The Portrayal of Autism in Hollywood Films. Int. J. Cult. Ment. Health 2012, 5, 54–62. [Google Scholar] [CrossRef]
- Rolls, K.; Massey, D. Social Media Is a Source of Health-Related Misinformation. Evid. Based Nurs. 2021, 24, 46. [Google Scholar] [CrossRef]
- Baig, M.; Jameel, T.; Alzahrani, S.H.; Mirza, A.A.; Gazzaz, Z.J.; Ahmad, T.; Baig, F.; Almurashi, S.H. Predictors of Misconceptions, Knowledge, Attitudes, and Practices of COVID-19 Pandemic among a Sample of Saudi Population. PLoS ONE 2020, 15, e0243526. [Google Scholar] [CrossRef]
- Jones, S.C.; Akram, M.; Gordon, C.S.; Murphy, N.; Sharkie, F. Autism in Australia: Community Knowledge and Autistic People’s Experiences. J. Autism Dev. Disord. 2021, 51, 3677–3689. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Stronach, S.; Harrison, A.J. Public Knowledge and Stigma of Autism Spectrum Disorder: Comparing China with the United States. Autism 2020, 24, 1531–1545. [Google Scholar] [CrossRef] [PubMed]
- May, T.; Sciberras, E.; Brignell, A.; Williams, K. Autism Spectrum Disorder: Updated Prevalence and Comparison of Two Birth Cohorts in a Nationally Representative Australian Sample. BMJ Open 2017, 7, e015549. [Google Scholar] [CrossRef] [Green Version]
- Żuk, P.; Żuk, P.; Lisiewicz-Jakubaszko, J. The Anti-Vaccine Movement in Poland: The Socio-Cultural Conditions of the Opposition to Vaccination and Threats to Public Health. Vaccine 2019, 37, 1491–1494. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Mesibov, G.B.; Shea, V. Full Inclusion and Students with Autism. J. Autism Dev. Disord. 1996, 26, 337–346. [Google Scholar] [CrossRef]
- Harrower, J.; Dunlap, G. Including Children with Autism in General Education Classrooms A Review of Effective Strategies. Behav. Modif. 2001, 25, 762–784. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Item | Response | |
|---|---|---|
| 1 | Vaccines can cause ASD | False |
| 2 | ASD is more common among boys than girls | True |
| 3 | ASD is caused by emotional deprivation from the mother | False |
| 4 | Children with siblings who have ASD are at a higher risk of developing the disorder | True |
| 5 | Advanced maternal age is a risk factor of ASD | True |
| 6 | Advanced paternal age is a risk factor of ASD | True |
| 7 | There are no differences in the identification rate of ASD across regional, racial and ethnic groups | False |
| 8 | All individuals with ASD have low intellectual quotient (IQ) | False |
| 9 | Children with ASD may not play with things the way they are intended | True |
| 10 | Children with ASD may have strict routines or rituals | True |
| 11 | Individuals with ASD have difficulties interacting socially with others | True |
| 12 | Individuals with ASD may be uncoordinated or clumsy | True |
| 13 | Individuals with ASD have difficulties expressing themselves | True |
| 14 | Symptoms of ASD do not appear before the age of 2 years | False |
| 15 | Diagnosis of ASD is primarily based on behavioral observations and parents’ interviews | True |
| 16 | ASD can only be diagnosed after the age of 4 years | False |
| 17 | ASD can be diagnosed using brain imaging only | False |
| 18 | For a diagnosis of ASD, symptoms must be present from early childhood | True |
| 19 | It is possible for ASD to develop in adulthood | False |
| 20 | There are no beneficial interventions for individuals with ASD | False |
| 21 | Restricting certain food (e.g., gluten) and giving supplements (vitamin D, magnesium…) are an effective intervention for ASD | True |
| 22 | Social skills (visual support, role-play, video-modelling…) training is an effective intervention for individuals with ASD | True |
| 23 | Individuals with ASD can learn to speak | True |
| 24 | Individuals with ASD have difficulties living and working independently in adulthood | True |
| 25 | Up to 70% of individuals with ASD also have an additional mental health such as anxiety, depression, obsessive-compulsive disorder OCD, attention Deficit Hyperactivity Disorder ADHD | True |
| 26 | All individuals with ASD display aggressive behavior | False |
| 27 | Individuals with ASD experience sleep disturbances | True |
| 28 | Individuals with ASD experience feeding problems | True |
| 29 | Individuals with ASD experience gastrointestinal problems | True |
| 30 | Individuals with ASD experience epilepsy | True |
| 31 | After being diagnosed and treated, symptoms of ASD such as delayed language and movement skills, learning skills remain stable throughout an individual’s life | False |
| 32 | After being diagnosed and treated, metabolic syndromes such as mitochondrial disorder, creatine deficiency, purine metabolism disorder remain stable throughout an individual’s life | False |
| Variable | N | Percentage (%) |
|---|---|---|
| Gender | ||
| Female | 343 | 68.6 |
| Male | 148 | 29.6 |
| Prefer not to say | 9 | 1.8 |
| Age | ||
| 18–24 | 114 | 22.8 |
| 25–34 | 120 | 24 |
| 35–49 | 169 | 33.8 |
| 50 and above | 97 | 19.4 |
| Marital status | ||
| Single | 238 | 47.6 |
| Married | 237 | 47.4 |
| Divorced | 7 | 1.4 |
| Widowed | 12 | 2.4 |
| Prefer not to say | 6 | 1.2 |
| Highest education level | ||
| Primary education | 3 | 0.6 |
| Intermediate education | 20 | 4 |
| Secondary education | 84 | 16.8 |
| Bachelor degree | 154 | 30.8 |
| Master degree | 202 | 40.4 |
| Doctorate | 33 | 6.6 |
| No degree | 2 | 0.4 |
| Prefer not to say | 2 | 0.4 |
| Region of residence | ||
| Akkar | 4 | 0.8 |
| North | 64 | 12.8 |
| Baalback | 7 | 1.4 |
| Bekaa | 15 | 3 |
| Mount Lebanon | 341 | 68.2 |
| Beirut | 51 | 10.2 |
| Nabatieh | 1 | 0.2 |
| South | 14 | 2.8 |
| Prefer not to say | 3 | 0.6 |
| Variable | N | Percentage (%) |
|---|---|---|
| Have you heard about Autism Spectrum Disorder? | ||
| Yes | 444 | 88.8 |
| No | 56 | 11.2 |
| If yes, how would you rate your understanding of ASD? | ||
| Very little understanding | 211 | 42.2 |
| Some understanding | 199 | 39.8 |
| Very familiar with autism | 40 | 8 |
| Are you aware about any special centers for children with ASD in Lebanon? | ||
| Yes | 229 | 45.8 |
| No | 271 | 54.2 |
| Do you know someone who has ASD? | ||
| Yes | 174 | 34.8 |
| No | 326 | 65.2 |
| If yes, please indicate the relationship | ||
| Family member | 30 | 17.14 |
| Friends’ family | 65 | 37.14 |
| Colleagues’ family | 80 | 45.71 |
| How would you define ASD? | ||
| Psychiatric disorder | 76 | 15.2 |
| Emotional disorder | 31 | 6.2 |
| Behavioral/social disorder | 224 | 44.8 |
| Neurodevelopmental disorder | 169 | 33.8 |
| Item | True Response N (%) | False Response N (%) |
|---|---|---|
| Domain 1: Etiology and prevalence | ||
| Vaccines can cause ASD | 238 (47.6%) | 262 (52.4%) |
| ASD is more common among boys than girls | 175 (35.0%) | 325 (65.0%) |
| ASD is caused by emotional deprivation from the mother | 266 (53.2%) | 234 (46.8%) |
| Children with siblings who have ASD are at a higher risk of developing the disorder | 87 (17.4%) | 413 (82.6%) |
| Advanced maternal age is a risk factor of ASD | 105 (21.0%) | 395 (79.0%) |
| Advanced paternal age is a risk factor of ASD | 57 (11.4%) | 443 (88.6%) |
| There are no differences in the identification rate of ASD across regional, racial and ethnic groups | 87 (17.4%) | 413 (82.6%) |
| Domain 2: Symptoms and associated behaviors | ||
| All individuals with ASD have low intellectual quotient (IQ) | 344 (68.8%) | 156 (31.2%) |
| Children with ASD may not play with things the way they are intended | 356 (71.2%) | 144 (28.8%) |
| Children with ASD may have strict routines or rituals | 427 (85.4%) | 73 (14.6%) |
| Individuals with ASD have difficulties interacting socially with others | 319 (63.8%) | 181 (36.2%) |
| Individuals with ASD may be uncoordinated or clumsy | 390 (78.0%) | 110 (22.0%) |
| Individuals with ASD have difficulties expressing themselves | 363 (72.6%) | 137 (27.4%) |
| Symptoms of ASD do not appear before the age of 2 years | 102 (20.4%) | 398 (79.6%) |
| All individuals with ASD display aggressive behavior | 83 (16.6%) | 417 (83.4%) |
| Individuals with ASD experience sleep disturbances | 70 (14.0%) | 430 (86%) |
| Individuals with ASD experience feeding problems | 287 (57.4%) | 213 (42.6%) |
| Individuals with ASD experience gastrointestinal problems | 150 (30%) | 350 (70%) |
| Individuals with ASD experience epilepsy | 137 (27.4%) | 363 (72.6%) |
| Domain 3: Assessment and diagnosis | ||
| Diagnosis of ASD is primarily based on behavioral observations and parents’ interviews | 329 (65.8%) | 171 (34.2%) |
| ASD can only be diagnosed after the age of 4 years | 214 (42.8%) | 286 (57.2%) |
| ASD can be diagnosed using brain imaging only | 188 (37.6%) | 312 (62.4%) |
| For a diagnosis of ASD, symptoms must be present from early childhood | 199 (39.8%) | 301 (60.2%) |
| It is possible for ASD to develop in adulthood | 53 10.6%) | 447 (89.4%) |
| Domain 4: Treatment | ||
| There are no beneficial interventions for individuals with ASD | 209 (41.8%) | 291 (58.2%) |
| Restricting certain food (e.g., gluten) and giving supplements (vitamin D, magnesium…) are an effective intervention for ASD | 84 (16.8%) | 416 (83.2%) |
| Social skills (visual support, role-play, video-modelling…) training is an effective intervention for individuals with ASD | 396 (79.2%) | 104 (20.8%) |
| Domain 5: Outcomes and prognosis | ||
| Individuals with ASD can learn to speak | 369 (73.8%) | 131 (26.2%) |
| Individuals with ASD have difficulties living and working independently in adulthood | 259 (51.8%) | 241 (48.2%) |
| Up to 70% of individuals with ASD also have an additional mental health such as anxiety, depression, obsessive-compulsive disorder OCD, attention Deficit Hyperactivity Disorder ADHD | 284 (56.8%) | 216 (43.2%) |
| After being diagnosed and treated, symptoms of ASD such as delayed language and movement skills, learning skills remain stable throughout an individual’s life | 125 (25%) | 375 (75%) |
| After being diagnosed and treated, metabolic syndromes such as mitochondrial disorder, creatine deficiency, purine metabolism disorder remain stable throughout an individual’s life | 57 (11.4%) | 443 (88.6%) |
| Scale | Number of Items | Mean (SD) | Percentage (%) | Level of Knowledge |
|---|---|---|---|---|
| Knowledge about etiology and prevalence | 7 | 2.03 (1.63) | 29 | Poor |
| Knowledge about symptoms and associated behaviors | 12 | 6.24 (2.91) | 52 | Moderate |
| Knowledge about assessment and diagnosis | 5 | 1.96 (1.42) | 39.2 | Poor |
| Knowledge about treatment | 3 | 1.38 (0.858) | 26 | Poor |
| Knowledge about outcomes and prognosis | 5 | 2.17 (1.35) | 43.4 | Poor |
| Total score for all items | 32 | 13.8 (6.69) | 43.1 | Poor |
| Variables | Knowledge | |||
|---|---|---|---|---|
| Poor Knowledge | Moderate Knowledge | Good Knowledge | ||
| N (%) | N (%) | N (%) | ||
| Gender | Female | 170 (34%) | 75 (15%) | 98 (19.6%) |
| Male | 111 (22.2%) | 15 (3%) | 22 (4.4%) | |
| Prefer not to say | 6 (1.2%) | 2 (4.6%) | 1 (0.2%) | |
| p-value | <0.001 * | |||
| Age | 18–24 | 64 (12.8%) | 19 (3.65%) | 31 (6.2%) |
| 25–34 | 55 (11%) | 23 (4.6%) | 42 (8.4%) | |
| 35–49 | 103 (20.6%) | 35 (7%) | 31 (6.2%) | |
| 50 and above | 65 (13%) | 15 (3%) | 17 (3.4%) | |
| p-value | 0.012 * | |||
| Marital status | Single | 138 (27%) | 41 (8.2%) | 59 (11.8%) |
| Married | 133 (26.6%) | 45 (9%) | 59 (11.8%) | |
| Divorced | 5 (1%) | 2 (0.4%) | 0 (0%) | |
| Widowed | 9 (1.8%) | 1 (0.2%) | 2 (0.4%) | |
| Prefer not to say | 2 (0.4%) | 3 (0.6%) | 1 (0.2%) | |
| p-value | 0.404 | |||
| Region of residence | North | 1 (0.2%) | 1 (0.2%) | 2 (0.4%) |
| Baalback | 27 (5.4%) | 10 (2%) | 27 (5.4%) | |
| Bekaa | 5 (1%) | 1 (0.2%) | 1 (0.2%) | |
| Mount Lebanon | 12 (2.4%) | 1 (0.2%) | 2 (0.4%) | |
| Beirut | 205 (41%) | 66 (13.2%) | 73 (14.6%) | |
| Nabatieh | 32 (6.4%) | 8 (1.6%) | 11 (2.2%) | |
| South | 0 (0%) | 0 (0%) | 1 (0.2%) | |
| Prefer not to say | 5 (1%) | 5 (1%) | 4 (0.8%) | |
| p-value | 0.026 * | |||
| Highest education level | Primary education | 2 (0.4%) | 1 (0.2%) | 0 (0%) |
| Intermediate education | 14 (2.8%) | 4 (0.8%) | 2 (0.4%) | |
| Secondary education | 58 (11.6%) | 13 (2.6%) | 13 (2.6%) | |
| Bachelor degree | 90 (18%) | 23 (4.6%) | 41 (8.2%) | |
| Master degree | 110 (22%) | 44 (8.8%) | 48 (9.6%) | |
| Doctorate | 11 (2.2%) | 7 (1.4%) | 15 (3%) | |
| No degree | 1 (0.2%) | 0 (0%) | 1 (0.2%) | |
| Prefer not to say | 1 (0.2%) | 0 (0%) | 1 (0.2%) | |
| p-value | 0.062 | |||
| ASD case | Family’s member | 8 (1.6%) | 7 (1.4%) | 15 (3%) |
| Friends’ member | 27 (5.4%) | 15 (3%) | 23 (4.6%) | |
| Colleagues’ member | 31 (6.2%) | 17 (3.4%) | 32 (6.4%) | |
| p-value | <0.001 * | |||
| Source of information | Personal experience | 51 (10.2%) | 20 (4%) | 41 (8.2%) |
| School | 22 (4.4%) | 9 (1.8%) | 11 (2.2%) | |
| Media | 153 (30.6%) | 47 (9.4%) | 44 (8.8%) | |
| Books | 5 (1%) | 5 (1%) | 3 (0.6%) | |
| Workshops | 0 (0%) | 2 (0.4%) | 7 (1.4%) | |
| Doctor | 2 (0.4%) | 3 (0.6%) | 10 (2%) | |
| other | 5 (1%) | 4 (0.8%) | 5 (1%) | |
| p-value | <0.001 * | |||
| Independent Variables | p-Value | 95% Confidence Intervals | |
|---|---|---|---|
| Lower Limit | Upper Limit | ||
| Age | 0.000 | −3.973 | −1.753 |
| Gender | 0.012 | −1.236 | −0.156 |
| Region of residence | 0.026 | −0.942 | −0.062 |
| ASD case | 0.000 | −2.450 | −1.202 |
| Source of information | 0.002 | −0.712 | −0.153 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouphael, M.; Gerges, P.; Andres, C.; Sacre, Y.; Bitar, T.; Hleihel, W. Evaluation of the Lebanese Adults’ Knowledge Regarding Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2023, 20, 4622. https://doi.org/10.3390/ijerph20054622
Rouphael M, Gerges P, Andres C, Sacre Y, Bitar T, Hleihel W. Evaluation of the Lebanese Adults’ Knowledge Regarding Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2023; 20(5):4622. https://doi.org/10.3390/ijerph20054622
Chicago/Turabian StyleRouphael, Melissa, Perla Gerges, Christian Andres, Yonna Sacre, Tania Bitar, and Walid Hleihel. 2023. "Evaluation of the Lebanese Adults’ Knowledge Regarding Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 20, no. 5: 4622. https://doi.org/10.3390/ijerph20054622