
Interventions to Foster Resilience in Family Caregivers of People with Alzheimer’s Disease: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Research Question
2.3. Search Strategy
Results Management
2.4. Selecting Studies: Inclusion and Exclusion Criteria
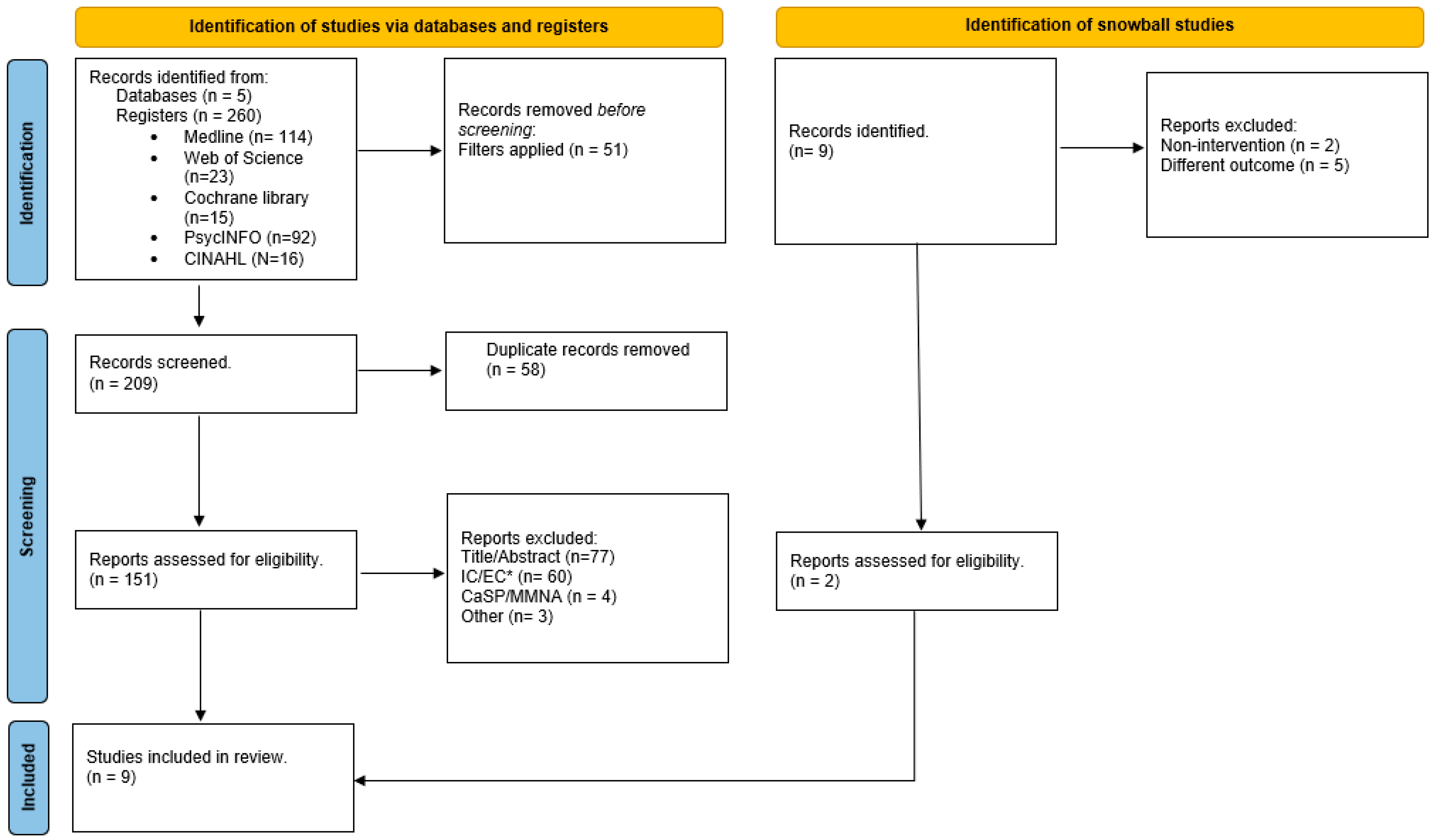
2.5. Selection of Evidence Sources
2.5.1. Quality Appraisal
2.5.2. Outcomes of the Methodological Critique of the Articles
2.6. Data Charting and Synthesis
3. Results
3.1. Resilience
3.2. Other Health Outcomes That Have Been Studied Together with Resilience
3.3. Profile of the Caregiver Receiving the Intervention
3.4. Implication of Nursing Professionals and Main Features of the Interventions
3.4.1. Nursing Professionals
3.4.2. Interventions
Interventions Based on Creative Art
Multicomponent Interventions Based on Psychoeducation
Interventions Based on Meditation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Strategy and Action Plan on Ageing and Health (2016–2020); World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/252783/A69_R3-en.pdf?sequence=1 (accessed on 7 August 2022).
- López-Picazo, J.J.; de Dios Cánovas-García, J.; Antúnez, C.; Marín, J.; Antequera, M.M.; Vivancos, L.; Martínez, B.; Legaz, A.; Navarro, D.; Leal, M. Perceived quality in a dementia unit: Patients’ caregivers as information providers. Neurologia 2018, 33, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Escobar, J.; Del-Moral-Sánchez, J.; García-Ramos-García, R.; Matías-Guiu-Guía, J.; Gómez-Pastor, I.; Martín-Acero, T.; Carrasco-Marín, L.; Mayor-de-Frutos, A. Strategy on Neurodegenerative Diseases of the National Health System MINISTRY OF HEALTH, SOCIAL SERVICES AND EQUALITY. Ministerio De Sanidad, Servicios Sociales E Igualdad. 2016. Available online: https://www.sefac.org/sites/default/files/sefac2010/private/documentos_sefac/documentos/Estrategia_Neurodegenerativas_2016CIT.pdf (accessed on 18 April 2021).
- Prince, M.J.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.M.M.; Karagiannidou, M. World Alzheimer Report 2016-Improving Healthcare for People Living with Dementia: Coverage, Quality and Costs Now and in the Future. Alzheimer’s Disease International (ADI). 2016. Available online: https://kclpure.kcl.ac.uk/portal/en/publications/world-alzheimer-report-2016--improving-healthcare-for-people-living-with-dementia-coverage-quality-and-costs-now-and-in-the-future(d77a0786-a217-4001-8951-04011d7f4adf).html (accessed on 26 September 2022).
- Zvěřová, M. Alzheimer’s disease and blood-based biomarkers–Potential contexts of use. Neuropsychiatr. Dis. Treat. 2018, 14, 1877. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.C.; Zelman, D.C. Caregiver expressed emotion as mediator of the relationship between neuropsychiatric symptoms of dementia patients and caregiver mental health in Hong Kong. Aging Ment. Health 2020, 24, 1690–1699. [Google Scholar] [CrossRef] [PubMed]
- Deb, A.; Thornton, J.D.; Sambamoorthi, U.; Innes, K. Direct and Indirect Cost of Managing Alzheimer’s Disease and Related Dementias in the United States. Expert Rev. Pharmacoecon Outcomes Res. 2017, 17, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Bekhet, A.K.; Avery, J.S. Resilience from the Perspectives of Caregivers of Persons with Dementia. Arch. Psychiatr. Nurs. 2018, 32, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Handels, R.L.H.; Sköldunger, A.; Bieber, A.; Edwards, R.T.; Gonçalves-Pereira, M.; Hopper, L.; Irving, K.; Jelley, H.; Kerpershoek, L.; Marques, M.J.; et al. Quality of Life, Care Resource Use, and Costs of Dementia in 8 European Countries in a Cross-Sectional Cohort of the Actifcare Study. J. Alzheimer’s Dis. 2018, 66, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Ruisoto, P.; Contador, I.; Fernández-Calvo, B.; Serra, L.; Jenaro, C.; Flores, N.; Ramos, F.; Rivera-Navarro, J. Mediating effect of social support on the relationship between resilience and burden in caregivers of people with dementia. Arch. Gerontol. Geriatr. 2020, 86, 103952. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ji, M.; Leng, M.; Li, X.; Zhang, X.; Wang, Z. Comparative efficacy of 11 non-pharmacological interventions on depression, anxiety, quality of life, and caregiver burden for informal caregivers of people with dementia: A systematic review and network meta-analysis. Int. J. Nurs. Stud. 2022, 129, 104204. [Google Scholar] [CrossRef]
- García del Castillo, J.A.; García del Castillo-López, Á.; López-Sánchez, C.; Dias, P.C. Theoretical conceptualization of psychosocial resilience and its relationship with health. Health Addict. 2016, 16, 59–68. Available online: https://www.redalyc.org/articulo.oa?id=83943611006 (accessed on 7 July 2021).
- Caro, P.; Rodríguez-Martín, B.; Caro, A. Potentials of resilience for nursing professionals. Index. Enfermería 2018, 27, 42–46. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962018000100009&lng=es&nrm=iso&tlng=es (accessed on 11 March 2022).
- Deist, M.; Greeff, A.P. Living with a parent with dementia: A family resilience study. Dementia 2017, 16, 126–141. [Google Scholar] [CrossRef] [PubMed]
- Herdman, H.; Kamitsuru, S. NANDA International Nursing Diagnoses: Definitions and Classification: 2018–2020; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Cheng, S.T.T.; Li, K.K.K.; Losada, A.; Zhang, F.; Au, A.; Thompson, L.W.; Gallagher-Thompson, D. The effectiveness of nonpharmacological interventions for informal dementia caregivers: An updated systematic review and meta-analysis. Psychol. Aging 2020, 35, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Fitting, H. Alzheimer’s patients and their caregivers: Nursing interventions. Der Reichs Civilproceß 2021, 3, 565–588. [Google Scholar]
- Bourgeois, M.S.; Schulz, R.; Burgio, L. Interventions for caregivers of patients with Alzheimer’s disease: A review and analysis of content, process, and outcomes. Int. J. Aging Hum. Dev. 1996, 43, 35–92. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Guzmán, M.; Sánchez-Villegas, M.; Bahamón, M.J.; Arenas Landgrave, P. Resiliencia y cáncer de mama: Una revisión sistemática. Arch. Venez. Farmacol. Ter. 2020, 39, 326–333. [Google Scholar]
- Lin, P.J.J.; D’Cruz, B.; Leech, A.A.; Neumann, P.J.; Sanon Aigbogun, M.; Oberdhan, D.; Lavelle, T.A. Family and Caregiver Spillover Effects in Cost-Utility Analyses of Alzheimer’s Disease Interventions. Pharmacoeconomics 2019, 37, 597–608. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=135876222&lang=es&site=ehost-live&scope=site (accessed on 14 August 2021). [CrossRef]
- Ornelas Tavares, P.E. Coping strategies and resilience in grieving primary caregivers. Rev. Psicol. Y Salud 2016, 26. Available online: https://psicologiaysalud.uv.mx/index.php/psicysalud/article/view/2193 (accessed on 15 March 2022).
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Zhou, Y.; Strayer, A.T.; Phelan, E.A.; Sadak, T.; Hooyman, N.R. A mixed methods systematic review of informal caregivers’ experiences of fall risk among community-dwelling elders with dementia. Health Soc. Care Community 2021, 29, 1126–1144. [Google Scholar] [CrossRef] [PubMed]
- Villarejo Galende, A.; Eimil Ortiz, M.; Llamas Velasco, S.; Llanero Luque, M.; López de Silanes de Miguel, C.; Prieto Jurczynska, C. Report by the Spanish Foundation of the Brain on the social impact of Alzheimer disease and other types of dementia. Neurologia 2021, 36, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Elston, D.M. Mendeley. J. Am. Acad. Dermatol. 2019, 81, 1071. [Google Scholar] [CrossRef] [PubMed]
- CASPe. Critical Appraisal Skills Programme [Internet]. 2022. Available online: https://redcaspe.org/ (accessed on 1 October 2021).
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Cerquera, A.; Pabón, D.; Ruíz, A. Implementation of the psychological intervention program in resilience for informal caregivers of patients with Alzheimer’s dementia PIRCA. Univ. Psychol. 2017, 12, 2. [Google Scholar] [CrossRef]
- Ghaffari, F.; Rostami, M.; Fotokian, Z.; Hajiahmadi, M. Effectiveness of resilience education in the mental health of family caregivers of elderly patients with Alzheimer’s disease. Iran. J. Psychiatry Behav. Sci. 2019, 13, e69507. [Google Scholar] [CrossRef]
- Leach, M.J.; Francis, A.; Ziaian, T. Transcendental Meditation for the improvement of health and wellbeing in community-dwelling dementia caregivers [TRANSCENDENT]: A randomised wait-list controlled trial. BMC Complement. Altern. Med. 2015, 15, 145. [Google Scholar] [CrossRef]
- Orrell, M.; Yates, L.; Leung, P.; Kang, S.; Hoare, Z.; Whitaker, C.; Burns, A.; Knapp, M.; Leroi, I.; Moniz-Cook, E.; et al. The impact of individual Cognitive Stimulation Therapy (iCST) on cognition, quality of life, caregiver health, and family relationships in dementia: A randomised controlled trial. PLoS Med. 2017, 14, e1002269. [Google Scholar] [CrossRef]
- Pandya, S.P. Meditation Program Enhances Self-efficacy and Resilience of Home-based Caregivers of Older Adults with Alzheimer’s: A Five-year Follow-up Study in Two South Asian Cities. J. Gerontol. Soc. Work. 2019, 62, 663–681. [Google Scholar] [CrossRef]
- Hunt, B.; Truran, L.; Reynolds, F. “Like a drawing of breath”: Leisure-based art-making as a source of respite and identity among older women caring for loved ones with dementia. Arts Health 2016, 10, 29–44. [Google Scholar] [CrossRef]
- Pienaar, L.; Reynolds, F. A respite thing: A qualitative study of a creative arts leisure programme for family caregivers of people with dementia. Health Psychol. Open 2015, 2, 11. Available online: https://www.proquest.com/scholarly-journals/i-respite-thing-qualitative-study-creative-arts/docview/1985637260/se-2?accountid=14777 (accessed on 14 August 2021). [CrossRef] [PubMed]
- Kidd, L.I.; Zauszniewski, J.A.; Morris, D.L. Benefits of a poetry writing intervention for family caregivers of elders with dementia. Issues Ment. Health Nurs. 2011, 32, 598–604. [Google Scholar] [CrossRef] [PubMed]
- McManus, K.; Tao, H.; Jennelle, P.J.; Wheeler, J.C.; Anderson, G.A. The effect of a performing arts intervention on caregivers of people with mild to moderately severe dementia. Aging Ment. Health 2021, 26, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.; Crane, N.; Ings, R.; Taylor, K. Promoting well-being through creativity: How arts and public health can learn from each other. Perspect. Public Health 2013, 133, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Cancino, J.J.; Moreno-Pérez, N.E. Psychoeducation: Nursing intervention to care for the family in their role as caregiver. Enfermería Univ. 2017, 14, 207–218. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Chapleau, M.-A.; Paquin, K.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef]
- Lavretsky, H.; Siddarth, P.; Irwin, M.R. Improving depression and enhancing resilience in family dementia caregivers: A pilot randomized placebo-controlled trial of escitalopram. Am. J. Geriatr. Psychiatry 2010, 18, 154–162. [Google Scholar] [CrossRef]
- Córdoba, A.M.C. Resilience and Associated Variables in Informal Caregivers of Patients with Alzheimer’s; Poches, D.K.P., Ed.; Revista Colombiana de Psicología: Bucaramanga, Colombia, 2016; Volume 25, Available online: https://revistas.unal.edu.co/index.php/psicologia/article/view/44558 (accessed on 1 October 2021).
- Orgeta, V.; Leung, P.; Yates, L.; Kang, S.; Hoare, Z.; Henderson, C.; Whitaker, C.; Burns, A.; Knapp, M.; Leroi, I.; et al. Individual cognitive stimulation therapy for dementia: A clinical effectiveness and cost-effectiveness pragmatic, multicentre, randomised controlled trial. Health Technol. Assess. 2015, 19, 1–108. Available online: https://pubmed.ncbi.nlm.nih.gov/26292178/ (accessed on 14 August 2021). [CrossRef]
- González Piñeiro, M. A New Resilient Look at Caregivers of Patients with Dementia. 2019. Available online: http://riull.ull.es/xmlui/handle/915/14628 (accessed on 18 April 2021).
- Wagnild, G.M.; Young, H.M. Development and psychometric. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Espín Andrade, A.M.; Andrade, A.E.A. Psychosocial characterization of informal caregivers of older adults with dementia. Rev. Cub Salud Publica 2008, 34, 1–12. [Google Scholar]
- Vaquiro, S.; Stiepovich, J. Informal care, a challenge taken on by women. Sci. Nurs. Rev. En La. 2010, 9–16. [Google Scholar]
- Lee, M.; Ryoo, J.H.; Crowder, J.; Byon, H.D.; Wiiliams, I.C. A systematic review and meta-analysis on effective interventions for health-related quality of life among caregivers of people with dementia. J. Adv. Nurs. 2020, 76, 475–489. [Google Scholar] [CrossRef] [PubMed]
- Bonilla-Santos, J.; Calceto-Garavito, L.N.; Cala-Martínez, D.Y.; Gonzalez-Hernández, A. Caregiver influence on cognitive and functional decline in people with dementia: Systematic review. Med. De Fam. Semer. 2021, 47, 488–494. [Google Scholar]
- Pessotti, C.F.C.; Fonseca, L.C.; Tedrus, G.M.d.A.S.; Laloni, D.T. Family caregivers of elderly with dementia Relationship between religiosity, resilience, quality of life and burden. Dement. Neuropsychol. 2018, 12, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Losada, A.; Márquez-González, M.; Romero-Moreno, R.; Mausbach, B.T.; López, J.; Fernández-Fernández, V.; Nogales-González, C. Cognitive–behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for dementia family caregivers with significant depressive symptoms: Results of a randomized clinical trial. J. Consult. Clin. Psychol. 2015, 83, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Burnside, L.D.; Knecht, M.J.; Hopley, E.K.; Logsdon, R.G. Here:Now—Conceptual model of the impact of an experiential arts program on persons with dementia and their care partners. Dementia 2017, 16, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Leng, M.; Zhao, Y.; Xiao, H.; Li, C.; Wang, Z. Internet-based supportive interventions for family caregivers of people with dementia: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, 1–15. Available online: http://www.jmir.org/2020/9/e19468/ (accessed on 14 August 2021). [CrossRef]
- Scorsolini-Comin, F.; da Cunha, V.F.; Miasso, A.I.; Pillon, S.C. Mindfulness and Mental Health: Dialogues between Nursing and Positive Psychology. Index. Enfermería 2021, 30, 229–233. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962021000200016 (accessed on 6 July 2022).
- Matchar, B.G.; Gwyther, L.P. Resilience in early-stage dementia: Lessons learned from early-stage alzheimer education and support groups. Top. Geriatr. Rehabil. 2014, 30, 170–175. [Google Scholar] [CrossRef]


{kind=link}
| Group 1. Binding terms regarding type of chronic process. |
| Alzheimer Disease * OR Alzheimer’s Disease * |
| AND |
| Group 2. Binding terms regarding type of population. |
| Carer * OR Caregiver * OR Family caregiv * OR Spouse Caregiv * OR Informal Caregiv * |
| AND |
| Group 3. Binding terms regarding intervention. |
| Intervention * OR Multidisciplinary intervention * OR psychological multicomponent intervention * |
| AND |
| Group 4. Binding terms regarding outcomes. |
| Psychological resilience * OR Resilience * |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies that included people with Alzheimer’s disease in any stage of illness and/or their family caregivers. | Studies conducted on formal caregivers, understood as a person who is not part of the family, whether qualified or not to perform care, in exchange of a monetary compensation. |
| Studies whose population diagnosed with Alzheimer’s disease were 65 or older. | Studies in which those receiving care from family caregivers presented a neurodegenerative disease other than Alzheimer’s disease and/or were under 65 years of age. |
| Studies that explored or intervened on family caregivers of people with Alzheimer’s disease with a main or secondary objective of improving resilience. | Studies whose aim was not to improve resilience and/or did not used resilience as a method of eliciting other variables. |
| Studies involving non-pharmacological interventions. | Studies that chose external resources such as institutionalization or other types of resource or financial aid. |
| Full-text studies with qualitative, observational, analytical and/or mixed designs. | Letters to editorials, comments, literature reviews, guidelines, grey literature and research that did not meet quality criteria. |
| Main Author Year Country | Design Sample Main activity | Resilience Definition Measurement | Implementation Strategies | Outcomes |
|---|---|---|---|---|
| Pienaar L 2015 UK | Design: qualitative Sample: 4 caregivers (wives from 50 to 79 years old) Alzheimer’s disease severity: early, middle, and late stage Activity: to go to an art gallery and craft-making | Definition: No Measurement: transcription | Format: on-site (Healthy Aging Café) Total duration: 5 weeks Frequency: 4 sessions/90′ Agents: an occupational therapist and a psychologist Abandonment: 50% | Feelings of guilt and stress were reduced. Resilience and mental health took on a positive meaning. |
| Hunt B 2016 UK | Design: qualitative Sample: 6 caregivers (4 wives and 2 daughters from 60 to 77 years old) Alzheimer’s disease severity: middle and late stage Activity: to make a painting | Definition: Achieving relevant tasks despite adversity Measurement: transcription | Format: place of residence Total duration: Unknown Frequency: Unknown Agents: Occupational therapist Abandonment: Unknown | Psychological welfare, resilience, identity, relief and good mood were increased. |
| Kidd L 2011 US | Design: mixed Sample: 20 caregivers (17 women and 3 men from 41 to 80 years old) Alzheimer’s disease severity: early and middle stage Activity: poem writing | Definition: overcoming obstacles Measurement: Wagnild and Young resilience scale | Format: place of residence Total duration: 8 weeks Frequency: 1 poem/week Agents: nurses Abandonment: Unknown | Resilience and mental health were reduced. Depression and overload were increased. Conclusive quantitative outcomes cannot be drawn. Women and younger caregivers scored worse than men in all variables. |
| McManus K 2021 US | Design: mixed Sample: 32 dyads (wives, from 61 to 80 years old) Alzheimer’s disease severity: early and middle stage Activity: theatrical staging | Definition: No Measurement: Brief Resilience Scale | Format: on- site Total duration: 8 weeks Frequency: 1 h/week Agents: theatre instructors Abandonment: 37% | Overload and resilience caregiver were reduced. QoL* (person with Alzheimer’s disease) was reduced. |
| rell M 2017 UK | Design: RCT Sample: 356 dyads Alzheimer’s disease severity: early and middle stage Activity: cognitive stimulation | Definition: Synonym of QoL Measurement: Resilience Scale-14 | Format: place of residence Total duration: 25 weeks Frequency: 90′/week (75 sessions) Agents: Mental health nurses, clinical psychologists, occupational therapists or research assistants Abandonment: 23% | Relationship quality (according to the person with Alzheimer’s disease) and caregiver depression were increased. QoL*,cognition in the person with Alzheimer’s disease andcaregiver’s health status remained constant. |
| Cerquera A 2017 Colombia | Design: quasi-experimental Sample: 30 caregivers (women, from 55 to 80 years old) Alzheimer’s disease severity: early, middle, and late stage Activity: cognitive-behavioural stimulation | Definition: personality trait Measurement: Resilience Scale | Format: on-site Total duration: Unknown Frequency: 10 sessions/90′ Agents: Unknown Abandonment: 66.6% | Mood, resilience and social support were increased. It is not possible to conclude if it is effective on depression and stress or not. |
| Ghaffari F 2019 Iran | Design: RCT Sample: 54 caregivers (daughters, 43 years of age) Alzheimer’s disease severity: middle and late stage Activity: resilience psychoeducation | Definition: overcoming difficulties and adaptation Measurement: Connor-Davidson Resilience Scale | Format: on-site Total duration: 8 weeks Frequency: 30 caregivers (women, from 55 to 80 years old) Agents: Healthcare professionals Abandonment: 7.4% | Mental health, age-related resilience (greater), care giving duration (lower), income level and toxic habits (smoking) were increased. Depression, anxiety and insomnia were reduced. There were no relations between gender, kinship, civil status or educational level. |
| Leach MJ 2015 Australia | Design: RCT Sample: 17 caregivers (wives, 66 years old on average) Alzheimer’s disease severity: middle and late stage Activity: Transcendental meditation | Definition: NO Measurement: WebNeuro scores | Format: on-site Total duration: 12 weeks Frequency: Unknown Agents: Transcendental meditation instructor Abandonment: 52.7% | QoL*, depression and resilience remained constant. Stress was reduced. |
| Pandya S 2019 Asia | Design: quasi-experimental Sample: 185 caregivers (Hindu wives) Alzheimer’s disease severity: early, middle, and late stage Activity: Mindfulness meditation | Definition: No Measurement: resilience scale | Format: combined Total duration: 5 years Frequency: 1 session/45′ per week Agents: Transcendental meditation instructor Abandonment: 21.6% | Overload was reduced. Resilience and auto-efficacy were increased. Gender, kinship, religion, social status, education, employment, and assistance to 75% of sessions were decisive factors. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santonja-Ayuso, L.; Corchón-Arreche, S.; Portillo, M.C. Interventions to Foster Resilience in Family Caregivers of People with Alzheimer’s Disease: A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 485. https://doi.org/10.3390/ijerph21040485
Santonja-Ayuso L, Corchón-Arreche S, Portillo MC. Interventions to Foster Resilience in Family Caregivers of People with Alzheimer’s Disease: A Scoping Review. International Journal of Environmental Research and Public Health. 2024; 21(4):485. https://doi.org/10.3390/ijerph21040485
Chicago/Turabian StyleSantonja-Ayuso, Lucía, Silvia Corchón-Arreche, and Mari Carmen Portillo. 2024. "Interventions to Foster Resilience in Family Caregivers of People with Alzheimer’s Disease: A Scoping Review" International Journal of Environmental Research and Public Health 21, no. 4: 485. https://doi.org/10.3390/ijerph21040485