
REM Sleep Impairment May Underlie Sleep-Driven Modulations of Tinnitus in Sleep Intermittent Tinnitus Subjects: A Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessment
2.2.1. Anamnesis Case Report Form
2.2.2. Overnight Tinnitus Variation Assessment
2.2.3. Polysomnography Recording
2.3. Analyses
2.3.1. Polysomnography Scoring
2.3.2. Statistical Analyses
3. Results
3.1. Etiological Group Comparison
- The proportion of patients experiencing an increase of tinnitus after naps were significantly higher in the SIT group than in the Non-SIT group (p < 0.01);
- The proportion of patients complaining of neck stiffness and/or lack of cervical mobility was significantly lower for the SIT group than for the Non-SIT group (p < 0.01);
- The proportion of patients experiencing rises of tinnitus after an exposition to loud noises was significantly lower in the SIT than in the Non-SIT group (p < 0.05).
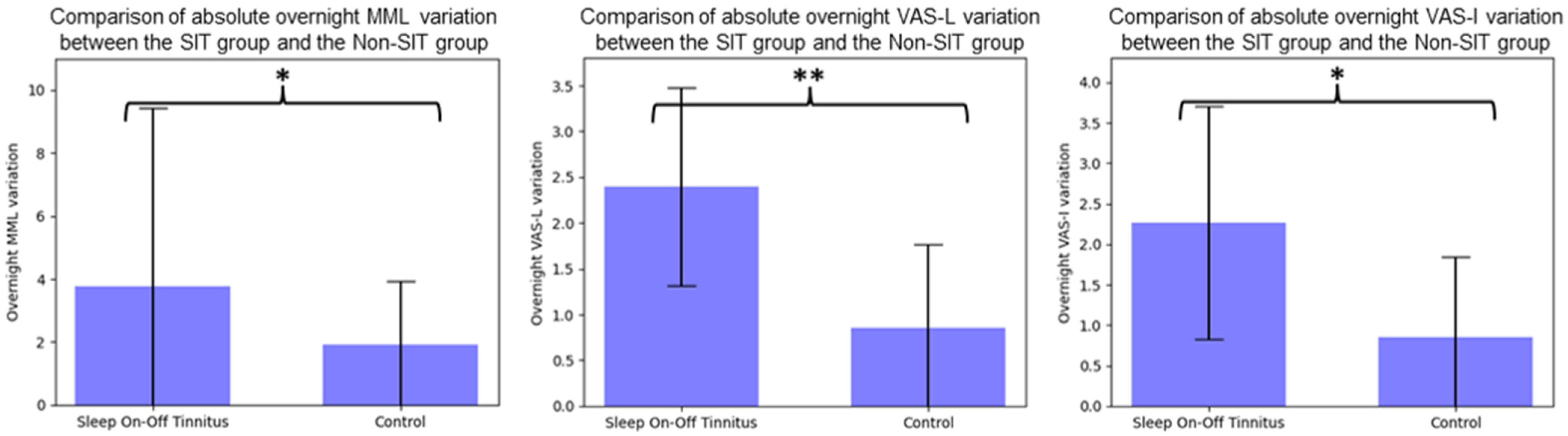
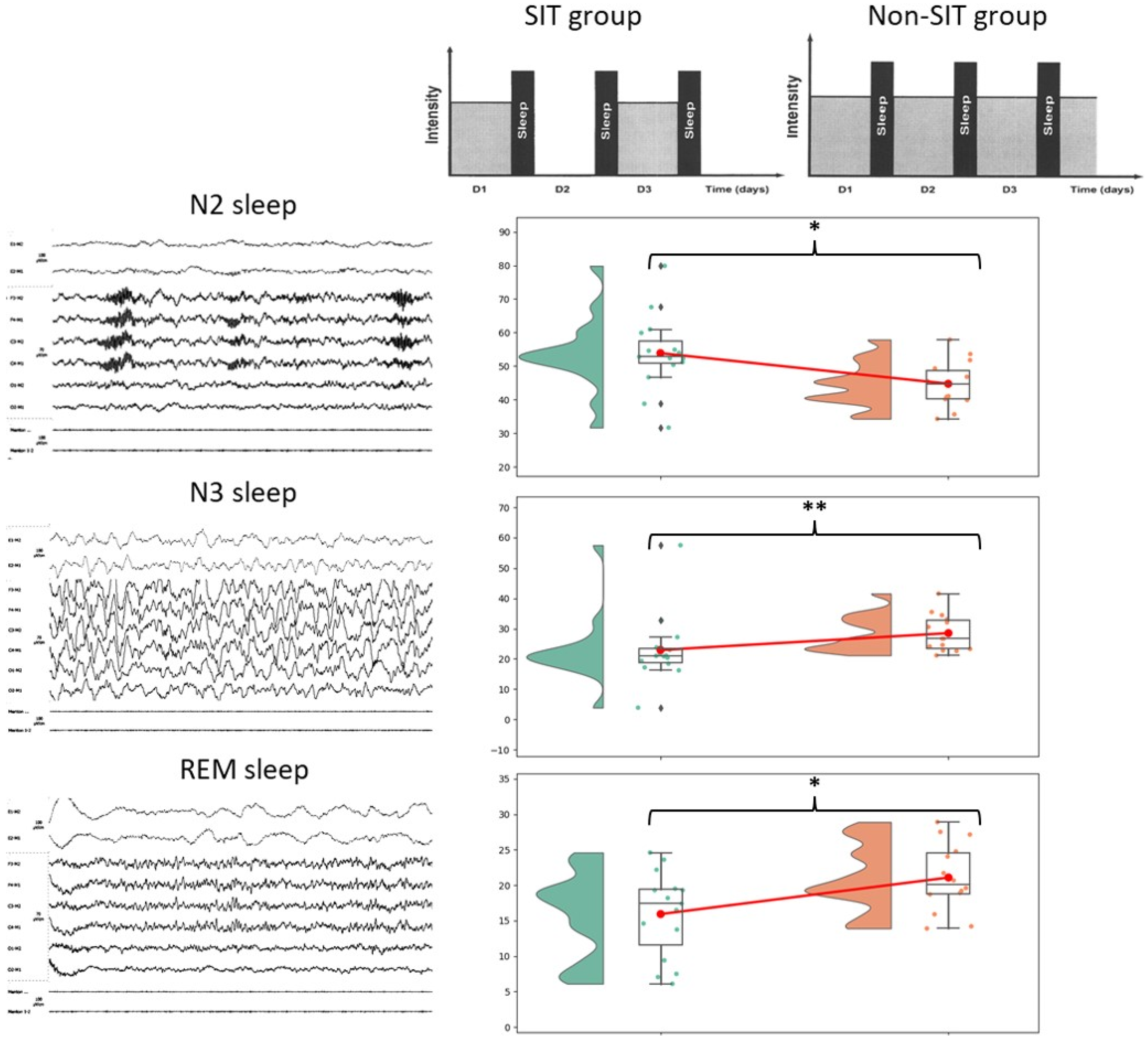
3.2. Sleep Characteristics Group Comparison
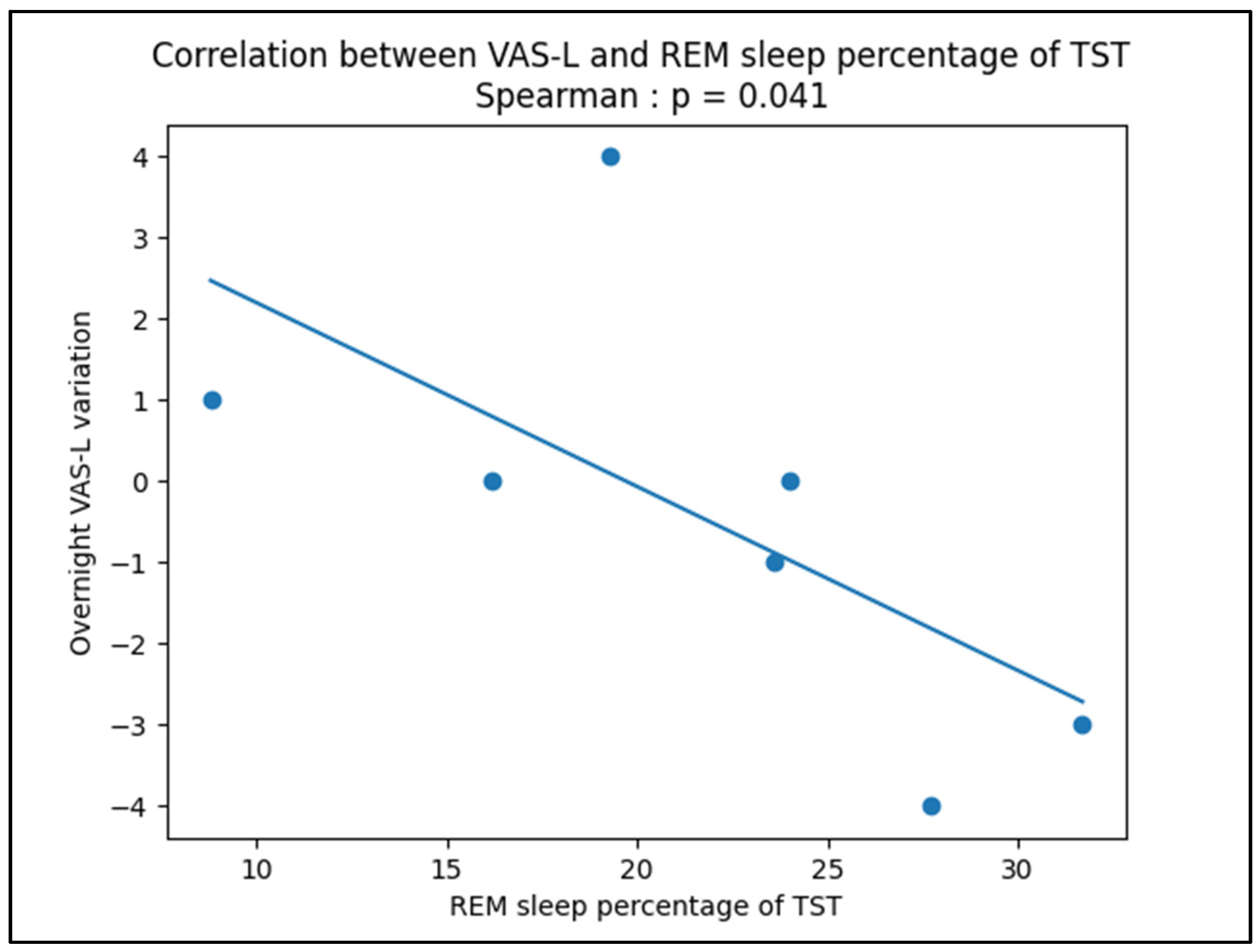
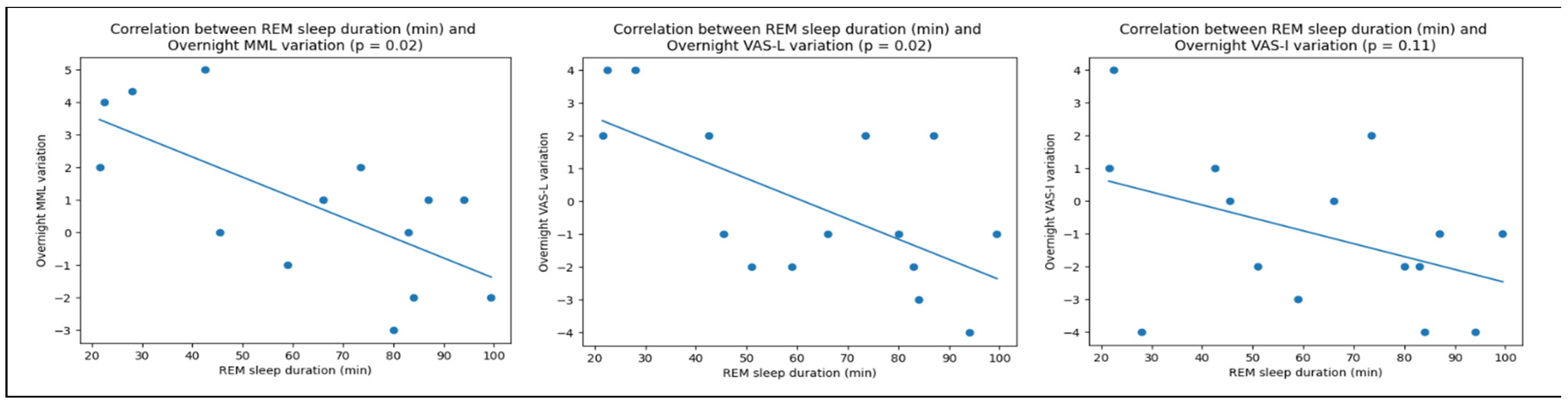
3.3. Correlations between Tinnitus Modulation and Sleep Characteristics
4. Discussion
4.1. REM Sleep Seems to Be Specifically Implicated in SIT Sleep-Driven Modulations
4.2. Merits
4.3. Limits
4.4. Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Subject Presentation
- 2.
- Polysomnographic Recordings and Methodology
- 3.
- Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VAS-L Evening | VAS-L Morning | TST | WASO | Sleep Latency | REM Latency | %N1 | %N2 | %N3 | %REM | %Snoring | %Supine | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Night 1 | 2 | 1 | 421 | 8.3 | 5.3 | 71.5 | 4.9 | 38.8 | 32.7 | 23.6 | 10.7 | 97.4 |
| Night 2 | 1 | 5 | 514.5 | 21.2 | 6.6 | 80 | 11 | 54.8 | 14.9 | 19.3 | 17.5 | 94.2 |
| Night 3 | 0 | 0 | 423 | 22.6 | 7.7 | 70.7 | 6.4 | 39.4 | 38 | 16.2 | 6.1 | 78.9 |
| Night 4 | 3 | 0 | 358 | 22.5 | 2.4 | 44.4 | 6 | 39 | 23.3 | 31.7 | 2.8 | 72.8 |
| Night 5 | 4 | 0 | 464 | 27 | 8 | 70 | 5.6 | 37.4 | 29.3 | 27.7 | 3.6 | 75.9 |
| Night 6 | 3 | 3 | 339 | 7.2 | 15.9 | 96.9 | 5.7 | 29.6 | 40.6 | 24 | 30.1 | 82.7 |
| Night 7 | 0 | 1 | 297 | 2.9 | 2.4 | 91.4 | 3.5 | 32.3 | 55.4 | 8.8 | 30.6 | 75.6 |
- 4.
- Discussion
References
- Al Lawati, N.M.; Patel, S.R.; Ayas, N.T. Epidemiology, Risk Factors, and Consequences of Obstructive Sleep Apnea and Short Sleep Duration. Prog. Cardiovasc. Dis. 2009, 51, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Itani, O.; Jike, M.; Watanabe, N.; Kaneita, Y. Short Sleep Duration and Health Outcomes: A Systematic Review, Meta-Analysis, and Meta-Regression. Sleep Med. 2017, 32, 246–256. [Google Scholar] [CrossRef] [PubMed]
- von Ruesten, A.; Weikert, C.; Fietze, I.; Boeing, H. Association of Sleep Duration with Chronic Diseases in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. PLoS ONE 2012, 7, e30972. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Dugravot, A.; Léger, D.; Ben Hassen, C.; Kivimaki, M.; Singh-Manoux, A. Association of Sleep Duration at Age 50, 60, and 70 Years with Risk of Multimorbidity in the UK: 25-Year Follow-up of the Whitehall II Cohort Study. PLoS Med. 2022, 19, e1004109. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.T.U.; Menna-Barreto, L. Diabetes and Sleep: A Complex Cause-and-Effect Relationship. Diabetes Res. Clin. Pract. 2011, 91, 129–137. [Google Scholar] [CrossRef]
- Lainsamputty, F.; Chen, H.-M. The Correlation Between Fatigue and Sleep Quality among Patients with Heart Failure. NurseLine J. 2018, 3, 100–114. [Google Scholar] [CrossRef] [Green Version]
- Alster, J.; Shemesh, Z.; Ornan, M.; Attias, J. Sleep Disturbance Associated with Chronic Tinnitus. Biol. Psychiatry 1993, 34, 84–90. [Google Scholar] [CrossRef]
- Fioretti, A.B.; Fusetti, M.; Eibenstein, A. Association between Sleep Disorders, Hyperacusis and Tinnitus: Evaluation with Tinnitus Questionnaires. Noise Health 2013, 15, 91. [Google Scholar] [CrossRef]
- Hébert, S.; Carrier, J. Sleep Complaints in Elderly Tinnitus Patients: A Controlled Study. Ear Hear. 2007, 28, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Wallhäusser-Franke, E.; Schredl, M.; Delb, W. Tinnitus and Insomnia: Is Hyperarousal the Common Denominator? Sleep Med. Rev. 2013, 17, 65–74. [Google Scholar] [CrossRef]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.-J.; Andersson, G.; et al. Chapter 1-Tinnitus and Tinnitus Disorder: Theoretical and Operational Definitions (an International Multidisciplinary Proposal). In Progress in Brain Research; Schlee, W., Langguth, B., Kleinjung, T., Vanneste, S., De Ridder, D., Eds.; Tinnitus-An Interdisciplinary Approach Towards Individualized Treatment: From Heterogeneity to Personalized Medicine; Elsevier: Amsterdam, The Netherlands, 2021; Volume 260, pp. 1–25. [Google Scholar]
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-Analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef]
- Folmer, R.L.; Griest, S.E. Tinnitus and Insomnia. Am. J. Otolaryngol. 2000, 21, 287–293. [Google Scholar] [CrossRef]
- Miguel, G.S.; Yaremchuk, K.; Roth, T.; Peterson, E. The Effect of Insomnia on Tinnitus. Ann. Otol. Rhinol. Laryngol. 2014, 123, 696–700. [Google Scholar] [CrossRef]
- Li, Y.-L.; Hsu, Y.-C.; Lin, C.-Y.; Wu, J.-L. Sleep Disturbance and Psychological Distress in Adult Patients with Tinnitus. J. Formos. Med. Assoc. 2022, 121, 995–1002. [Google Scholar] [CrossRef]
- Asnis, G.M.; Ma, H.; C, S.; M, T.; M, K.; G, R.D.L. Insomnia in Tinnitus Patients: A Prospective Study Finding a Significant Relationship. Int. Tinnitus J. 2020, 24, 65–69. [Google Scholar] [CrossRef]
- Asnis, G.M.; Majeed, K.; Henderson, M.A.; Sylvester, C.; Thomas, M.; La Garza, R.D. An Examination of the Relationship Between Insomnia and Tinnitus: A Review and Recommendations. Clin. Med. Insights Psychiatry 2018, 9, 1–8. [Google Scholar] [CrossRef]
- Axelsson, A.; Ringdahl, A. Tinnitus—A Study of Its Prevalence and Characteristics. Br. J. Audiol. 1989, 23, 53–62. [Google Scholar] [CrossRef]
- Hallam, R. Correlates of Sleep Disturbance in Chronic Distressing Tinnitus. Scand. Audiol. 1996, 25, 263–266. [Google Scholar] [CrossRef]
- Asplund, R. Sleepiness and Sleep in Elderly Persons with Tinnitus. Arch. Gerontol. 2003, 37, 139–145. [Google Scholar] [CrossRef]
- Shao, Y.; Huang, J.; Li, M. Clinical features analysis of 1240 tinnitus cases. Zhonghua Er. Bi. Yan Hou Tou Jing Wai Ke Za Zhi 2009, 44, 641–644. [Google Scholar]
- Lasisi, A.O.; Gureje, O. Prevalence of Insomnia and Impact on Quality of Life among Community Elderly Subjects with Tinnitus. Ann. Otol. Rhinol. Laryngol. 2011, 120, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Izuhara, K.; Wada, K.; Nakamura, K.; Tamai, Y.; Tsuji, M.; Ito, Y.; Nagata, C. Association between Tinnitus and Sleep Disorders in the General Japanese Population. Ann. Otol. Rhinol. Laryngol. 2013, 122, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Hébert, S.; Fullum, S.; Carrier, J. Polysomnographic and Quantitative Electroencephalographic Correlates of Subjective Sleep Complaints in Chronic Tinnitus: Sleep Complaints in Tinnitus. J. Sleep Res. 2011, 20, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.S.; Oliveira, C.A.C.; Granjeiro, R.C.; Petry, C.; Travaglia, A.B.L.; Bahmad, F. Polysomnographic Findings in Patients With Chronic Tinnitus. Ann. Otol. Rhinol. Laryngol. 2018, 127, 953–961. [Google Scholar] [CrossRef]
- Teixeira, L.S.; Granjeiro, R.C.; de Oliveira, C.A.P.; Bahamad Júnior, F.; Teixeira, L.S.; Granjeiro, R.C.; de Oliveira, C.A.P.; Bahamad Júnior, F. Polysomnography Applied to Patients with Tinnitus: A Review. Int. Arch. Otorhinolaryngol. 2018, 22, 177–180. [Google Scholar] [CrossRef] [Green Version]
- Attanasio, G.; Russo, F.Y.; Roukos, R.; Covelli, E.; Cartocci, G.; Saponara, M. Sleep Architecture Variation in Chronic Tinnitus Patients. Ear Hear. 2013, 34, 503–507. [Google Scholar] [CrossRef]
- Lu, C.-T.; Lee, L.-A.; Lee, G.-S.; Li, H.-Y. Obstructive Sleep Apnea and Auditory Dysfunction—Does Snoring Sound Play a Role? Diagnostics 2022, 12, 2374. [Google Scholar] [CrossRef]
- Burgos, I.; Feige, B.; Hornyak, M.; Härter, M.; Weske-Heck, G.; Voderholzer, U.; Riemann, D. Chronic Tinnitus and Associated Sleep Disturbances. Somnologie 2005, 9, 133–138. [Google Scholar] [CrossRef]
- Gupta, M.A. Tinnitus Severity in Posttraumatic Stress Disorder (PTSD) is Inversely Correlated with Rapid Eye Movement (REM) Sleep Percentage and Duration and Directly Correlated with Indices of Hyperarousal. Sleep 2019, 42 (Suppl. 1), A354. [Google Scholar] [CrossRef]
- Milinski, L.; Nodal, F.R.; Vyazovskiy, V.V.; Bajo, V.M. Tinnitus: At a Crossroad between Phantom Perception and Sleep. Brain Commun. 2022, 4, fcac089. [Google Scholar] [CrossRef]
- Camparis, C.M.; Formigoni, G.; Teixeira, M.J.; Siqueira, J.T.T.D. Clinical Evaluation of Tinnitus in Patients with Sleep Bruxism: Prevalence and Characteristics. J. Oral Rehabil. 2005, 32, 808–814. [Google Scholar] [CrossRef]
- Fernandes, G.; de Siqueira, J.T.T.; de Gonçalves, D.A.G.; Camparis, C.M.; Fernandes, G.; de Siqueira, J.T.T.; Gonçalves, D.A.d.G.; Camparis, C.M. Association between Painful Temporomandibular Disorders, Sleep Bruxism and Tinnitus. Braz. Oral Res. 2014, 28, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Koo, M.; Hwang, J.-H. Risk of Tinnitus in Patients with Sleep Apnea: A Nationwide, Population-Based, Case-Control Study. Laryngoscope 2017, 127, 2171–2175. [Google Scholar] [CrossRef]
- Tseng, H.-H.; Hwang, S.-W.; Hwang, S.-R.; Hwang, J.-H. Sleep Apnea Plays a More Important Role on Sleep N3 Stage than Chronic Tinnitus in Adults. Medicine 2022, 101, e30089. [Google Scholar] [CrossRef]
- Hwang, S.-W.; Chu, Y.-C.; Hwang, S.-R.; Hwang, J.-H. Association of Periodic Limb Movements during Sleep and Tinnitus in Humans. Sci. Rep. 2020, 10, 5972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, S.-R.; Hwang, S.-W.; Chu, Y.-C.; Hwang, J.-H. Association of Sleep Terror, Walking or Talking and Tinnitus. J. Formos. Med. Assoc. 2021, 120, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Cederroth, C.R.; Gallus, S.; Hall, D.A.; Kleinjung, T.; Langguth, B.; Maruotti, A.; Meyer, M.; Norena, A.; Probst, T.; Pryss, R.; et al. Editorial: Towards an Understanding of Tinnitus Heterogeneity. Front. Aging Neurosci. 2019, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Landgrebe, M.; Zeman, F.; Koller, M.; Eberl, Y.; Mohr, M.; Reiter, J.; Staudinger, S.; Hajak, G.; Langguth, B. The Tinnitus Research Initiative (TRI) Database: A New Approach for Delineation of Tinnitus Subtypes and Generation of Predictors for Treatment Outcome. BMC Med. Inf. Decis. Mak. 2010, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Langguth, B. Treatment of Tinnitus. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFerran, D.J.; Stockdale, D.; Holme, R.; Large, C.H.; Baguley, D.M. Why Is There No Cure for Tinnitus? Front. Neurosci. 2019, 13, 802. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.A.; Hibbert, A.; Smith, H.; Haider, H.F.; Londero, A.; Mazurek, B.; Fackrell, K. One Size Does Not Fit All: Developing Common Standards for Outcomes in Early-Phase Clinical Trials of Sound-, Psychology-, and Pharmacology-Based Interventions for Chronic Subjective Tinnitus in Adults. Trends Hear. 2019, 23, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Kim, S. Why the One-Size-Fits-All Approach to Tinnitus Is Not Successful. Hear. Rev. 2022, 29, 28–31. [Google Scholar]
- Beukes, E.W.; Manchaiah, V.; Allen, P.M.; Andersson, G.; Baguley, D.M. Chapter 4-Exploring Tinnitus Heterogeneity. In Progress in Brain Research; Schlee, W., Langguth, B., Kleinjung, T., Vanneste, S., De Ridder, D., Eds.; Tinnitus-An Interdisciplinary Approach towards Individualized Treatment: From Heterogeneity to Personalized Medicine; Elsevier: Amsterdam, The Netherlands, 2021; Volume 260, pp. 79–99. [Google Scholar]
- Levine, R.A.; Oron, Y. Tinnitus. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 129, pp. 409–431. ISBN 978-0-444-62630-1. [Google Scholar]
- Levine, R. Tinnitus: Diagnostic Approach Leading to Treatment. Semin. Neurol. 2013, 33, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Genitsaridi, E.; Partyka, M.; Gallus, S.; Lopez-Escamez, J.A.; Schecklmann, M.; Mielczarek, M.; Trpchevska, N.; Santacruz, J.L.; Schoisswohl, S.; Riha, C.; et al. Standardised Profiling for Tinnitus Research: The European School for Interdisciplinary Tinnitus Research Screening Questionnaire (ESIT-SQ). Hear. Res. 2019, 377, 353–359. [Google Scholar] [CrossRef]
- van den Berge, M.J.C.; Free, R.H.; Arnold, R.; de Kleine, E.; Hofman, R.; van Dijk, J.M.C.; van Dijk, P. Cluster Analysis to Identify Possible Subgroups in Tinnitus Patients. Front. Neurol. 2017, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Ralli, M.; Altissimi, G.; Turchetta, R.; Cianfrone, G. Somatic Modulation of Tinnitus: A Review and Some Open Questions. Otolaryngol. Open J. 2016, 2, 111–114. [Google Scholar] [CrossRef]
- Nicolas-Puel, C.; Faulconhridge, R.L.; Guitton, M.; Puel, J.-L.; Mondain, M.; UzieP, A. Characteristics of Tinnitus and Etiology of Associated Hearing Loss: A Study of 123 Patients. Int. Tinnitus J. 2002, 8, 37–44. [Google Scholar]
- Rauschecker, J.P.; Leaver, A.M.; Mühlau, M. Tuning Out the Noise: Limbic-Auditory Interactions in Tinnitus. Neuron 2010, 66, 819–826. [Google Scholar] [CrossRef] [Green Version]
- Guillard, R.; Decobecq, F.; Fraysse, M.-J.; Favre, A.; Congedo, M.; Loche, V.; Boyer, M.; Londero, A. Validated French Translation of the ESIT-SQ Standardized Tinnitus Screening Questionnaire. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2023. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Jurcak, V.; Tsuzuki, D.; Dan, I. 10/20, 10/10, and 10/5 Systems Revisited: Their Validity as Relative Head-Surface-Based Positioning Systems. NeuroImage 2007, 34, 1600–1611. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Rompre, P.H.; Montplaisir, J.Y. Sleep Bruxism: Validity of Clinical Research Diagnostic Criteria in a Controlled Polysomnographic Study. J. Dent. Res. 1996, 75, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Carra, M.C.; Huynh, N.; Lavigne, G.J. Diagnostic Accuracy of Sleep Bruxism Scoring in Absence of Audio-Video Recording: A Pilot Study. Sleep Breath 2015, 19, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genitsaridi, E. Novel Approaches for Tinnitus Subphenotyping: Evidence Synthesis, Standardised Assessment, and Supervised and Unsupervised Machine Learning Applications. Ph.D. Thesis, University of Nottingham, Nottingham, UK, 2021. [Google Scholar]
- Langguth, B.; Landgrebe, M.; Schlee, W.; Schecklmann, M.; Vielsmeier, V.; Steffens, T.; Staudinger, S.; Frick, H.; Frick, U. Different Patterns of Hearing Loss among Tinnitus Patients: A Latent Class Analysis of a Large Sample. Front. Neurol. 2017, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rompré, P.H.; Daigle-Landry, D.; Guitard, F.; Montplaisir, J.Y.; Lavigne, G.J. Identification of a Sleep Bruxism Subgroup with a Higher Risk of Pain. J. Dent. Res. 2007, 86, 837–842. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-Analysis of Quantitative Sleep Parameters From Childhood to Old Age in Healthy Individuals: Developing Normative Sleep Values Across the Human Lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef]
- Fagelson, M.A. The Association Between Tinnitus and Posttraumatic Stress Disorder. Am. J. Audiol. 2007, 16, 107–117. [Google Scholar] [CrossRef]
- Fagelson, M. Tinnitus and Traumatic Memory. Brain Sci. 2022, 12, 1585. [Google Scholar] [CrossRef]
- Moring, J.C.; Peterson, A.L.; Kanzler, K.E. Tinnitus, Traumatic Brain Injury, and Posttraumatic Stress Disorder in the Military. Int. J. Behav. Med. 2018, 25, 312–321. [Google Scholar] [CrossRef]
- Phillips, J.S.; Erskine, S.; Moore, T.; Nunney, I.; Wright, C. Eye Movement Desensitization and Reprocessing as a Treatment for Tinnitus. Laryngoscope 2019, 129, 2384–2390. [Google Scholar] [CrossRef]
- Luyten, T.; van Rompaey, V.; van de Heyning, P.; van Looveren, N.; Jacquemin, L.; Cardon, E.; Declau, F.; Fransen, E.; de Bodt, M.; Gilles, A. EMDR in the Treatment of Chronic Subjective Tinnitus: A Systematic Review. J. EMDR Pract. Res. 2020, 14, 135–149. [Google Scholar] [CrossRef]
- Coubard, O.A. An Integrative Model for the Neural Mechanism of Eye Movement Desensitization and Reprocessing (EMDR). Front. Behav. Neurosci. 2016, 10, 52. [Google Scholar] [CrossRef] [Green Version]
- Landin-Romero, R.; Moreno-Alcazar, A.; Pagani, M.; Amann, B.L. How Does Eye Movement Desensitization and Reprocessing Therapy Work? A Systematic Review on Suggested Mechanisms of Action. Front. Psychol. 2018, 9, 1395. [Google Scholar] [CrossRef]
- Vanderheyden, W.M.; Poe, G.R.; Liberzon, I. Trauma Exposure and Sleep: Using a Rodent Model to Understand Sleep Function in PTSD. Exp. Brain Res. 2014, 232, 1575–1584. [Google Scholar] [CrossRef]
- Poe, G.R. Sleep Is for Forgetting. J. Neurosci. 2017, 37, 464–473. [Google Scholar] [CrossRef] [Green Version]
- Scott, T.D. The Effects of Continuous, High Intensity, White Noise on the Human Sleep Cycle. Psychophysiology 1972, 9, 227–232. [Google Scholar] [CrossRef]
- Messineo, L.; Taranto-Montemurro, L.; Sands, S.A.; Oliveira Marques, M.D.; Azabarzin, A.; Wellman, D.A. Broadband Sound Administration Improves Sleep Onset Latency in Healthy Subjects in a Model of Transient Insomnia. Front. Neurol. 2017, 8, 718. [Google Scholar] [CrossRef] [Green Version]
- Griefahn, B. Sleep Disturbances Related to Environmental Noise. Noise Health 2002, 4, 57–60. [Google Scholar]
- Endo, S.; Kobayashi, T.; Yamamoto, T.; Fukuda, H.; Sasaki, M.; Ohta, T. Persistence of the Circadian Rhythm of REM Sleep: A Variety of Experimental Manipulations of the Sleep-Wake Cycle. Sleep 1981, 4, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Carr, M.; Nielsen, T. Morning REM Sleep Naps Facilitate Broad Access to Emotional Semantic Networks. Sleep 2015, 38, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.A. Sleep Patterns During Afternoon Naps in the Young and Elderly. Br. J. Psychiatry 1969, 115, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Pessah, M.A.; Roffwarg, H.P. Spontaneous Middle Ear Muscle Activity in Man: A Rapid Eye Movement Sleep Phenomenon. Sci. New Ser. 1972, 178, 773–776. [Google Scholar] [CrossRef]
- Benson, K.; Zarcone, V.P. Phasic Events of REM Sleep: Phenomenology of Middle Ear Muscle Activity and Periorbital Integrated Potentials in the Same Normal Population. Sleep 1979, 2, 199–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slegel, D.E.; Benson, K.L.; Zarcone, V.P.; Schubert, E.D. Middle-Ear Muscle Activity (MEMA) and Its Association with Motor Activity in the Extremities and Head in Sleep. Sleep 1991, 14, 454–459. [Google Scholar]
- Slegel, D.E.; Benson, K.L.; Zarcone, V.P. An Inexpensive Alternative for Recording Middle Ear Muscle Activity (MEMA) During Sleep. Sleep 1992, 15, 567–570. [Google Scholar] [CrossRef] [Green Version]
| SIT Group (n = 15) | Non-SIT Group (n =15) | p-Value | Effect Size | |
|---|---|---|---|---|
| Mean (Std) | Mean (Std) | |||
| Gender ratio (W = 1; M = 0) | 0.33 (0.47) | 0.4 (0.49) | 0.73 | |
| Age (years) | 50.67 (10.83) | 48.67 (13.26) | 0.71 | |
| THI score (0 - 100) | 54.4 (18.59) | 47.87 (25.61) | 0.38 | |
| VAS score on tinnitus intensity (0, 10) | 6.29 (1.67) | 6.6 (1.54) | 0.47 | |
| VAS score on tinnitus annoyance (0, 10) | 7.5 (1.64) | 6.47 (2.31) | 0.33 | |
| Tinnitus pitch (High: 0, Medium: 0.5, Low: 1) | 0.13 (0.34) | 0.16 (0.35) | 0.7 | |
| Tinnitus lateralisation (Bilateral: 0, Partly lateral: 0.5, Unilateral: 1) | 0.43 (0.32) | 0.3 (0.4) | 0.27 | |
| Hearing loss grade (No: 0, Mild: 1, Medium: 2; Severe: 3) | 0.73 (0.68) | 0.87 (0.96) | 0.95 | |
| Have used or are using hearing aids (Yes: 1, No: 0) | 0.47 (0.5) | 0.53 (0.5) | 0.74 | |
| Tinnitus increases after naps (Strongly: 1, Mildly: 0.5, No: 0) | 0.87 (0.29) | 0.07 (0.17) | <0.01 ** | 3.499 |
| Masked by noisy environment ? (Yes: 1, No: 0) | 0.47 (0.5) | 0.47 (0.5) | 1.0 | |
| Masked by white noise ? (Yes: 1, No: 0) | 0.47 (0.5) | 0.8 (0.4) | 0.07 | −0.712 |
| Tinnitus raises with long noise exposure (Yes: 1, No: 0) | 0.23 (0.36) | 0.37 (0.43) | 0.41 | |
| Tinnitus raises with loud noise (Yes: 1, No: 0) | 0.1 (0.2) | 0.43 (0.44) | 0.03 * | −0.938 |
| Are daily noises inconfortable ? (Yes: 1, No: 0) | 0.53 (0.5) | 0.6 (0.49) | 0.74 | |
| Is powerful noise exposure painful ? (Yes: 1, No: 0) | 0.47 (0.5) | 0.6 (0.49) | 0.49 | |
| Jaw stiffness in the morning (Frequency gradation) | 0.47 (0.81) | 0.53 (0.88) | 0.94 | |
| Jaw clenching during the day (Frequency gradation) | 1.0 (1.32) | 0.4 (0.8) | 0.2 | 0.532 |
| Facial pain or jaw pain (Frequency gradation) | 0.73 (1.0) | 0.4 (0.8) | 0.29 | |
| Facial or jaw muscle fatigue (Frequency gradation) | 0.6 (0.88) | 0.13 (0.5) | 0.08 | 0.631 |
| Jaw popping (Frequency gradation) | 0.67 (1.14) | 0.67 (1.01) | 0.88 | |
| Headaches/migraine (Frequency gradation) | 0.6 (0.95) | 1.0 (1.15) | 0.37 | |
| Neck pain (Frequency gradation) | 1.47 (1.54) | 1.6 (1.08) | 0.79 | |
| Neck stiffness/hypomobility (Frequency gradation) | 0.27 (0.77) | 1.27 (1.24) | <0.01 ** | −0.937 |
| Ear fullness (Frequency gradation) | 1.07 (1.06) | 0.87 (1.2) | 0.62 | |
| Autophony (Frequency gradation) | 0.13 (0.5) | 0.4 (0.8) | 0.31 | |
| Otalgia (Frequency gradation) | 0.6 (1.14) | 0.73 (1.34) | 0.94 | |
| Sleep duration (<6 h: −1, 6–8 h: 0, >8 h: 1) | 0.07 (0.57) | −0.07 (0.57) | 0.55 | |
| Self reported insomnia (Yes: 1, No: 0) | 0.4 (0.49) | 0.13 (0.34) | 0.11 | 0.611 |
| Hard to stay asleep (Yes: 1, No: 0) | 0.6 (0.49) | 0.6 (0.49) | 1.0 | |
| Hard to fall asleep (Yes: 1, No: 0) | 0.27 (0.44) | 0.47 (0.5) | 0.27 | |
| Snoring (Yes: 1, No: 0) | 0.73 (0.44) | 0.4 (0.49) | 0.07 | 0.69 |
| SIT Group (n = 15) | Non-SIT Group (n = 14) | p-Value | Effect Size | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (Std) | Mean (Std) | |||||||
| Total sleep time (TST, in min) | 385.63 (46.37) | 408.35 (61.11) | 0.23 | |||||
| Wake time after sleep onset (WASO, in min) | 59.31 (35.32) | 68.79 (38.72) | 0.6 | |||||
| Sleep latency (min) | 16.13 (18.71) | 18.45 (16.83) | 0.33 | |||||
| REM sleep latency (min) | 120.87 (44.89) | 118.68 (54.67) | 0.66 | |||||
| Total Bruxism (number of episodes per hour) | 13.05 (4.14) | 15.85 (5.29) | 0.14 | −0.571 | ||||
| Phasic Bruxism (number of episodes per hour) | 1.72 (0.69) | 1.88 (0.85) | 0.61 | |||||
| Tonic Bruxism (number of episodes per hour) | 3.02 (1.81) | 4.53 (2.17) | 0.06 | −0.733 | ||||
| Mixed Bruxism (number of episodes per hour) | 0.77 (0.44) | 0.93 (0.39) | 0.31 | |||||
| Apnea Hypopnea Index (AHI) (*) | 14.19 (10.58) | 14.0 (10.1) | 0.91 | |||||
| Oxygen Desaturation Index (ODI) | 12.77 (10.16) | 13.37 (8.71) | 0.79 | |||||
| % TST | Duration (min) | % TST | Duration (min) | For % TST | Duration (min) | For % TST | Duration (min) | |
| N1 sleep (%, min) | 7.2 (2.79) | 27.55 (9.71) | 5.68 (2.74) | 22.05 (7.85) | 0.13 | 0.1 | 0.53 | 0.6 |
| N2 sleep (%, min) | 53.87 (10.79) | 209.04 (53.31) | 44.74 (6.5) | 184.34 (44.87) | 0.01 * | 0.2 | 0.98 | |
| N3 sleep (%, min) | 22.93 (10.97) | 86.45 (35.18) | 28.52 (5.88) | 114.89 (22.8) | <0.01 ** | <0.01 ** | −0.61 | −0.92 |
| REM sleep (%, min) | 15.93 (5.84) | 62.13 (25.46) | 21.08 (4.66) | 87.18 (26.5) | 0.04 * | 0.04 * | −0.94 | −0.93 |
| Snoring (%, min) | 20.23 (15.45) | 74.75 (54.26) | 19.08 (19.19) | 72.46 (72.29) | 0.66 | 0.65 | ||
| Supine position (%, min) | 45.33 (33.81) | 185.18 (149.91) | 30.86 (24.89) | 127.4 (105.41) | 0.25 | 0.37 | ||
| Lateral position (%, min) | 48.47 (31.79) | 178.9 (114.28) | 56.29 (27.42) | 223.7 (108.22) | 0.53 | 0.31 | ||
| Prone position (%, min) | 4.46 (8.82) | 18.61 (36.32) | 10.43 (18.07) | 45.95 (81.85) | 0.16 | 0.15 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillard, R.; Korczowski, L.; Léger, D.; Congedo, M.; Londero, A. REM Sleep Impairment May Underlie Sleep-Driven Modulations of Tinnitus in Sleep Intermittent Tinnitus Subjects: A Controlled Study. Int. J. Environ. Res. Public Health 2023, 20, 5509. https://doi.org/10.3390/ijerph20085509
Guillard R, Korczowski L, Léger D, Congedo M, Londero A. REM Sleep Impairment May Underlie Sleep-Driven Modulations of Tinnitus in Sleep Intermittent Tinnitus Subjects: A Controlled Study. International Journal of Environmental Research and Public Health. 2023; 20(8):5509. https://doi.org/10.3390/ijerph20085509
Chicago/Turabian StyleGuillard, Robin, Louis Korczowski, Damien Léger, Marco Congedo, and Alain Londero. 2023. "REM Sleep Impairment May Underlie Sleep-Driven Modulations of Tinnitus in Sleep Intermittent Tinnitus Subjects: A Controlled Study" International Journal of Environmental Research and Public Health 20, no. 8: 5509. https://doi.org/10.3390/ijerph20085509