
Bullying against Healthcare Professionals and Coping Strategies: A Scoping Review



Abstract
1. Introduction
- What are the main bullying behaviours identified by healthcare professionals and what are their consequences?
- What coping strategies are used by healthcare professionals who are victims of bullying?
2. Methodology
2.1. Research Procedures
2.2. Inclusion and Exclusion Criteria
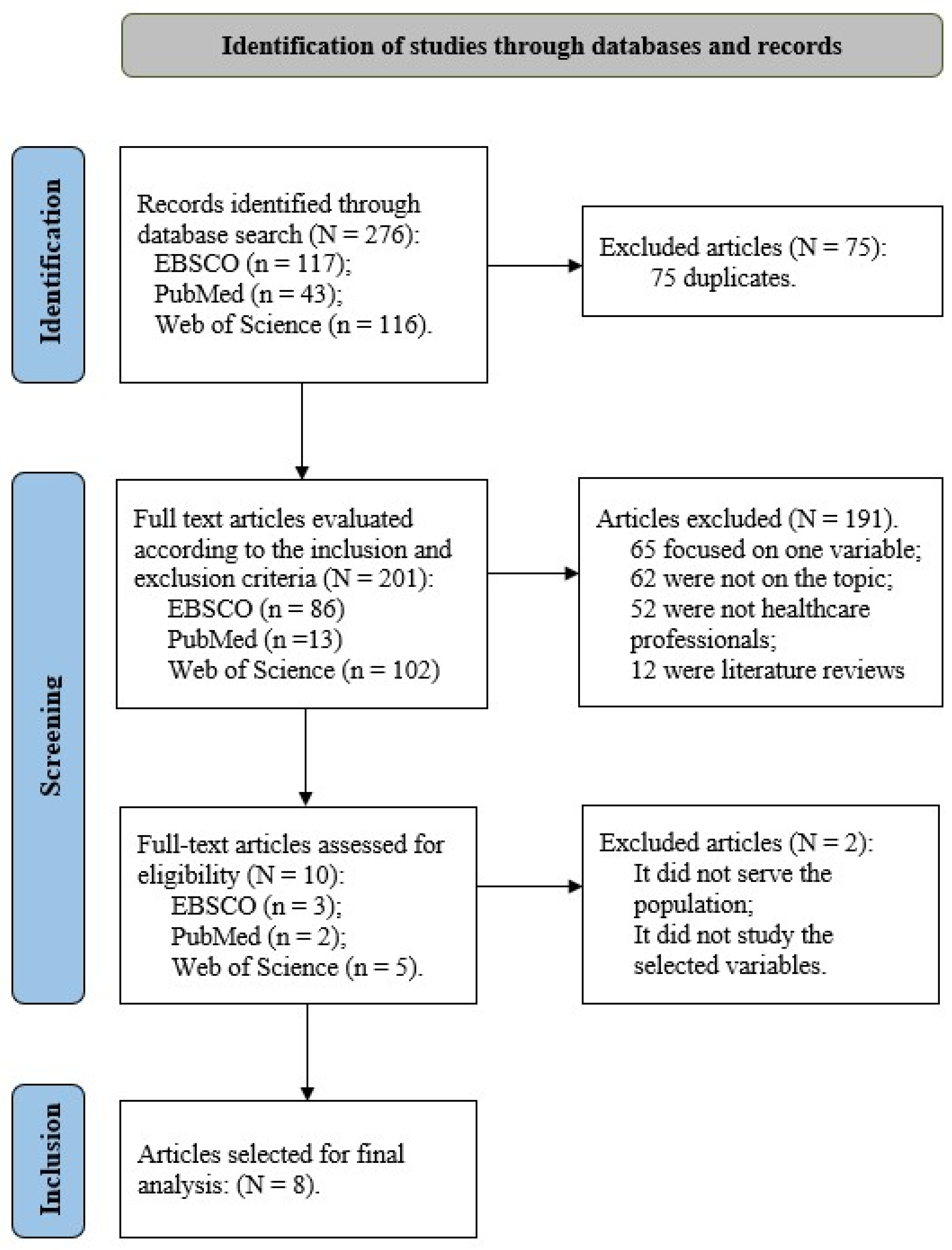
2.3. Article Selection
2.4. Article Quality Analysis
3. Results
3.1. Multiple Approaches to Workplace Bullying Research
3.2. Methodological Aspects of International Research on Workplace Bullying
3.3. Bullying Behaviours, Consequences, and Coping Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carvalho, M.; Matos, M.G. Bullying. In Dicionário Crime, Justiça e Sociedade; Maia, R., Nunes, L., Caridade, S., Sani, A., Estrada, R., Nogueira, C., Fernandes, H., Afonso, L., Eds.; Edições Sílabo: Lisbon, Portugal, 2016; pp. 67–69. [Google Scholar]
- Munro, C.E.; Phillips, A.W. Bullying in the workplace. Surgery 2023, 10, 653–658. [Google Scholar]
- Brodsky, C.M. The Harassed Worker; Lexington Books: Toronto, ON, Canada, 1976. [Google Scholar]
- Leymann, H. Mobbing and Psychological Terror at Workplaces. Violence Vict. 1990, 5, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Leymann, H. The content and development of mobbing at work. Eur. J. Work. Organ. Psychol. 1996, 5, 165–184. [Google Scholar] [CrossRef]
- Hirigoyen, M. Assédio, Coacção e Violência no Quotidiano; Pergaminho: Lisbon, Portugal, 1999. [Google Scholar]
- American Nurses Association. American Nurses Association Position Statement on Incivility, Bullying, and Workplace Violence. 2015. Available online: http://nursingworld.org/DocumentVault/Position-Statements/Practice/Position-Statement-on-Incivility-Bullying-and-Workplace-Violence.pdf (accessed on 20 March 2024).
- Layne, D.M.; Nemeth, L.S.; Mueller, M. Negative Behavior Among Healthcare Professionals: Integrative Review of Instruments. J. Nurs. Meas. 2020, 28, E30–E65. [Google Scholar] [CrossRef] [PubMed]
- Einarsen, S.; Hoel, H.; Zapf, D.; Cooper, C.L. The concept of bullying and harassment at work: The European tradition. In Bullying and Harassment in the Workplace: Developments in Theory, Research, and Practice; Einarsen, S., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2011; pp. 3–39. [Google Scholar]
- Lee, H.; Ryu, Y.M.; Yu, M.; Kim, H.; Oh, S. A Qualitative Meta-Synthesis of Studies on Workplace Bullying among Nurses. Int. J. Environ. Res. Public Health 2022, 19, 14120. [Google Scholar] [CrossRef] [PubMed]
- Barros, C.; Meneses, R.F.; Sani, A.; Baylina, P. Workplace Violence in Healthcare Settings: Work-Related Predictors of Violence Behaviours. Psych 2022, 4, 516–524. [Google Scholar] [CrossRef]
- Pompeii, L.A.; Schoenfisch, A.L.; Lipscomb, H.J.; Dement, J.M.; Smith, C.D.; Upadhyaya, M. Physical assault, physical threat, and verbal abuse perpetrated against hospital workers by patients or visitors in six U.S. hospitals. Am. J. Ind. Med. 2015, 58, 1194–1204. [Google Scholar] [CrossRef]
- Rahm, G.; Rystedt, I.; Wilde-Larsson, B.; Nordström, G.; Strandmark, K.M. Workplace bullying among healthcare professionals in Sweden: A descriptive study. Scand. J. Caring Sci. 2019, 33, 582–591. [Google Scholar] [CrossRef]
- Sun, P.; Zhang, X.; Sun, Y.; Ma, H.; Jiao, M.; Xing, K.; Kang, Z.; Ning, N.; Fu, Y.; Wu, Q.; et al. Workplace Violence against Health Care Workers in North Chinese Hospitals: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2017, 14, 96. [Google Scholar] [CrossRef]
- Antão, H.S.; Sacadura-Leite, E.; Manzano, M.J.; Pinote, S.; Relvas, R.; Serranheira, F.; Sousa-Uva, A. Workplace Violence in Healthcare: A Single-Center Study on Causes, Consequences and Prevention Strategies. Acta Médica Port. 2020, 33, 31–37. [Google Scholar] [CrossRef]
- Goh, H.S.; Hosier, S.; Zhang, H. Prevalence, Antecedents, and Consequences of Workplace Bullying among Nurses—A Summary of Reviews. Int. J. Environ. Res. Public Health 2022, 19, 8256. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.; Costa, V.; Teixeira, J.; Azevedo, A.; Roma-Torres, A.; Amaro, J.; Cunha, L. Prevalence and Determinants of Bullying Among Health Care Workers in Portugal. Work Health Saf. 2017, 65, 188–196. [Google Scholar] [CrossRef]
- Torres, A.; Costa, D.; Sant’Ana, H.; Coelho, B.; Sousa, I. Assédio Sexual e Moral no Local de Trabalho; CITE: Lisbon, Portugal, 2016. [Google Scholar]
- Yosep, I.; Mardhiyah, A.; Hendrawati, H.; Hendrawati, S. Interventions for Reducing Negative Impacts of Workplace Violence Among Health Workers: A Scoping Review. J. Multidiscip. Health 2023, 16, 1409–1421. [Google Scholar] [CrossRef] [PubMed]
- Purpora, C.; Cooper, A.; Sharifi, C. The prevalence of nurses’ perceived exposure to workplace bullying and its effect on nurse, patient, organization and nursing-related outcomes in clinical settings: A quantitative systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 51–62. [Google Scholar] [CrossRef]
- Rai, A.; Agarwal, U.A. A review of literature on mediators and moderators of workplace bullying: Agenda for future research. Manag. Res. Rev. 2018, 41, 822–859. [Google Scholar] [CrossRef]
- Lazarus, R.; Folkman, S. Stress, Appraisal and Coping; Springer: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Folkman, S.; Lazarus, R.S. If it changes it must be a process: Study of emotion and coping during three stages of a college examination. J. Pers. Soc. Psychol. 1985, 48, 150–170. [Google Scholar] [CrossRef]
- Rodriguez, S.Y.S.; Otto, M.S.; Barcinski, M. Estratégias de enfrentamento utilizadas por psicólogos: Uma análise de gênero [Coping strategies used by psychologists: A gender analysis]. Salud Soc. 2015, 6, 110–119. [Google Scholar] [CrossRef]
- Santos, N.A.R.; Gomes, V.S.; Rodrigues, C.M.A.; Santos, J.; Passos, J.P. Estratégias de enfrentamento utilizadas pelos enfermeiros em cuidados paliativos oncológicos: Revisão integrativa. Cogitare Enferm. 2016, 21, 1–8. [Google Scholar]
- Acquadro Maran, D.; Giacomini, G.; Scacchi, A.; Bigarella, R.; Magnavita, N.; Gianino, M.M. Consequences and coping strategies of nurses and registered nurses perceiving to work in an environment characterized by workplace bullying. Dialogues Health 2024, 4, 100174. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. An Analysis of Coping in a Middle-Aged Community Sample. J. Health Soc. Behav. 1980, 21, 219–239. [Google Scholar] [CrossRef]
- Angst, R. Psicologia e resiliência: Uma revisão de literatura. Psicol. Argum. 2009, 27, 253–260. [Google Scholar] [CrossRef]
- General Directorate of Health. Relatório de Avaliação dos Episódios de Violência Contra os Profissionais de Saúde. Departamento da Qualidade na Saúde. 2011. Available online: https://app.parlamento.pt/webutils/docs (accessed on 20 March 2024).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Mak, S.; Thomas, A. Steps for Conducting a Scoping Review. J. Grad. Med Educ. 2022, 14, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Berry, P.; Gillespie, G.; Fisher, B.; Gormley, D.; Haynes, J. Psychological Distress and Workplace Bullying Among Registered Nurses. Online J. Issues Nurs. 2022, 21, 8. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.; Jeong, S.; Smith, T. Negative workplace behavior and coping strategies among nurses: A cross-sectional study. Nurs. Health Sci. 2020, 23, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Kim, H.; Choi, E.K.; Park, C.G. Workplace bullying and different levels of post-traumatic stress symptoms of nurses: A quantile regression approach for effective coping strategies. J. Nurs. Manag. 2021, 30, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Mills, C.B.; Keller, M.; Chilcutt, A.; Nelson, M.D. No Laughing Matter: Workplace Bullying, Humor Orientation, and Leadership Styles. Work Health Saf. 2018, 67, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Luo, H.; Ma, Q.; Zhong, Y.; Yang, X.; Huang, Y.; Sun, X.; Wang, X.; He, J.; Song, Y. Association between workplace bullying and nurses’ professional quality of life: The mediating role of resilience. J. Nurs. Manag. 2021, 30, 1549–1558. [Google Scholar] [CrossRef]
- Reknes, I.; Einarsen, S.; Pallesen, S.; Bjorvatn, B.; Moen, B.E.; Magerøy, N. Exposure to bullying behaviors at work and subsequent symptoms of anxiety: The moderating role of individual coping style. Ind. Health 2016, 54, 421–432. [Google Scholar] [CrossRef]
- Tabakakis, C.K.; McAllister, M.; Bradshaw, J.; To, Q.G. Psychological resilience in New Zealand registered nurses: The role of workplace characteristics. J. Nurs. Manag. 2019, 27, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Ahn, H.Y. Nurses’ Workplace Bullying Experiences, Responses, and Ways of Coping. Int. J. Environ. Res. Public Health 2020, 17, 7052. [Google Scholar] [CrossRef] [PubMed]
- Einarsen, S.; Hoel, H.; Notelaers, G. Measuring exposure to bullying and harassment at work: Validity, factor structure and psychometric properties of the Negative Acts Questionnaire-Revised. Work Stress 2009, 23, 24–44. [Google Scholar] [CrossRef]
- Lee, Y.; Lee, M. Development and Validity of Workplace Bullying in Nursing-Type Inventory (WPBN-TI). J. Korean Acad. Nurs. 2014, 44, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y. Development of Workplace Bullying in Nursing-Consequence Inventory (WPBN-CI). J. Korean Acad. Ind. Coop. Soc. 2016, 17, 479–488. [Google Scholar] [CrossRef]
- Han, J.S.; Oh, K.S. A study on the grief and coping pattern of mothers who have a chronically ill child. Korean Nurse 1990, 29, 73–87. [Google Scholar] [CrossRef]
- Thorson, J.A.; Powell, F.C. Development and validation of a multidimensional sense of humor scale. J. Clin. Psychol. 1993, 49, 13–23. [Google Scholar] [CrossRef]
- Muenjohn, N.; Armstrong, A. Evaluating the structural validity of the Multifactor Leadership Questionnaire (MLQ), capturing the leadership factors of transformational-transactional leadership. Contemp. Manag. Res. 2008, 4, 704. [Google Scholar] [CrossRef]
- Lim, H.-K.; Woo, J.-M.; Kim, T.-S.; Kim, T.-H.; Choi, K.-S.; Chung, S.-K.; Chee, I.S.; Lee, K.-U.; Paik, K.C.; Seo, H.-J.; et al. Reliability and validity of the Korean version of the Impact of Event Scale-Revised. Compr. Psychiatry 2009, 50, 385–390. [Google Scholar] [CrossRef]
- Park, A.S.; Lee, Y.H. Influence of the sex role characteristics and stress perception of married women on the coping style for stress. Korean J. Couns. Psychother. 1992, 4, 69–79. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, H.R.; Olff, M.; Ursin, H. The CODE: A revised battery for coping and defense and its relations to subjective health. Scand. J. Psychol. 1997, 38, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Yu, H.; Zhang, Y.; Jiang, A. Professional quality of life: A cross-sectional survey among Chinese clinical nurses. Nurs. Health Sci. 2015, 17, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.; Notelaers, G.; Einarsen, S. Measuring exposure to workplace bullying. In Bullying and Harassment in the Workplace: Developments in Theory, Research, and Practice; Einarsen, S., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2011; pp. 149–174. [Google Scholar]
- Lake, E.T. Development of the practice environment scale of the Nursing Work Index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Edwards, C.D.; Montuori, J.L.R. State-Trait Anxiety Inventory for Children; Consulting Psychologist Press: Palo Alto, CA, USA, 1976. [Google Scholar]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behaviour Research and Therapy 1996, 34, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Hampton, D.; Rayens, M.K. Impact of Psychological Empowerment on Workplace Bullying and Intent to Leave. J. Nurs. Adm. 2019, 49, 179–185. [Google Scholar] [CrossRef]
- Asi Karakaş, S.; Okanli, A. The Effect of Assertiveness Training on the Mobbing That Nurses Experience. Work. Health Saf. 2015, 63, 446–451. [Google Scholar] [CrossRef]
- Botha, E.; Gwin, T.; Purpora, C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: A systematic review of quantitative evidence protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 21–29. [Google Scholar] [CrossRef]
- Glass, N.; Hanson, G.C.; Anger, W.K.; Laharnar, N.; Campbell, J.C.; Weinstein, M.; Perrin, N. Computer-based training (CBT) intervention reduces workplace violence and harassment for homecare workers. Am. J. Ind. Med. 2017, 60, 635–643. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Articles/Topics | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Berry et al. [33] | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 19 Average |
| Hawkins et al. [34] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 25 High |
| Hong et al. [35] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 26 High |
| Mills et al. [36] | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 22 High |
| Peng et al. [37] | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 24 High |
| Reknes et al. [38] | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 23 High |
| Tabakakis et al. [39] | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 1 | 22 High |
| Yoo & Ahn [40] | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 20 Average |
| Authors (Year) | Goals | Local/ Participants | Instruments | Design | Main Results [Bullying, Symptoms, and Coping Strategies] |
|---|---|---|---|---|---|
| Berry et al. [33] | Determine differences in the perception of stress, state anxiety, and post-traumatic stress symptoms based on levels of exposure to bullying, as well as determine the strategies used | USA 1st phase = 84 nurses 2nd phase = 11 nurses | Negative Acts Questionnaire; 10-Item Perceived Stress Scale; 20-Item Subscale of the State Trait Anxiety Inventory; Post-traumatic Stress Disorder Checklist Civilian Version; Individual Questionnaire | Quantitative and qualitative study | The study identified significant differences in the perception of stress, anxiety, and post-traumatic symptoms that have been reported by people with frequent or daily exposure to workplace bullying behaviour. |
| Hawkins et al. [34] | Understand the type and frequency of negative behaviours in the workplace and the strategies used when exposed to these behaviours | Australia 74 nurses | Negative Acts Questionnaire—Revised; Purpose-designed questions; Ways of Coping questionnaire | Quantitative study | The most common type of negative workplace behaviour reported was “work-related bullying”, and they reported using a variety of coping strategies, including problem-focused strategies and seeking social support. |
| Hong et al. [35] | Investigate the effects of workplace bullying and different symptoms of post-traumatic stress and coping among hospital nurses | Korea 233 nurses | Workplace Bullying in Nursing—Type Inventory; Impact of Event Scale—Revised; Ways of Coping Checklist | Quantitative study | The study explores bullying in the workplace of nurses, detecting high-risk subgroups, and suggesting the development of coping interventions to reduce workplace bullying and symptoms of post-traumatic stress. |
| Mills et al. [36] | Determine whether nurses’ humour orientation styles and leadership styles can influence perceptions of workplace bullying | USA 459 participants | Multidimensional Sense of Humour Scale; Bass’s Multifactor Leadership Questionnaire; Negative Acts Questionnaire—Revised | Quantitative study | One of the four humour subscales, Humour Appreciation, affected perceptions of workplace bullying. The other three, Humour Recognition, Humour Production and Humour for Coping, had no effect. However, managers’ leadership styles affected reports of negative acts. |
| Peng et al. [37] | Determine the relationship between workplace bullying and nurses’ quality of life and also the mediating role of resilience between workplace bullying and quality of life | China 493 nurses | Negative Acts Questionnaire—Revised; 10-item Connor–Davidson Resilience; the Chinese Version of Professional Quality-of-Life Scale | Quantitative study | Bullying in the workplace had negative and direct effects on nurses’ quality of professional life. Resilience mediated the relationship between workplace bullying and quality of professional life. |
| Reknes et al. [38] | To investigate whether bullied nurses have a more negative coping style when faced with stressful events than nurses who are not bullied and to determine whether coping style moderates the relationship between bullying and anxiety | Norway 1st phase = 2059 participants 2nd phase = 1582 participants | Negative Acts Questionnaire—Revised; Hospital Anxiety and Depression Scale; Utrecht Coping List | Quantitative study | Bullied nurses use a goal-oriented active coping style less frequently than non-bullied nurses. Furthermore, active goal-oriented coping appears to be beneficial only when exposure to bullying behaviours is very low. Victims of bullying appear to deal more negatively with stressful events than others. |
| Tabakakis et al. [39] | Investigate the impact of workplace factors on nurses’ psychological resilience, including bullying | Australia 480 nurses | The Connor–Davidson Resilience 10 scale; The Practice Environment Scale of the Nursing Work Index; Negative Acts Questionnaire—Revised | Quantitative study | The work environment and perception of exposure to workplace bullying play a significant role in shaping nurses’ psychological resilience. |
| Yoo & Ahn [40] | Analyse the relationship between workplace bullying experiences, responses, and coping strategies | Korea 113 nurses | Workplace Bullying in Nursing-Type Inventory; Workplace Bullying in Nursing—Consequence Inventory; Way of Coping | Quantitative study | Nurses complained of helplessness, depression, stress, insomnia, and physical discomfort, and complained that they made more mistakes in their work and wanted to change jobs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, A.R.V.; Sani, A.I. Bullying against Healthcare Professionals and Coping Strategies: A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 459. https://doi.org/10.3390/ijerph21040459
Ribeiro ARV, Sani AI. Bullying against Healthcare Professionals and Coping Strategies: A Scoping Review. International Journal of Environmental Research and Public Health. 2024; 21(4):459. https://doi.org/10.3390/ijerph21040459
Chicago/Turabian StyleRibeiro, Ana Rita Valente, and Ana Isabel Sani. 2024. "Bullying against Healthcare Professionals and Coping Strategies: A Scoping Review" International Journal of Environmental Research and Public Health 21, no. 4: 459. https://doi.org/10.3390/ijerph21040459
APA StyleRibeiro, A. R. V., & Sani, A. I. (2024). Bullying against Healthcare Professionals and Coping Strategies: A Scoping Review. International Journal of Environmental Research and Public Health, 21(4), 459. https://doi.org/10.3390/ijerph21040459