1. Introduction
Worldwide, there are differences in the prevalence of preschool wheezing, and it appears to be rising [
1]. Wheeze can be described as a persistent high-pitched sound characterized by a melodic tone that originates from the chest during the act of exhaling [
1,
2]. Wheezing throughout early childhood is a prevalent yet intricate symptom characterized by multiple aetiologies and potential consequences [
2]. Moreover, wheezing in preschoolers results in significant healthcare costs and unscheduled hospital consultations [
3].
It is common for children who exhibit wheezing symptoms before the age of three, and persist with wheezing until the age of six, to possess atopic tendencies and subsequently develop asthma over the years [
4,
5]. Moreover, it has been observed that the respiratory capacity of children experiencing wheezing tends to enhance as they grow older; however, their respiratory capacity never reaches the level observed in children who have never experienced wheezing [
4].
Preschool wheezing is a common condition, and environmental tobacco smoke (ETS) exposure is a significant risk factor for wheezing in preschool children [
6,
7,
8]. ETS possess comparable toxic components to those found in conventional tobacco smoke, consequently resulting in similar detrimental consequences akin to those observed in individuals who engage in active smoking [
9]. The symptoms of wheezing may exhibit temporary remission following therapy interventions and/or the avoidance of triggers associated with the condition. Hence, it is advisable to enact legislation aimed at the elimination and regulation of children’s exposure to ETS.
According to the Tobacco Products Control Act of 1993 in South Africa, specifically Section 2(1)(a)(iii), it is prohibited for individuals to engage in smoking any tobacco product within a motor vehicle in the presence of a child under the age of 12 years. This provision has been subject to amendments. The act of smoking is now prohibited within buildings designated for commercial childcare services. Sweets and toys resembling cigarettes are likewise prohibited. The implementation of new tobacco regulations was officially announced in September 2022 through the publication of Government Gazette Staats koerant [
10].
The following are highlights that will be considered regarding the risk of childhood exposure to ETS:
In the event that a residence is utilized for educational purposes, tutoring services, or commercial childcare, the act of smoking is prohibited.
There is implementation of a prohibition on smoking within motor vehicles in the presence of a minor under the age of 18, provided that there is more than one individual occupying said vehicle.
The proposed legislative expansion involves not only traditional cigarettes, but also embraces any devices used in connection with tobacco-related goods and electronic delivery systems, such as pipes, water pipes, and electronic devices.
There is a tendency for wheezing prevalence to be lower in rural areas, with some evidence suggesting the presence of an urban–rural gradient [
11,
12]. The urban–rural gradient of wheeze in preschool children is examined in this study to determine whether this indicator differs along an urban–rural gradient.
The current tobacco control laws are introduced as a baseline and the impact of the regulations will be seen in later years. This study presents the baseline of the prevalence of wheezing in Mpumalanga where children are exposed to polluted air including ETS. The aim was to assess the prevalence of wheezing and its association with environmental tobacco smoke exposure among rural and urban preschool children in Mpumalanga province, South Africa.
2. Methods
2.1. Study Design and Settings
An analytical cross-sectional survey was conducted between November 2020 and April 2021. The objective of our study was to assess the prevalence of wheezing and its association with environmental tobacco smoke exposure, a common symptom of asthma, among preschool children residing in rural and urban areas. The research was carried out within the Mpumalanga province, specifically in the Gert Sibande district municipality, which is situated within the Highveld Priority Area. In accordance with the National Environmental Management: Air Quality Act, 2004 (Act No. 39 of 2004), the Minister of Environmental Affairs named this region a priority area for air pollution in 2007.
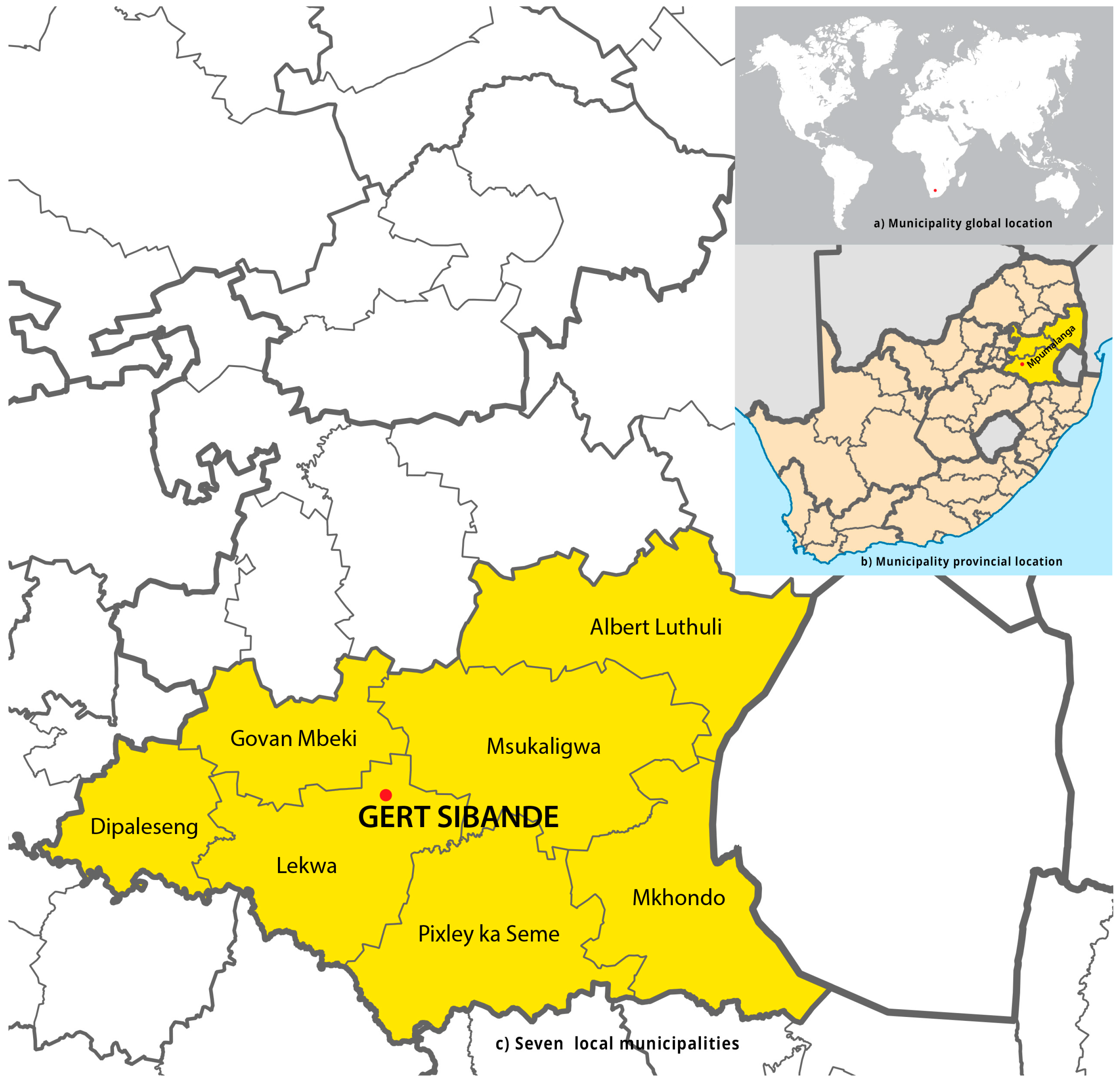
The Gert Sibande district municipality was purposively selected because it is in the Highveld priority area. The Highveld priority area has substandard air quality and heightened levels of pollutants originating from both industrial and non-industrial origins. The district encompasses a diverse range of sectors, such as power generating, petrochemical, primary metallurgy, and open-cast mining. The district municipality comprises seven local municipalities, specifically Dipaleseng, Govan Mbeki, Lekwa, Msukukaligwa, and DR Pixley ka Seme, all of which are situated within the Highveld priority area. The Chief Albert Luthuli and Mkhondo municipalities are not encompassed under the Highveld priority area.
Figure 1 illustrates the geographical distribution of seven local district municipalities, with Gert Sibande being visually distinguished by the use of light-yellow highlighting.
2.2. Study Population, Sample Size Estimation, and Sampling Procedure
The participants in this study consisted of preschool-aged children, ranging from one to eight years old, who resided in and attended preschools located in either rural or urban areas within the Mpumalanga province, specifically in the Gert Sibande district municipality. Based on the data from the 2019 Gert Sibande database, the number of children enrolled in preschool was recorded as 13,485 (see
Table S1, Supplementary Materials) [
13]. The overall sample size required for this study was determined to be 3900, assuming a response rate of 70%. A study power of 80% was used for the investigation, with a significance level of 5%. The sample size was determined using the sample size calculator in Microsoft Excel (see
Tables S2 and S3, Supplementary Materials).
A probability sample design was employed to achieve equitable representation of all preschool children throughout seven local municipalities (see
Tables S2 and S3, Supplementary Materials). Preschools were identified in the northern, southern, eastern, and western regions of each of the seven municipalities within the Gert Sibande district (
Figure 1). A representative sample of preschools was chosen from each of the four areas within each municipality. Preschool children were selected randomly from a class roster obtained from each designated preschool. Selected preschoolers were then given participant information leaflets inviting their parents to be part of the study. Parents, who consented to let their children participate, were then given an informed consent form and a questionnaire to complete (during parent meetings or when they pick up or drop off the children) and return to the preschool. All necessary COVID-19 protocols were implemented.
2.3. Study Tools
Data were collected using the modified International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire. The questionnaire was divided into two sections: namely demographic data and health outcomes. The questionnaire was in English, which is the common language in a region with multiple local languages. In order to evaluate the data collection procedure and the quality of the survey questions in light of COVID-19 limitations, a pre-test of the instrument was conducted with environmental health practitioners. These professionals were chosen owing to their regular interaction with parents and carers, which provides them with insights into the educational background of these individuals.
2.4. Health Outcomes of the Study
The following central questions about asthma symptoms were used in order to evaluate health outcomes: (1) Has your child ever experienced chest wheezing or whistling in the past? (Wheeze Ever) (2) Has he or she had chest wheezing or whistling in the previous 12 months? (Current Wheeze) (3) How many wheezing episodes did your child have in the last 12 months? (4) How frequently, on average, during the previous 12 months was your child’s sleep interrupted by wheezing? (5) Has your child’s wheezing ever been sufficiently severe to prevent them from speaking more than a few phrases at any time between breathing in the last 12 months? (6) Did the child ever suffer from asthma? (Asthma Ever) (7) Did a physician or nurse diagnose the asthma? (8) Has your child’s chest ever made a wheezy noise while playing or right after? (9) Besides from a cough brought on by a cold or chest illness, has your child experienced a cough that is dry at night in the last 12 months?
The classification of Current Severe Wheeze was determined if parents provided affirmative responses to every one of the subsequent questions, noting that (1) the children have severe wheezing, with a frequency of 4–12 bouts or over 12 episodes throughout the preceding 12-month period; (2) the children experience disrupted sleep as a result of wheezing at least once a week or more; (3) the children had experienced a wheezing episode within the last 12 months, resulting in a reduction in their ability to speak to just a few phrases at a time due to intermittent breaths; and (4) the children experienced wheezing symptoms during or following physical activity throughout the preceding 12-month period.
2.5. Environmental Tobacco Smoke Exposure
Parents and caregivers were requested to provide responses pertaining to risk factors associated with wheezing, a symptom commonly observed in individuals with asthma. The questions encompassed the following: Does the male parent engage in smoking behaviour? (yes/no). Is the female parent engaged in the act of smoking? (yes/no).
The present study examines the extent of children’s exposure to smoking inside their household during the past 30 days, categorized into several frequency levels: never, 1–6 days, 7–10 days, 16–20 days, and more than 20 days. The present study examines the prevalence of children’s exposure to smoking inside the school environment over a period of 30 days.
The duration of the observed time intervals ranges from never through 1–6 days, 7–10 days, 16–20 days, and more than 20 days. The present study examines the extent to which children have been exposed to smoking in cars or other modes of transportation within the preceding 30 days. The duration of the event might vary, ranging from less than a week to over three weeks. The present study examines the frequency of children being subjected to smoking within the past 30 days in a restaurant setting. Parents/caregivers were asked to indicate the number of days in which children were exposed to smoking, with response options ranging from never to more than 20 days. In addition, they were asked the following question: what is the number of individuals residing in the same household as your child that engages in smoking?
2.6. Confounders
Parents and caregivers were asked to answer a series of questions about the following topics: What is the gender of the child (male/female)? What is the location of the child (rural/urban)? How long has the child lived in the area (6 to 12 months/1 to 2 years/3 years or longer)? Was the child born in the area (hospital/clinic/home/does not apply)? What kind of residence does the child live in (brick/mud/corrugated iron/mixture/other)? In the last 12 months, has the child used analgesics/antibiotics (never/at least once a year/at least once per month)? What type of fuel is utilized for cooking and heating (electricity/gas/paraffin/coal/wood/other)? How does the child get to and from school (walks/taxi/bus/motor vehicle/combination/other)? How frequently do trucks, buses, and taxis pass through your neighbourhood (never/rarely/frequently throughout the day/almost the entire day)? Other questions focused on pet ownership, education for parents/caregivers, job occupation of parents/caregivers, and family health history.
2.7. Data Processing and Analysis
The data were captured using EpiData version 3.1 [
14], for the purpose of ensuring quality, and subsequently analysed using STATA 17. Descriptive statistics were computed, utilizing means and standard deviations for continuous data, and frequencies expressed as percentages for categorical data. Observations that were labelled as “not recorded” were designated as missing. Consequently, there were variations in the sample sizes utilized to address each respective question.
In this study, we assessed the association between demographic factors, including gender, age, location, and family history, with four outcome variables: Wheeze Ever, Current Wheeze, Current Severe Wheeze, and Asthma Ever. Statistical comparisons were conducted using the chi-square test for independent samples. The researchers employed multiple logistic regression to account for any confounding variables, assessing the strength of the relationship using the odds ratio (OR) and 95% confidence intervals (CIs). For outcomes with two categories, binary multiple logistic regression was utilized.
4. Discussion
This study aimed to assess the prevalence of wheezing and its association with environmental tobacco smoke exposure, a common symptom of asthma, among preschool children residing in rural and urban areas of Mpumalanga province, South Africa. The reported prevalence of wheeze in Mpumalanga is similar to that observed in previous research. Based on the findings of the ISAAC Phase Three study, it was determined that the worldwide prevalence of current wheeze among school-aged children was 11.5%. This prevalence showed significant regional variation, varying from 6.8% in the Indian subcontinent to 21% in Oceania [
15]. Furthermore, the prevalence of Current Wheeze (10%) and lifetime asthma (3.4%) in Africa exhibited a comparable pattern to the outcomes observed in our study [
15]. Additionally, the findings of Huq et al. [
16] who assessed allergy symptoms and diagnosis among children aged three years and five months from the Venda Health Examination of Mothers, Babies and their Environment (VHEMBE), Limpopo province in South Africa, support our study results. The prevalence of wheezing (4.7%) observed in their study aligns with the findings of our study.
The potential influence of various factors on the prevalence of asthma symptoms within a given region can be attributed to several key variables, including the age range of children considered in the study, the prevailing climate conditions, the specific timing of the study, the size of the sampled population, the design of the study itself, and the presence or absence of certain risk factors. Research studies that specifically examine children within similar age groups, as well as children residing in a particular place for a duration beyond six months, have found comparable rates of asthma symptom prevalence. Based on the aforementioned findings, it is evident that the management of asthma symptoms poses a persistent problem. Consequently, it may be necessary to formulate and execute strategies aimed at mitigating these symptoms within this specific demographic promptly.
This study found that there was a higher prevalence of Wheeze Ever and Asthma Ever among preschoolers living in urban areas compared to those residing in rural areas. Consistent with the results of our study, Levin et al. [
17], Feng et al. [
18], Rodriguez et al. [
19], and Kutzora et al. [
11] conducted research in South Africa, in China, a systematic review, and in Germany, respectively, which also indicated a greater prevalence of asthma and or symptoms among children residing in urban regions compared to those dwelling in rural areas. The present study found that children residing in the Mpumalanga Highveld region were predominantly impacted by Wheeze Ever, a common symptom of asthma, and also had a history of Asthma Ever, particularly if they attended an urban preschool. The results of our study align with the majority of the existing literature, which consistently demonstrates that residing in rural areas or on farms, being exposed to livestock, and the hygiene hypothesis confer protective advantages against the development of asthma and or symptoms in childhood compared to children residing in urban areas [
11,
20]. Additionally, our research findings provide support for the notion that children residing in urban areas are more prone to increased exposure and heightened sensitivity to several risk factors associated with asthma and or symptoms [
21].
The study outcome indicated above may have been influenced by specific environmental factors. The regions of Mpumalanga Highveld exhibit a notable deterioration in air quality, with heightened levels of pollutants stemming from both industrial and non-industrial origins. The district encompasses a variety of sectors, namely power generating, petrochemical, primary metallurgy, and open-cast mining. Urban environments possess a multitude of modifiable exposures that can impact the prevalence and morbidity of asthma symptoms. In the aggregate of both rural and urban areas, boys had a greater propensity for experiencing Wheeze Ever at any point and Current Severe Wheeze in comparison to their girl counterparts.
This observation aligns with previous research indicating that boys consistently have a higher incidence of wheezing and/or asthma symptoms relative to girls [
4,
22].
Risk factors and confounders associated with wheeze, a symptom commonly observed in individuals with asthma, were identified in our study. The risk factors with the highest potential for modification encompassed a female parent who engages in smoking, a male parent who engages in smoking, the number of individuals residing in the same household as a child and who engage in smoking, exposure to smoking within the home (within the previous 30 days), exposure to smoking within a motor vehicle or transportation (within the previous 30 days), exposure to smoking within a restaurant (within the previous 30 days), the mode of transportation utilized to commute to school, and ownership of a pet.
This study found that preschoolers were more likely to experience Wheeze Ever and Current Wheeze in their lives, if they had a female parent or caregiver who smoked, and if they lived in the same household as one or more people who smoked. Those who were exposed to smoking in cars and restaurants in the past 30 days were more likely to present with Current Wheeze. The results of our study are consistent with the existing literature, which indicates that children are primarily exposed to environmental tobacco smoke (ETS) through smoking by adults in environments where children reside and engage in recreational activities. This exposure significantly increases their susceptibility to developing asthma and or symptoms [
23,
24,
25].
According to studies conducted by Farzan et al. [
26] and Shahunja et al. [
27], there exists a significant relationship between the prevalence of asthma symptoms in children and their exposure to household tobacco smoke. Moreover, Wang et al. [
28] conducted a study that revealed a significant relationship between the presence of wheezing symptoms in children and their exposure to second-hand smoke. In addition, Tabuchi et al. [
29] and Harju et al. [
30] also reported that children who had two smoking parents were more likely to have asthma symptoms and had a greater chance of asthma attacks relative to children with non-smoking parents. Simic et al. [
31] provided additional support for the aforementioned results since they demonstrated that there are significant differences in the episodes of asthma symptoms in children depending on the area or room within which parents smoked the cigarettes.
Although the presence of second-hand smoke has been identified as a significant indicator of asthma symptoms, there remains a lack of consensus regarding the specific threshold at which exposure to smoking becomes detrimental. It is thus highly advisable to completely refrain from exposure to second-hand smoke and to ensure that household members who smoke confine their smoking activities to isolated areas that are inaccessible to these children. Parents should additionally take into consideration the implementation of a prohibition on smoking within the confines of their residence or its immediate vicinity.
Additionally, our study revealed that preschool-aged children who have been subjected to ETS in cars or transport without a complete physical barrier within the last 30 days were shown to have a higher likelihood of experiencing Current Wheeze. In addition, our research revealed an association between the utilization of motor vehicles for transportation to school among preschool-aged children and an increased likelihood of experiencing Wheeze Ever.
The anticipated outcomes of this study are in line with expectations, as the act of parents or caregivers smoking in the car during the transportation of children to school has been found to elevate exposure to ETS and therefore raise the probability of experiencing symptoms associated with asthma. The existing body of literature on the exposure of children to ETS and its impact on the development of respiratory and asthma symptoms provides substantial data that aligns with the findings of the aforementioned study [
24,
32]. Additionally, the use of motor vehicles may contribute to an increased likelihood of experiencing symptoms associated with asthma. Gasana and colleagues [
33] conducted a study that corroborated the aforementioned findings, as they concluded that children who are exposed to elevated amounts of air pollution from motor vehicles are more likely to exhibit symptoms of childhood wheezing. Lau et al. [
34] reported that traffic-related exposure tends to be closely related to asthma and or wheezing in children. Moreover, Suhaimi and colleagues [
35] found that children in elevated-traffic areas were four times more likely to present with wheezing as compared to children in low-traffic areas. It is advisable to prioritize the avoidance of ETS exposure as a crucial factor in mitigating the onset and facilitating the control of asthma and related symptoms.
5. Strength and Limitation of the Study
Firstly, the ISAAC questionnaire is a valid tool for data collection for this investigated population group and has been utilized worldwide in studies investigating asthma symptoms. Secondly, this study had a great participation rate with over 3000 children, which is a requirement of ISAAC centres, thus increasing the study’s statistical power. Finally, the implementation of a standardized and validated tool facilitates the ability to compare study findings with those of other studies conducted at various levels, including local, regional, and international contexts.
The study outcomes may deviate slightly from the actual prevalence of investigated symptoms due to the presence of missing data. Future research endeavours should prioritize the meticulous completion of questionnaires, aiming to minimize the occurrence of missing data to a significant extent. The study gathered data from the past year by using a parental-completed questionnaire. It was anticipated that these parents, who primarily reside with the children, would be able to accurately recall the information requested. The one-year timeframe was considered sufficient for recollection, without posing significant obstacles. The study was conducted during the COVID-19 period which had an impact on the implementation of the study methodology due to limited accessibility to the study areas and the availability of preschoolers to participate in the study.




{kind=link}