

Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. The Patient
1.2. Biomechanics
1.3. Surgical Treatment Approaches
1.4. Non-Operative Treatment Approach
1.5. Clinical Decision-Making
1.6. Aim
1.7. Method
2. Definitions
2.1. Massive Rotator Cuff Tear
2.2. Irreparable Rotator Cuff Tears
2.3. Ways to Identify Massive Irreparable Rotator Cuff Tears
- Tendon retraction
- 2.
- Fatty infiltration
- 3.
- Acromiohumeral distance
- 4.
- Positive tangent sign
2.4. Pseudoparesis versus Pseudoparalysis
3. What Constitutes the Best Physiotherapy Program?
4. How Successful Are Physiotherapy Exercise Programs in Patients with MIRCT?
5. What Are the Predictors of a Successful or Unsuccessful Response to Physiotherapy in Patients with MIRCT?
6. Discussion
6.1. Distinguishing between Predictors of Treatment Effect and Prognostic Factors
6.2. An Over-Emphasis on Biomechanical Factors
6.3. What Are the Methodological Challenges of Prognosis Studies?
7. Conclusions and Recommendations
7.1. Recommendations for Future Research
- Delphi study to gain expert consensus on possible predictors of response to physiotherapy in patients with MIRCT. This qualitative work should include exploration of patients’ perspectives on this question.
- Randomized controlled trials to compare different physiotherapy programs for MIRCT with each other, with surgical procedures, or with a no-treatment group.
- Evaluation of the effect of physiotherapy exercises on their purported biomechanical aims, e.g., anterior deltoid hypertrophy, teres minor hypertrophy, and reduction of superior migration of the head of the humerus.
- Evaluation of the biomechanical properties of patients with MIRCT who are asymptomatic.
- Longitudinal prospective prognostic studies including a wide range of possible predictors of response to physiotherapy in patients with MIRCT.
7.2. Recommendations to Improve Clarity of Terminology
7.3. Clinical Recommendations
8. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitchell, C.; Adebajo, A.; Hay, E.; Carr, A. Shoulder pain: Diagnosis and management in primary care. BMJ 2005, 331, 1124–1128. [Google Scholar] [CrossRef]
- Tashjian, R.Z. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin. Sports Med. 2012, 31, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J. Rotator cuff related shoulder pain: Assessment, management and uncertainties. Man. Ther. 2016, 23, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Denard, P.J.; Ladermann, A.; Jiwani, A.Z.; Burkhart, S.S. Functional outcome after arthroscopic repair of massive rotator cuff tears in individuals with pseudoparalysis. Arthroscopy 2012, 28, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Thes, A.; Hardy, P.; Bak, K. Decision-making in massive rotator cuff tear. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 449–459. [Google Scholar] [CrossRef]
- Hollinshead, R.M.; Mohtadi, N.G.; Vande Guchte, R.A.; Wadey, V.M. Two 6-year follow-up studies of large and massive rotator cuff tears: Comparison of outcome measures. J. Shoulder Elb. Surg. 2000, 9, 373–381. [Google Scholar] [CrossRef]
- Ladermann, A.; Collin, P.; Athwal, G.S.; Scheibel, M.; Zumstein, M.A.; Nourissat, G. Current concepts in the primary management of irreparable posterosuperior rotator cuff tears without arthritis. EFORT Open Rev. 2018, 3, 200–209. [Google Scholar] [CrossRef]
- Camenzind, R.S.; Lafosse, L.; Lafosse, T. Pseudoparalysis and pseudoparesis of the shoulder. Obere Extrem. 2021, 16, 237–246. [Google Scholar] [CrossRef]
- Tokish, J.M.; Alexander, T.C.; Kissenberth, M.J.; Hawkins, R.J. Pseudoparalysis: A systematic review of term definitions, treatment approaches, and outcomes of management techniques. J. Shoulder Elb. Surg. 2017, 26, e177–e187. [Google Scholar] [CrossRef]
- Akhtar, A.; Richards, J.; Monga, P. The biomechanics of the rotator cuff in health and disease—A narrative review. J. Clin. Orthop. Trauma 2021, 18, 150–156. [Google Scholar] [CrossRef]
- Wiater, J.M.; Fabing, M.H. Shoulder arthroplasty: Prosthetic options and indications. J. Am. Acad. Orthop. Surg. 2009, 17, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Gerber, C.; Pennington, S.D.; Nyffeler, R.W. Reverse total shoulder arthroplasty. J. Am. Acad. Orthop. Surg. 2009, 17, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Samitier, G.; Alentorn-Geli, E.; Torrens, C.; Wright, T.W. Reverse shoulder arthroplasty. Part 1: Systematic review of clinical and functional outcomes. Int. J. Shoulder Surg. 2015, 9, 24–31. [Google Scholar] [CrossRef]
- Mulieri, P.; Dunning, P.; Klein, S.; Pupello, D.; Frankle, M. Reverse shoulder arthroplasty for the treatment of irreparable rotator cuff tear without glenohumeral arthritis. J. Bone Jt. Surg. Am. 2010, 92, 2544–2556. [Google Scholar] [CrossRef]
- Hartzler, R.U.; Steen, B.M.; Hussey, M.M.; Cusick, M.C.; Cottrell, B.J.; Clark, R.E.; Frankle, M.A. Reverse shoulder arthroplasty for massive rotator cuff tear: Risk factors for poor functional improvement. J. Shoulder Elb. Surg. 2015, 24, 1698–1706. [Google Scholar] [CrossRef]
- Muh, S.J.; Streit, J.J.; Wanner, J.P.; Lenarz, C.J.; Shishani, Y.; Rowland, D.Y.; Riley, C.; Nowinski, R.J.; Edwards, T.B.; Gobezie, R. Early follow-up of reverse total shoulder arthroplasty in patients sixty years of age or younger. J. Bone Jt. Surg. Am. 2013, 95, 1877–1883. [Google Scholar] [CrossRef]
- Juhan, T.; Stone, M.; Jalali, O.; Curtis, W.; Prodromo, J.; Weber, A.E.; Hatch, G.F., III; Omid, R. Irreparable rotator cuff tears: Current treatment options. Orthop. Rev. (Pavia) 2019, 11, 8146. [Google Scholar] [CrossRef]
- Shepet, K.H.; Liechti, D.J.; Kuhn, J.E. Nonoperative treatment of chronic, massive irreparable rotator cuff tears: A systematic review with synthesis of a standardized rehabilitation protocol. J. Shoulder Elb. Surg. 2020, 30, 1431–1444. [Google Scholar]
- Kucirek, N.K.; Hung, N.J.; Wong, S.E. Treatment Options for Massive Irreparable Rotator Cuff Tears. Curr. Rev. Musculoskelet. Med. 2021, 30, 1431–1444. [Google Scholar] [CrossRef]
- Schumaier, A.P.; Bedeir, Y.H.; Dines, J.S.; Kenter, K.; Gulotta, L.V.; Dines, D.M.; Grawe, B.M. Quantifying the Impact of Patient-Specific Factors and Disease Severity on Clinical Decision Making in Cuff Tear Arthropathy: A Case-Based Survey. HSS J. 2019, 15, 276–285. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Thorne, S.; Malterud, K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur. J. Clin. Investig. 2018, 48, e12931. [Google Scholar] [CrossRef]
- Cofield, R.H. Rotator cuff disease of the shoulder. JBJS 1985, 67, 974–979. [Google Scholar]
- Ladermann, A.; Denard, P.J.; Collin, P. Massive rotator cuff tears: Definition and treatment. Int. Orthop. 2015, 39, 2403–2414. [Google Scholar] [CrossRef]
- Patte, D. Classification of rotator cuff lesions. Clin. Orthop. Relat. Res. 1990, 254, 81–86. [Google Scholar]
- Bedi, A.; Dines, J.; Warren, R.F.; Dines, D.M. Massive tears of the rotator cuff. J. Bone Jt. Surg. Am. 2010, 92, 1894–1908. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Danaceau, S.M.; Pearce, C.E., Jr. Arthroscopic rotator cuff repair: Analysis of results by tear size and by repair technique-margin convergence versus direct tendon-to-bone repair. Arthroscopy 2001, 17, 905–912. [Google Scholar] [CrossRef]
- Lo, I.K.; Burkhart, S.S. Arthroscopic revision of failed rotator cuff repairs: Technique and results. Arthroscopy 2004, 20, 250–267. [Google Scholar] [CrossRef]
- Henry, P.; Wasserstein, D.; Park, S.; Dwyer, T.; Chahal, J.; Slobogean, G.; Schemitsch, E. Arthroscopic Repair for Chronic Massive Rotator Cuff Tears: A Systematic Review. Arthroscopy 2015, 31, 2472–2480. [Google Scholar] [CrossRef]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Thomazeau, H.; Boukobza, E.; Morcet, N.; Chaperon, J.; Langlais, F. Prediction of rotator cuff repair results by magnetic resonance imaging. Clin. Orthop. Relat. Res. 1997, 344, 275–283. [Google Scholar] [CrossRef]
- Sheean, A.J.; Hartzler, R.U.; Denard, P.J.; Ladermann, A.; Sanders, T.G.; Zlatkin, M.B.; Burkhart, S.S. Preoperative Radiographic Risk Factors for Incomplete Arthroscopic Supraspinatus Tendon Repair in Massive Rotator Cuff Tears. Arthroscopy 2018, 34, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.J.; Lansdown, D.A.; Cheung, S.; Feeley, B.T.; Ma, C.B. The relationship between tear severity, fatty infiltration, and muscle atrophy in the supraspinatus. J. Shoulder Elb. Surg. 2013, 22, 18–25. [Google Scholar] [CrossRef]
- Kim, I.B.; Jung, D.W.; Suh, K.T. Prediction of the Irreparability of Rotator Cuff Tears. Arthroscopy 2018, 34, 2076–2084. [Google Scholar] [CrossRef]
- Saupe, N.; Pfirrmann, C.W.; Schmid, M.R.; Jost, B.; Werner, C.M.; Zanetti, M. Association between rotator cuff abnormalities and reduced acromiohumeral distance. AJR Am. J. Roentgenol. 2006, 187, 376–382. [Google Scholar] [CrossRef]
- Ernstbrunner, L.; El Nashar, R.; Favre, P.; Bouaicha, S.; Wieser, K.; Gerber, C. Chronic Pseudoparalysis Needs to Be Distinguished From Pseudoparesis: A Structural and Biomechanical Analysis. Am. J. Sports Med. 2021, 49, 291–297. [Google Scholar] [CrossRef]
- Fahey, C.J.; Delaney, R.A. Exploring expert variability in defining pseudoparalysis: An international survey. J. Shoulder Elb. Surg. 2021, 30, e237–e244. [Google Scholar] [CrossRef]
- Ainsworth, R.; Lewis, J.; Conboy, V. A Prospective Randomized Placebo Controlled Clinical Trial of a Rehabilitation Programme for Patients with a Diagnosis of Massive Rotator Cuff Tears of the Shoulder. Shoulder Elb. 2009, 1, 55–60. [Google Scholar] [CrossRef]
- Christensen, B.H.; Andersen, K.S.; Rasmussen, S.; Andreasen, E.L.; Nielsen, L.M.; Jensen, S.L. Enhanced function and quality of life following 5 months of exercise therapy for patients with irreparable rotator cuff tears—An intervention study. BMC Musculoskelet. Disord. 2016, 17, 252. [Google Scholar] [CrossRef]
- Levy, O.; Mullett, H.; Roberts, S.; Copeland, S. The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears. J. Shoulder Elb. Surg. 2008, 17, 863–870. [Google Scholar] [CrossRef]
- Yian, E.H.; Sodl, J.F.; Dionysian, E.; Schneeberger, A.G. Anterior deltoid reeducation for irreparable rotator cuff tears revisited. J. Shoulder Elb. Surg. 2017, 26, 1562–1565. [Google Scholar] [CrossRef]
- Collin, P.; Matsumura, N.; Ladermann, A.; Denard, P.J.; Walch, G. Relationship between massive chronic rotator cuff tear pattern and loss of active shoulder range of motion. J. Shoulder Elb. Surg. 2014, 23, 1195–1202. [Google Scholar] [CrossRef]
- Gutiérrez-Espinoza, H.; Arriagada-Núñez, V.; Araya-Quintanilla, F.; Zavala-González, J.; Rubio-Oyarzún, D.; Sfeir-Castro, R.; Gana-Hervias, G. Physical therapy in patients over 60 years of age with a massive and irreparable rotator cuff tear: A case series. J. Phys. Ther. Sci. 2018, 30, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Klintberg, I.H.; Cools, A.M.; Holmgren, T.M.; Holzhausen, A.C.; Johansson, K.; Maenhout, A.G.; Moser, J.S.; Spunton, V.; Ginn, K. Consensus for physiotherapy for shoulder pain. Int. Orthop. 2015, 39, 715–720. [Google Scholar] [CrossRef]
- Agout, C.; Berhouet, J.; Spiry, C.; Bonnevialle, N.; Joudet, T.; Favard, L.; French Arthroscopic, S. Functional outcomes after non-operative treatment of irreparable massive rotator cuff tears: Prospective multicenter study in 68 patients. Orthop. Traumatol. Surg. Res. 2018, 104, S189–S192. [Google Scholar] [CrossRef]
- Collin, P.G.; Gain, S.; Nguyen Huu, F.; Ladermann, A. Is rehabilitation effective in massive rotator cuff tears? Orthop. Traumatol. Surg. Res. 2015, 101, S203–S205. [Google Scholar] [CrossRef]
- Lewis, J.; McCreesh, K.; Roy, J.S.; Ginn, K. Rotator Cuff Tendinopathy: Navigating the Diagnosis-Management Conundrum. J. Orthop. Sports Phys. Ther. 2015, 45, 923–937. [Google Scholar] [CrossRef]
- Littlewood, C.; Malliaras, P.; Bateman, M.; Stace, R.; May, S.; Walters, S. The central nervous system—An additional consideration in ‘rotator cuff tendinopathy’ and a potential basis for understanding response to loaded therapeutic exercise. Man. Ther. 2013, 18, 468–472. [Google Scholar] [CrossRef]
- Wattanaprakornkul, D.; Cathers, I.; Halaki, M.; Ginn, K.A. The rotator cuff muscles have a direction specific recruitment pattern during shoulder flexion and extension exercises. J. Sci. Med. Sport 2011, 14, 376–382. [Google Scholar] [CrossRef]
- Ferreira, P.H.; Ferreira, M.L.; Maher, C.G.; Refshauge, K.M.; Latimer, J.; Adams, R.D. The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys. Ther. 2013, 93, 470–478. [Google Scholar] [CrossRef]
- Chester, R.; Jerosch-Herold, C.; Lewis, J.; Shepstone, L. Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: A multicentre longitudinal cohort study. Br. J. Sports Med. 2018, 52, 269–275. [Google Scholar] [CrossRef]
- Kovacevic, D.; Suriani, R.J., Jr.; Grawe, B.M.; Yian, E.H.; Gilotra, M.N.; Hasan, S.A.; Srikumaran, U.; Hasan, S.S.; Cuomo, F.; Burks, R.T.; et al. Management of irreparable massive rotator cuff tears: A systematic review and meta-analysis of patient-reported outcomes, reoperation rates, and treatment response. J. Shoulder Elb. Surg. 2020, 29, 2459–2475. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Espinoza, H.J.; Lorenzo-García, P.; Valenzuela-Fuenzalida, J.; Araya-Quintanilla, F. Functional outcomes after physiotherapy program in patients with massive and irreparable rotator cuff tear. Rev. Española De Cirugía Ortopédica Y Traumatol. 2021, 65, 248–254. [Google Scholar] [CrossRef]
- Keating, J.F.; Waterworth, P.; Shaw-Dunn, J.; Crossan, J. The relative strengths of the rotator cuff muscles. A cadaver study. J. Bone Jt. Surg. Br. 1993, 75, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Omi, R.; Sano, H.; Ohnuma, M.; Kishimoto, K.N.; Watanuki, S.; Tashiro, M.; Itoi, E. Function of the shoulder muscles during arm elevation: An assessment using positron emission tomography. J. Anat. 2010, 216, 643–649. [Google Scholar] [CrossRef]
- Collin, P.; Ladermann, A.; Le Bourg, M.; Walch, G. Subscapularis minor--an analogue of the Teres minor? Orthop. Traumatol. Surg. Res. 2013, 99, S255–S258. [Google Scholar] [CrossRef]
- Yoon, T.H.; Kim, S.J.; Choi, C.H.; Yoon, S.P.; Chun, Y.M. An intact subscapularis tendon and compensatory teres minor hypertrophy yield lower failure rates for non-operative treatment of irreparable, massive rotator cuff tears. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3240–3245. [Google Scholar] [CrossRef]
- Araya-Quintanilla, F.; Gutierrez-Espinoza, H.; Gana-Hervias, G.; Cavero-Redondo, I.; Alvarez-Bueno, C. Association between type of rotator cuff tear and functional outcomes in patients with massive and irreparable rotator cuff tear: A pre-post intervention study. J. Shoulder Elb. Surg. 2021, 30, 1393–1401. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, A.D.; Windt, D.A.; Riley, R.D.; Abrams, K.; Moons, K.G.; Steyerberg, E.W.; Schroter, S.; Sauerbrei, W.; Altman, D.G.; Hemingway, H.; et al. Prognosis research strategy (PROGRESS) 4: Stratified medicine research. BMJ 2013, 346, e5793. [Google Scholar] [CrossRef]
- Vad, V.B.; Warren, R.F.; Altchek, D.W.; O’Brien, S.J.; Rose, H.A.; Wickiewicz, T.L. Negative prognostic factors in managing massive rotator cuff tears. Clin. J. Sport Med. 2002, 12, 151–157. [Google Scholar] [CrossRef]
- Adolfsson, J.; Steineck, G. Prognostic and treatment predictive factors. Is there a difference? Prostate Cancer Prostatic Dis. 2000, 3, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Windt, D.V.D.; Croft, P.P.; Moons, K.G.M. Prognosis Research in Healthcare: Concepts, Methods, and Impact, 1st ed.; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Dunn, W.R.; Kuhn, J.E.; Sanders, R.; An, Q.; Baumgarten, K.M.; Bishop, J.Y.; Brophy, R.H.; Carey, J.L.; Harrell, F.; Holloway, B.G.; et al. 2013 Neer Award: Predictors of failure of nonoperative treatment of chronic, symptomatic, full-thickness rotator cuff tears. J. Shoulder Elb. Surg. 2016, 25, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Boorman, R.S.; More, K.D.; Hollinshead, R.M.; Wiley, J.P.; Brett, K.; Mohtadi, N.G.; Nelson, A.A.; Lo, I.K.; Bryant, D. The rotator cuff quality-of-life index predicts the outcome of nonoperative treatment of patients with a chronic rotator cuff tear. J. Bone Jt. Surg. Am. 2014, 96, 1883–1888. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Stokes, E.K.; Gojanovic, B.; Gellatly, P.; Mbada, C.; Sharma, S.; Diener, I.; O’Sullivan, P. Reframing how we care for people with persistent non-traumatic musculoskeletal pain. Suggestions for the rehabilitation community. Physiotherapy 2021, 112, 143–149. [Google Scholar] [CrossRef]
- Hutting, N.; Caneiro, J.P.; Ong’wen, O.M.; Miciak, M.; Roberts, L. Patient-centered care in musculoskeletal practice: Key elements to support clinicians to focus on the person. Musculoskelet. Sci. Pract. 2022, 57, 102434. [Google Scholar] [CrossRef]
- Miciak, M.; Mayan, M.; Brown, C.; Joyce, A.S.; Gross, D.P. A framework for establishing connections in physiotherapy practice. Physiother. Theory Pract. 2019, 35, 40–56. [Google Scholar] [CrossRef] [PubMed]
- McCabe, E.; Miciak, M.; Roduta Roberts, M.; Sun, H.; Kleiner, M.J.; Holt, C.J.; Gross, D.P. Development of the Physiotherapy Therapeutic Relationship Measure. Eur. J. Physiother. 2021, 24, 287–296. [Google Scholar] [CrossRef]
- Hall, A.M.; Ferreira, P.H.; Maher, C.G.; Latimer, J.; Ferreira, M.L. The influence of the therapist-patient relationship on treatment outcome in physical rehabilitation: A systematic review. Phys. Ther. 2010, 90, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Rossettini, G.; Latini, T.M.; Palese, A.; Jack, S.M.; Ristori, D.; Gonzatto, S.; Testa, M. Determinants of patient satisfaction in outpatient musculoskeletal physiotherapy: A systematic, qualitative meta-summary, and meta-synthesis. Disabil. Rehabil. 2020, 42, 460–472. [Google Scholar] [CrossRef] [PubMed]
- Miciak, M.; Rossettini, G. Looking at Both Sides of the Coin: Addressing Rupture of the Therapeutic Relationship in Musculoskeletal Physical Therapy/Physiotherapy. J. Orthop. Sports Phys. Ther. 2022, 52, 500–504. [Google Scholar] [CrossRef]
- Buchbinder, R.; Page, M.J.; Huang, H.; Verhagen, A.P.; Beaton, D.; Kopkow, C.; Lenza, M.; Jain, N.B.; Richards, B.; Richards, P.; et al. A Preliminary Core Domain Set for Clinical Trials of Shoulder Disorders: A Report from the OMERACT 2016 Shoulder Core Outcome Set Special Interest Group. J. Rheumatol. 2017, 44, 1880–1883. [Google Scholar] [CrossRef]
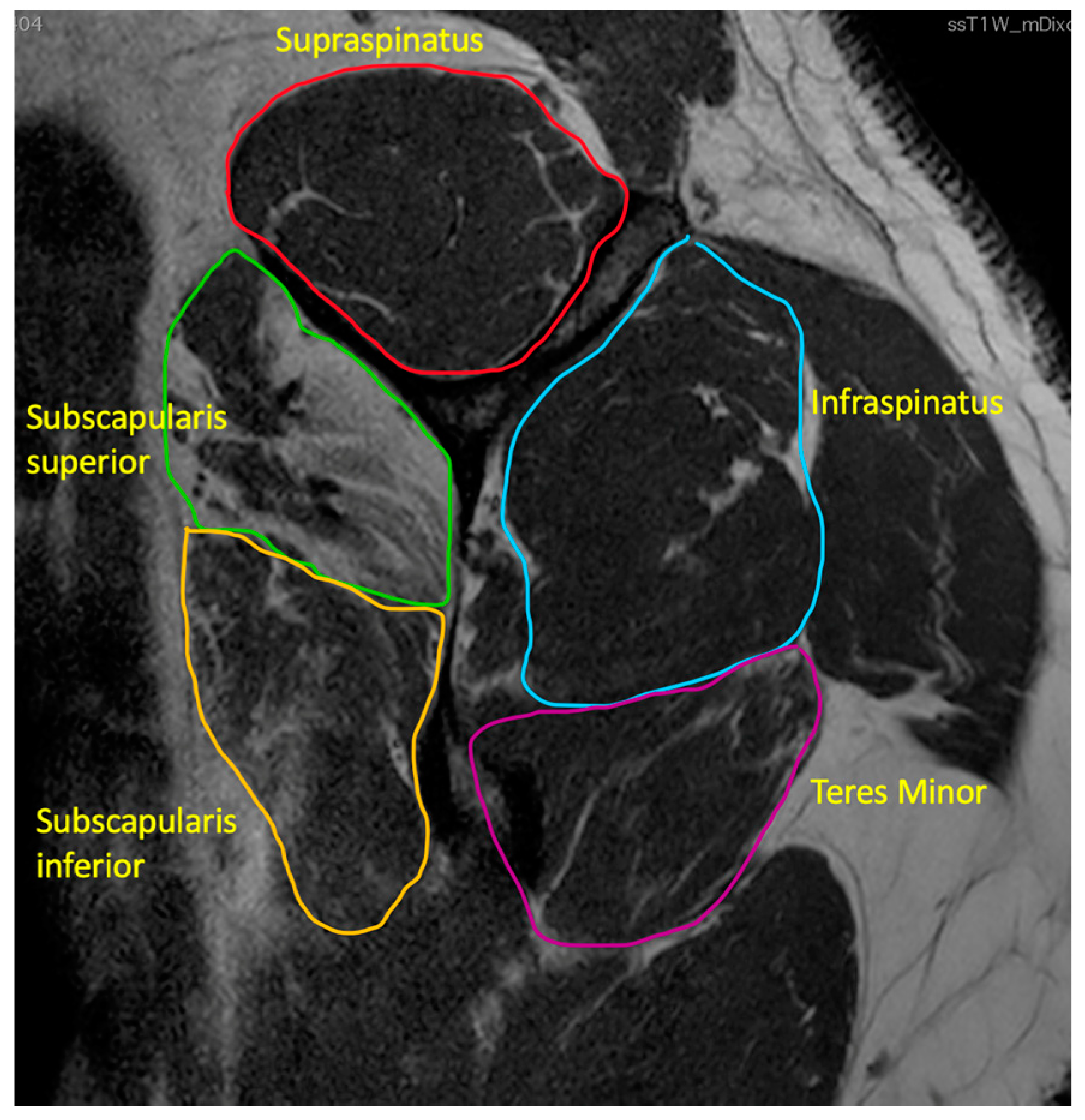
 indicates level of supraspinatus tendon retraction.
indicates level of supraspinatus tendon retraction.

 indicates supraspinatus extending above the tangent.
indicates supraspinatus extending above the tangent.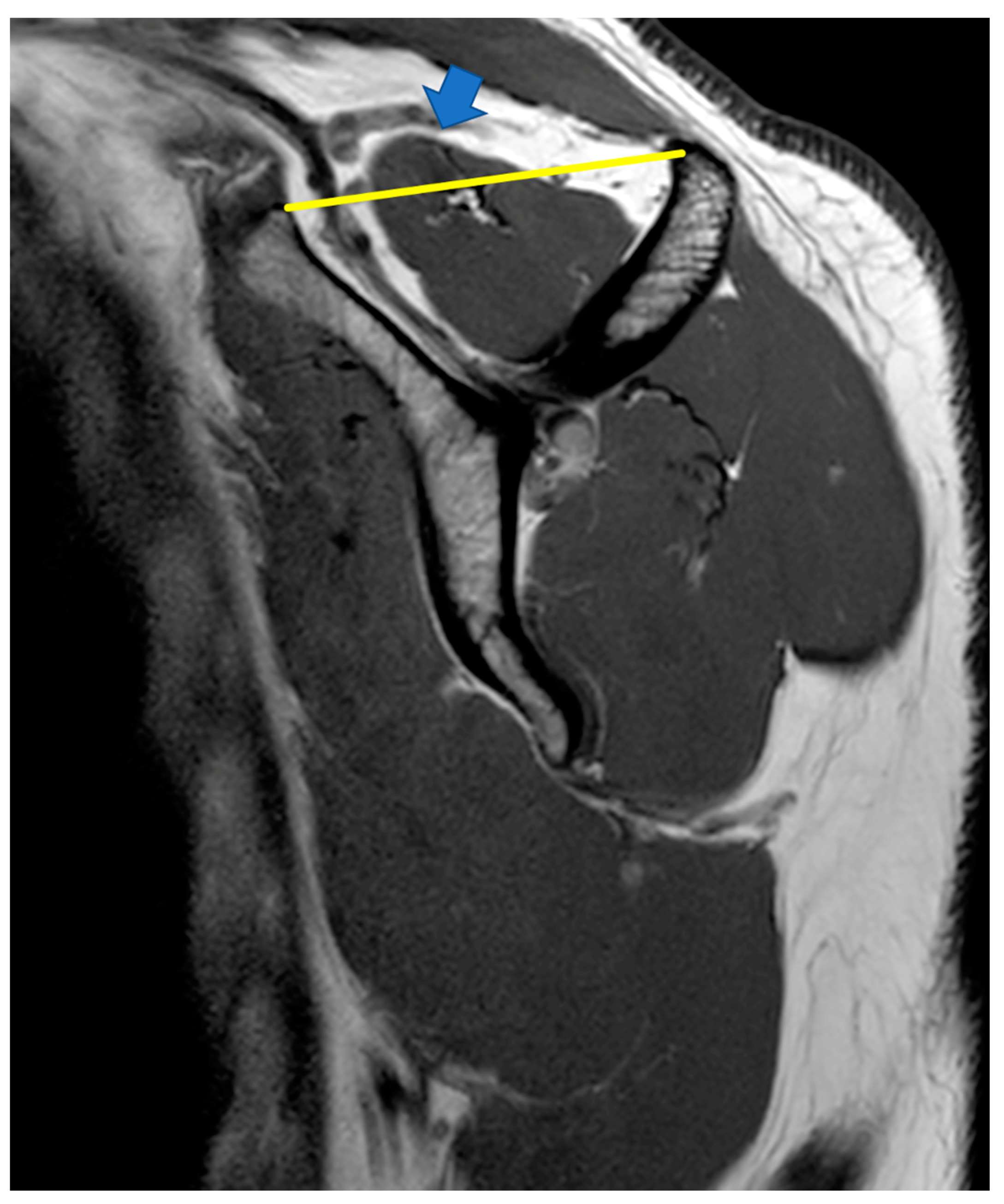

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Type | Number of Participants | Mean Age | Criteria for Defining Massive Irreparable Rotator Cuff Tear | Other Tear Types Included? | Exercise Intervention | Length of Physiotherapy Intervention | F/U Time | Definition of Successful Outcome | Definition of Failure | How Many Had Successful Outcome? | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Levy et al. (2008) [39] | Prospective case series | n = 17 | 80 (range: 70–96) | Complete rupture ≥ 2 tendons, Goutallier Grade 4 fatty infiltration, Patte Grade 3 retraction, AH distance ≤ 7 mm, pseudoparalysis | No | Anterior deltoid strengthening: well described | At least 12 weeks | 6 and 12 weeks, 6 and 9 months | Definition of successful outcome or failure unclear, but “adequate ROM” and “no pain medication” mentioned, but not defined. | 14/17 (82%) | III | |
| Yian et al. (2017) [40] | Prospective case series | n = 30 | 74 (range: 55–89) | Complete rupture ≥ 2 tendons, Goutallier Grade 4 fatty infiltration, Patte Grade 3 retraction | No | Anterior deltoid strengthening | 3 months | 9 and 24 months | Pt decision to not have surgery, >20 improvement on ASES score | Pt abandoning prog due to pain or pt’s decision to have surgery or less than 20 pt improvement on the ASES score on final follow-up | 40% | III |
| Christensen et al. (2016) [38] | Prospective case series | n = 24 (not including 6 dropouts) | 70 (range: 49–89) | Complete rupture ≥ 2 tendons, USS evaluation of tendon retraction or MRI (fatty infiltration/retraction or arthroscopic evaluation) | No | Anterior deltoid strengthening: well described | 5 months | 5 months | None | None | Not known. Mean statistical improvements only reported across PROM, QOL, strength and pain | III |
| Ainsworth et al. (2009) [37] | RCT (prospective, placebo controlled | n = 60 (6 lost to f/u) | 78 (range: 68–88) | FTT > 5 cm adjudged by surgeon to be irreparable | Yes | Anterior deltoid strengthening | 6 treatment sessions | 3,6 and 12 months | None | None | Not known, statistically significant improvement in OSS at 3 and 6 months, not significant at 12 months | I |
| Collin et al. (2015) [45] | Prospective case series | n = 45 | 67 (range: 56–76) | Complete rupture ≥ 2 tendons, Goutallier ≥ Grade 3, pseudoparalysis | No | Scapular and entire deltoid strengthening not well described | 5 physiotherapy sessions | 2 years | Not explicitly stated, but suggested significant improvement in constant score/achievement of 160º forward elevation (24/45 achieved this) | Not explicitly stated, but suggested not achieving 160° forward elevation | 24/45 (53%) | III |
| Guitierrez-Espinoza et al. (2018) [42] | Prospective case series | n = 92 | 68 (range: 63–72) | Complete rupture ≥2 tendons, Goutallier ≥Grade 3 | No | Manual therapy and specific exercises—progressive scapular and GHJ control exercises (MT joint mobilizations well described, but exercises a bit vague) | 12 weeks (x2 session/week) | 12 weeks | Statistically significant improvement | Not explicitly stated | Not known, mean statistically significant improvements shown in Constant Score, DASH and VAS | III |
| Study | Design | No. of Participants | Predictor | Predictor of Success/Failure? | Comments |
|---|---|---|---|---|---|
| Yian et al. (2017) [40] | Prospective case series | n = 30 | <40° shoulder flexion at outset of program | Failure | Design of the study was focused on evaluating success or failure of physiotherapy rather than identifying predictors of success or failure. No control group |
| Collin et al. (2015) [45] | Prospective case series | n = 45 | Tear involving subscapularis or three tendons torn. Tears isolated to posterior cuff | Failure Success | Study design focused on whether site of rotator cuff tear predicted outcome from physiotherapy, but did not use multivariate statistical analysis to consider whether other factors were involved in predicting response. No control group |
| Agout et al. (2018) [44] | Prospective case series | n = 71 | No correlation between site of tendon tears and success or failure | n/a | Study design did not use multivariate statistical analysis to test whether other factors were involved in predicting response. No control group |
| Ainsworth et al. (2009) [37] | RCT (prospective, placebo controlled | n = 60 (6 lost to f/u) | Authors hypothesised that increased teres minor recruitment was a predictor | Success | Study design did not test this hypothesis as it did not evaluate teres minor hypertrophy or recruitment |
| Yoon et al. (2019) [56] | Prospective case series | n = 108 | Intact subscapularis tendon and teres minor hypertrophy | Success | Study design did not use multivariate statistical analysis to test whether other factors were involved in predicting response. No control group |
| Araya_Quintanilla et al. (2021) [57] | Single group pre and post intervention study | n = 92 | No correlation between presence of subscapularis tear and failure of physiotherapy Long duration of symptoms, high body mass index and tobacco use | n/a Failure | Correlation shown between these factors and outcome, but values for long duration of symptoms and high body mass index not defined. No control group |
| Vad et al. (2002) [59] | Retrospective non-randomized cohort study | n = 108 | Presence of glenohumeral arthritis, decreased passive range of motion, superior migration of the humeral head, presence of muscle atrophy, and weakness of external rotation or abduction strength | Failure | Study design not appropriate to evaluate predictors of treatment effect. No control group |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ó Conaire, E.; Delaney, R.; Lädermann, A.; Schwank, A.; Struyf, F. Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review. Int. J. Environ. Res. Public Health 2023, 20, 5242. https://doi.org/10.3390/ijerph20075242
Ó Conaire E, Delaney R, Lädermann A, Schwank A, Struyf F. Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review. International Journal of Environmental Research and Public Health. 2023; 20(7):5242. https://doi.org/10.3390/ijerph20075242
Chicago/Turabian StyleÓ Conaire, Eoin, Ruth Delaney, Alexandre Lädermann, Ariane Schwank, and Filip Struyf. 2023. "Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review" International Journal of Environmental Research and Public Health 20, no. 7: 5242. https://doi.org/10.3390/ijerph20075242
APA StyleÓ Conaire, E., Delaney, R., Lädermann, A., Schwank, A., & Struyf, F. (2023). Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review. International Journal of Environmental Research and Public Health, 20(7), 5242. https://doi.org/10.3390/ijerph20075242