
Evaluating Intraocular Pressure Alterations during Large Muscle Group Isometric Exercises with Varying Head and Body Positions

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.2.1. Ophthalmological Examination
2.2.2. Isometric Exercises
2.2.3. Intraocular Pressure Measurement
2.3. Data Analysis
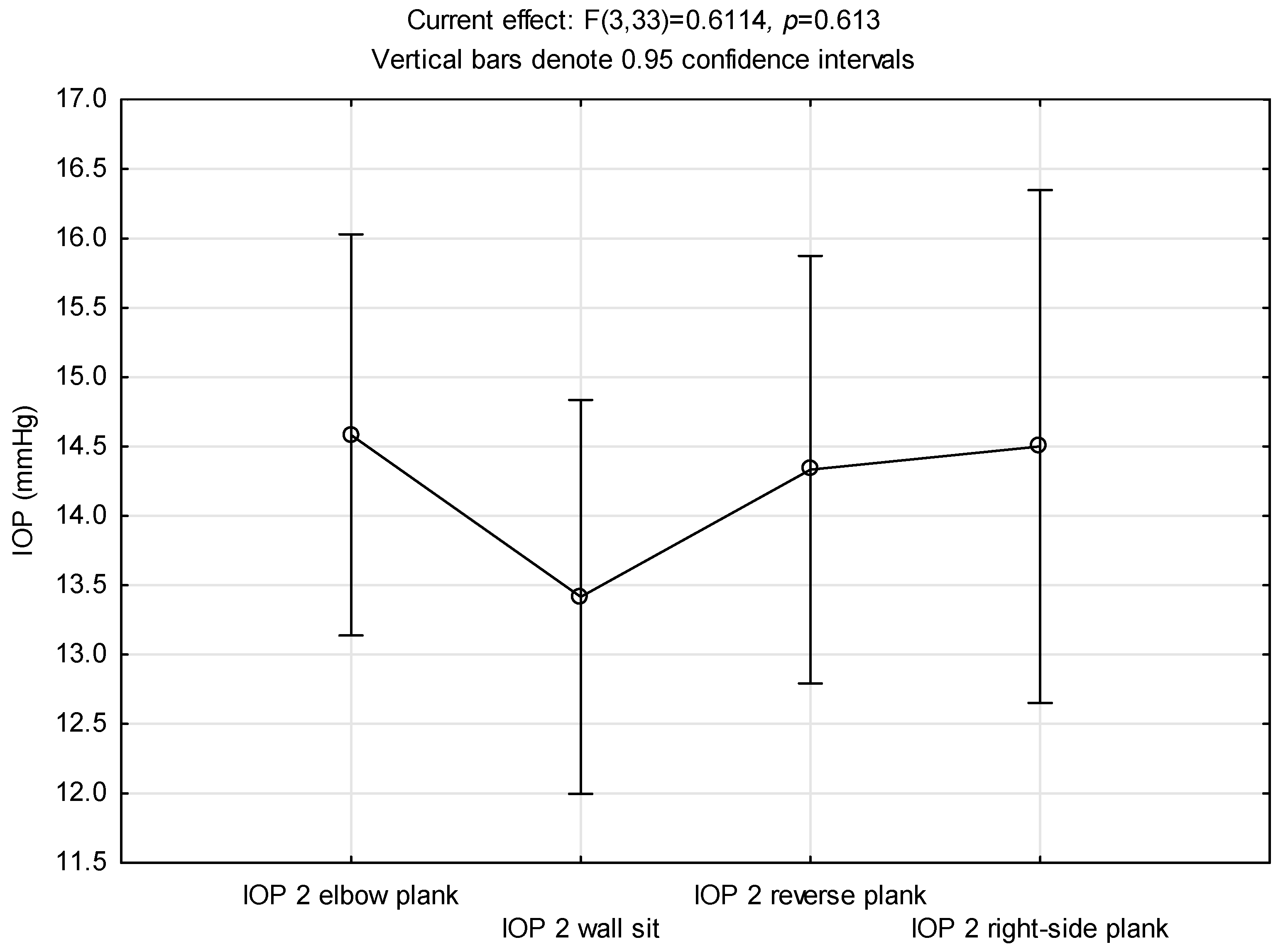
3. Results
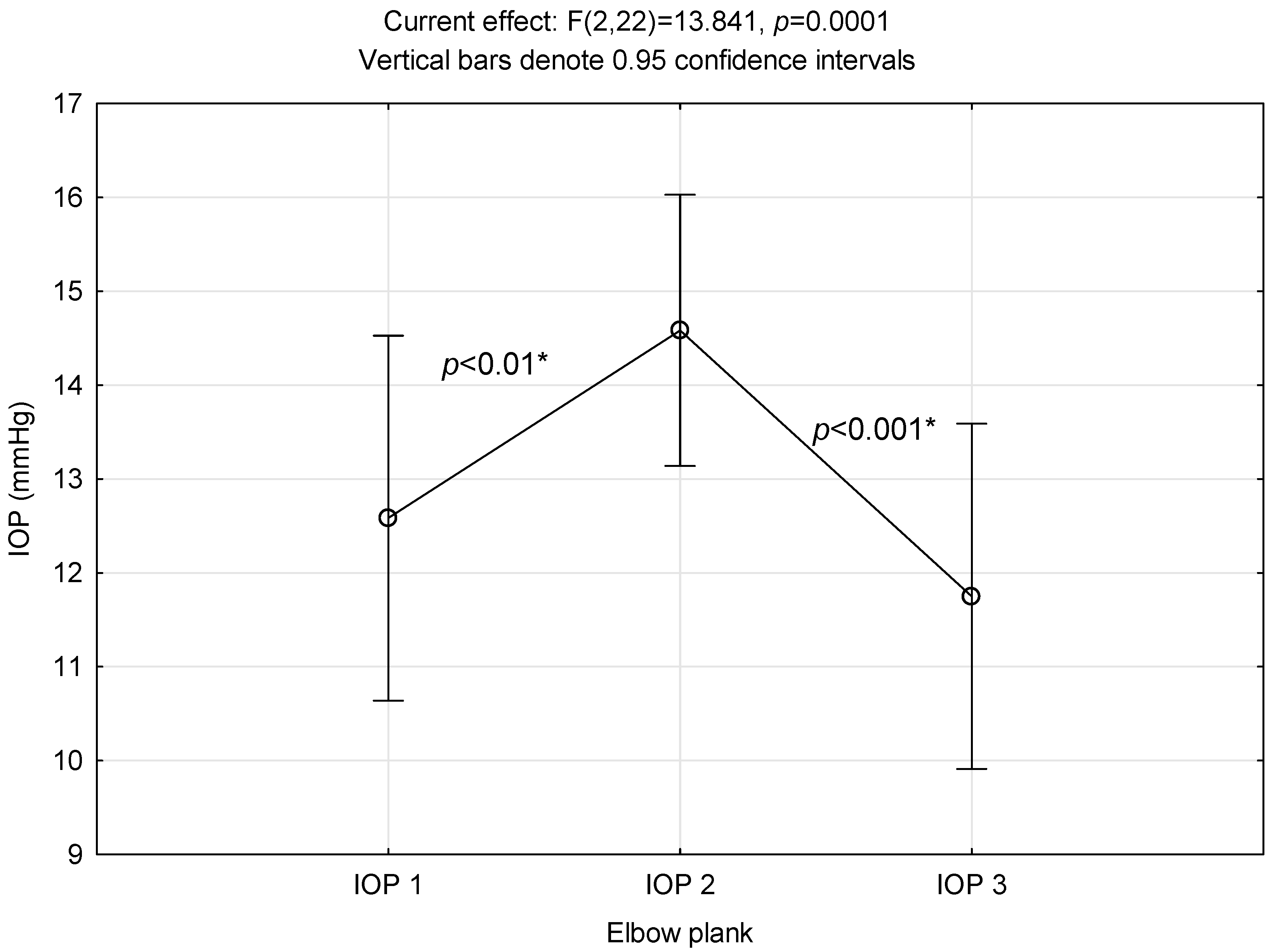
3.1. Elbow Plank
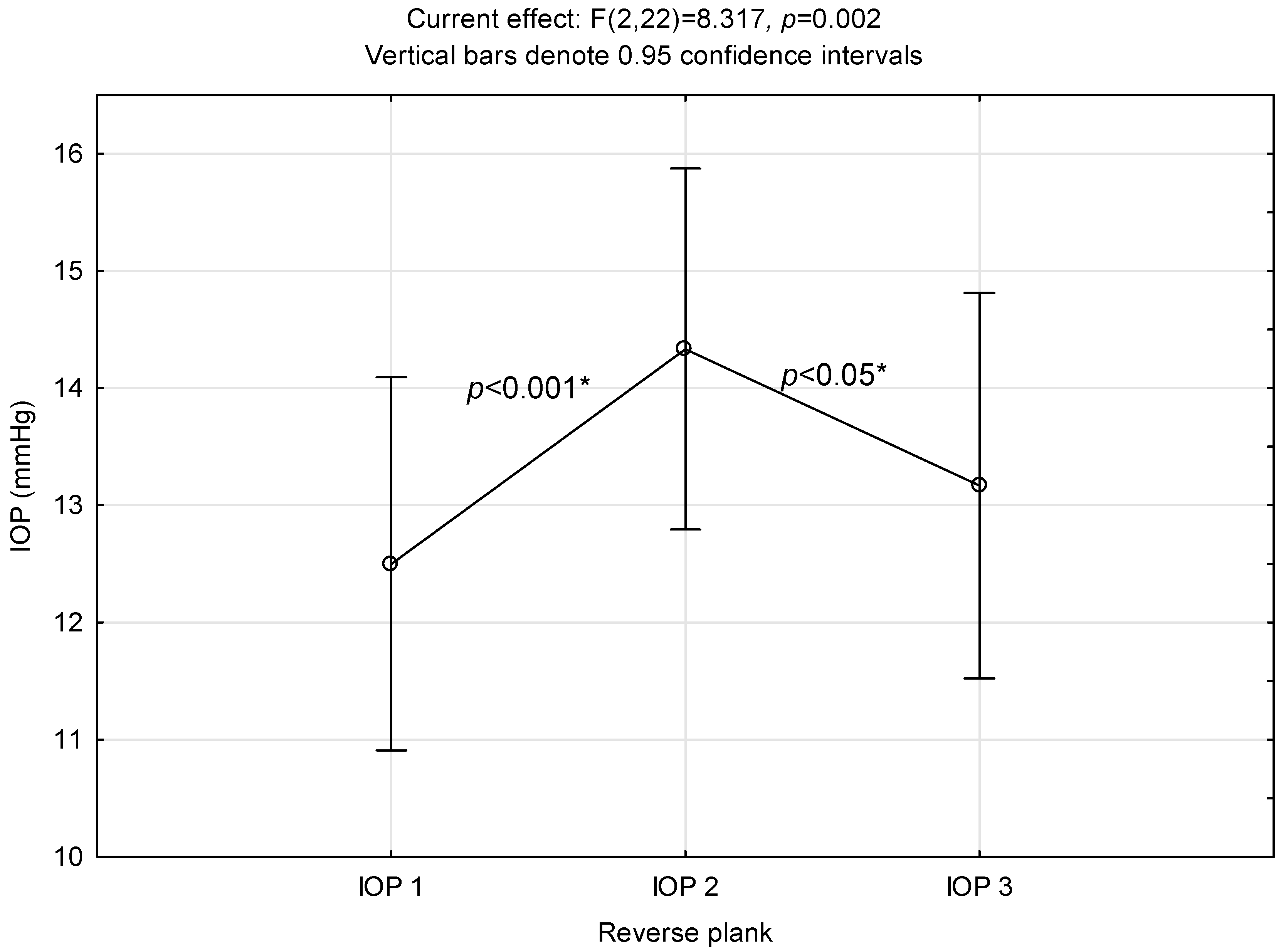
3.2. Reverse Plank
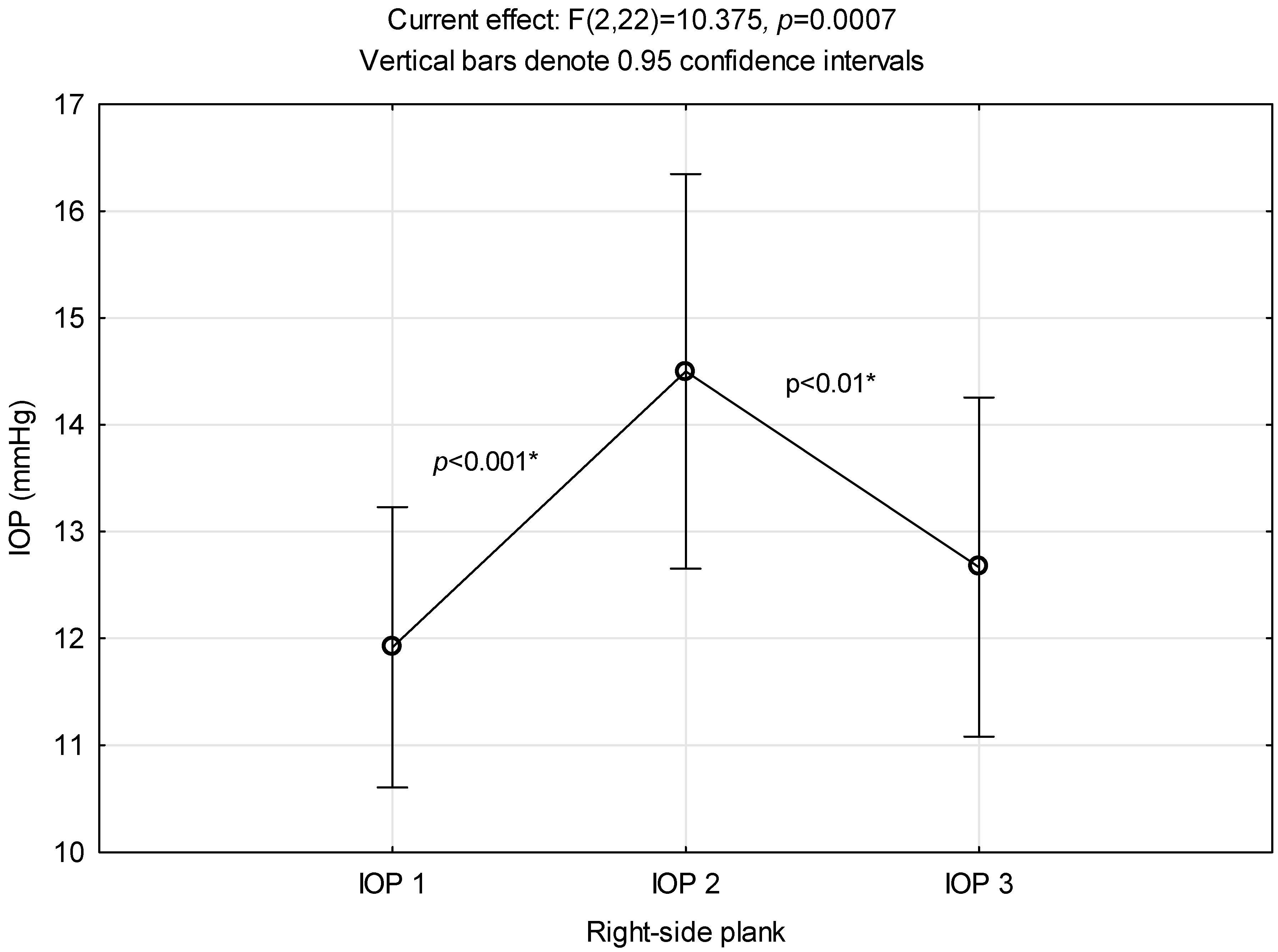
3.3. Right-Side Plank
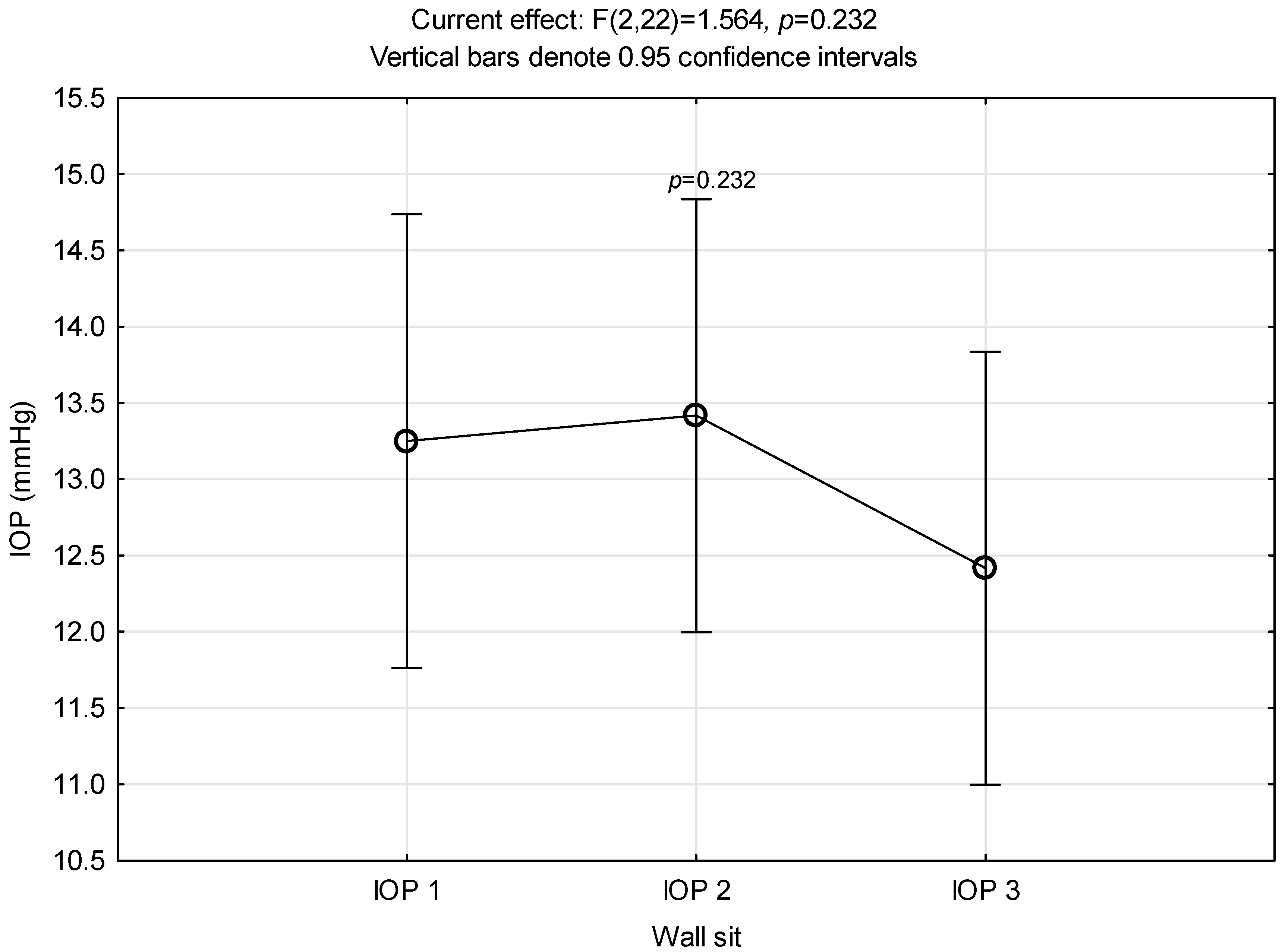
3.4. Wall Sit
3.5. The Head Position
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lum, D.; Barbosa, T.M. Brief Review: Effects of Isometric Strength Training on Strength and Dynamic Performance. Int. J. Sports Med. 2019, 40, 363–375. [Google Scholar] [CrossRef]
- Lee, B.C.; McGill, S.M. Effect of long-term isometric training on core/torso stiffness. J. Strength Cond. Res. 2015, 29, 1515–1526. [Google Scholar] [CrossRef] [PubMed]
- Oliva-Lozano, J.M.; Muyor, J.M. Core Muscle Activity During Physical Fitness Exercises: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4306. [Google Scholar] [CrossRef] [PubMed]
- Sax van der Weyden, M.; Toczko, M.; Fyock-Martin, M.; Martin, J. Relationship between a Maximum Plank Assessment and Fitness, Health Behaviors, and Moods in Tactical Athletes: An Exploratory Study. Int. J. Environ. Res. Public Health 2022, 19, 12832. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Massa, B.; Vecchiato, M.; Mazza, F.; De Blasiis, P.; Romano, A.M.; Di Salvatore, M.G.; Della Valle, E.; Tarantino, D.; Ruosi, C.; et al. Indirect Structural Muscle Injuries of Lower Limb: Rehabilitation and Therapeutic Exercise. J. Funct. Morphol. Kinesiol. 2021, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, P.C.; Lehnen, A.M.; Waclawovsky, G. Effect of isometric exercise on blood pressure in prehypertensive and hypertensive individuals: Protocol for a systematic review and meta-analysis of randomized controlled trials. Syst. Rev. 2022, 11, 100. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, 144–160. [Google Scholar] [CrossRef]
- Kim, Y.W.; Park, K.H. Exogenous influences on intraocular pressure. Br. J. Ophthalmol. 2019, 103, 1209–1216. [Google Scholar] [CrossRef]
- McMonnies, C.W. Glaucoma history and risk factors. J. Optom. 2017, 10, 71–78. [Google Scholar] [CrossRef]
- Gardiner, S.K.; Johnson, C.A.; Demirel, S. Factors predicting the rate of functional progression in early and suspected glaucoma. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3598–3604. [Google Scholar] [CrossRef]
- Chromiak, J.A.; Abadie, B.R.; Braswell, R.A.; Koh, Y.S.; Chilek, D.R. Resistance training exercises acutely reduce intraocular pressure in physically active men and women. J. Strength Cond. Res. 2003, 17, 715–720. [Google Scholar] [PubMed]
- Risner, D.; Ehrlich, R.; Kheradiya, N.S.; Siesky, B.; McCranor, L.; Harris, A. Effects of exercise on intraocular pressure and ocular blood flow: A review. J. Glaucoma 2009, 18, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Vieira, G.M.; Oliveira, H.B.; de Andrade, D.T.; Bottaro, M.; Ritch, R. Intraocular pressure variation during weight lifting. Arch. Ophthalmol. 2006, 124, 1251–1254. [Google Scholar] [CrossRef] [PubMed]
- Dane, Ş.; Koçer, I.; Demirel, H.; Ucok, K.; Tan, Ü. Effect of acute submaximal exercise on intraocular pressure in athletes and sedentary subjects. Int. J. Neurosci. 2006, 116, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Vera, J.; Redondo, B.; Koulieris, G.A.; Torrejon, A.; Jiménez, R.; Garcia-Ramos, A. Intraocular Pressure Responses to Four Different Isometric Exercises in Men and Women. Optom. Vis. Sci. 2020, 97, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Bakke, E.F.; Hisdal, J.; Semb, S.O. Intraocular pressure increases in parallel with systemic blood pressure during isometric exercise. Investig. Ophthalmol. Vis. Sci. 2009, 50, 760–764. [Google Scholar] [CrossRef] [PubMed]
- Malihi, M.; Sit, A.J. Effect of head and body position on intraocular pressure. Ophthalmology 2012, 119, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Prata, T.S.; De Moraes, C.G.; Kanadani, F.N.; Ritch, R.; Paranhos, A., Jr. Posture-induced intraocular pressure changes: Considerations regarding body position in glaucoma patients. Surv. Ophthalmol. 2010, 55, 445–453. [Google Scholar] [CrossRef]
- Vera, J.; Jiménez, R.; Redondo, B.; Cárdenas, D.; García-Ramos, A. Fitness Level Modulates Intraocular Pressure Responses to Strength Exercises. Curr. Eye Res. 2018, 43, 740–746. [Google Scholar] [CrossRef]
- Kiss, B.; Dallinger, S.; Polak, K.; Findl, O.; Eichler, H.G.; Schmetterer, L. Ocular hemodynamics during isometric exercise. Microvasc. Res. 2001, 61, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vera, J.; Jiménez, R.; Redondo, B.; Torrejón, A.; Koulieris, G.A.; De Moraes, C.G.; García-Ramos, A. Investigating the Immediate and Cumulative Effects of Isometric Squat Exercise for Different Weight Loads on Intraocular Pressure: A Pilot Study. Sports Health 2019, 11, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Matlach, J.; Bender, S.; König, J.; Binder, H.; Pfeiffer, N.; Hoffmann, E.M. Investigation of intraocular pressure fluctuation as a risk factor of glaucoma progression. Clin. Ophthalmol. 2018, 13, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.P.; Sultan, M.B.; Grunden, J.W.; Cioffi, G.A.; Consensus Panel. Assessing the Importance of IOP Variables in Glaucoma Using a Modified Delphi Process. J. Glaucoma 2010, 19, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Polska, E.; Luksch, A.; Schering, J.; Frank, B.; Imhof, A.; Fuchsjäger-Mayrl, G.; Wolzt, M.; Schmetterer, L. Propranolol and atropine do not alter choroidal blood flow regulation during isometric exercise in healthy humans. Microvasc. Res. 2003, 65, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Wimpissinger, B.; Resch, H.; Berisha, F.; Weigert, G.; Polak, K.; Schmetterer, L. Effects of isometric exercise on subfoveal choroidal blood flow in smokers and nonsmokers. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4859–4863. [Google Scholar] [CrossRef] [PubMed]
- Rüfer, F.; Schiller, J.; Klettner, A.; Lanzl, I.; Roider, J.; Weisser, B. Comparison of the influence of aerobic and resistance exercise of the upper and lower limb on intraocular pressure. Acta Ophthalmol. 2014, 92, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, S.; Wang, Y.; Zhou, J.; Yang, J.; Ma, J. Effects of isometric resistance exercise of the lower limbs on intraocular pressure and ocular perfusion pressure among healthy adults: A meta-analysis. J. Fr. Ophtalmol. 2021, 44, 1596–1604. [Google Scholar] [CrossRef] [PubMed]
- Lara, P.M.; Redondo, B.; Jerez-Mayorga, D.; Martínez-García, D.; García-Ramos, A.; Vera, J. Influence of the body positions adopted for resistance training on intraocular pressure: A comparison between the supine and seated positions. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 1971–1978. [Google Scholar] [CrossRef]
- Lee, T.E.; Yoo, C.; Kim, Y.Y. Effects of different sleeping postures on intraocular pressure and ocular perfusion pressure in healthy young subjects. Ophthalmology 2013, 120, 1565–1570. [Google Scholar] [CrossRef]
- Sultan, M.; Blondeau, P. Episcleral venous pressure in younger and older subjects in the sitting and supine positions. J. Glaucoma 2003, 12, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Burgoyne, C.F.; Downs, J.C. Premise and prediction-how optic nerve head biomechanics underlies the susceptibility and clinical behavior of the aged optic nerve head. J. Glaucoma 2008, 17, 318–328. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women (n = 7) | Men (n = 5) | |
|---|---|---|
| Age (y) | 29.00 ± 2.65 | 28.2 ± 2.17 |
| Height (cm) | 169.00 ± 7.48 | 182.6 ± 5.08 |
| Weight (kg) | 64.00 ± 7.16 | 84.2 ± 5.36 |
| BMI (kg/m2) | 22.43 ± 2.58 | 25.36 ± 2.68 |
| IOP1 * | IOP2 ** | IOP3 *** | |
|---|---|---|---|
| Wall sit | 13.25 (±2.34) | 13.42 (±2.23) | 12.42 (±2.23) |
| Elbow plank | 12.58 (±3.06) | 14.58 (±2.27) | 11.75 (±2.90) |
| Reverse plank | 12.50 (±2.50) | 14.33 (±2.42) | 13.17 (±2.59) |
| Right side plank | 11.92 (±2.06) | 14.50(±2.91) | 12.67 (±2.50) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krobot Cutura, N.; Mrak, M.; Cutura, D.-M.; Petric Vickovic, I.; Ruzic, L. Evaluating Intraocular Pressure Alterations during Large Muscle Group Isometric Exercises with Varying Head and Body Positions. Int. J. Environ. Res. Public Health 2024, 21, 476. https://doi.org/10.3390/ijerph21040476
Krobot Cutura N, Mrak M, Cutura D-M, Petric Vickovic I, Ruzic L. Evaluating Intraocular Pressure Alterations during Large Muscle Group Isometric Exercises with Varying Head and Body Positions. International Journal of Environmental Research and Public Health. 2024; 21(4):476. https://doi.org/10.3390/ijerph21040476
Chicago/Turabian StyleKrobot Cutura, Nina, Maksimilijan Mrak, Dominik-Mate Cutura, Ivanka Petric Vickovic, and Lana Ruzic. 2024. "Evaluating Intraocular Pressure Alterations during Large Muscle Group Isometric Exercises with Varying Head and Body Positions" International Journal of Environmental Research and Public Health 21, no. 4: 476. https://doi.org/10.3390/ijerph21040476
APA StyleKrobot Cutura, N., Mrak, M., Cutura, D.-M., Petric Vickovic, I., & Ruzic, L. (2024). Evaluating Intraocular Pressure Alterations during Large Muscle Group Isometric Exercises with Varying Head and Body Positions. International Journal of Environmental Research and Public Health, 21(4), 476. https://doi.org/10.3390/ijerph21040476