

Supported Standing and Supported Stepping Devices for Children with Non-Ambulant Cerebral Palsy: An Interdependence and F-Words Focus


Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. F-Words for Child Development
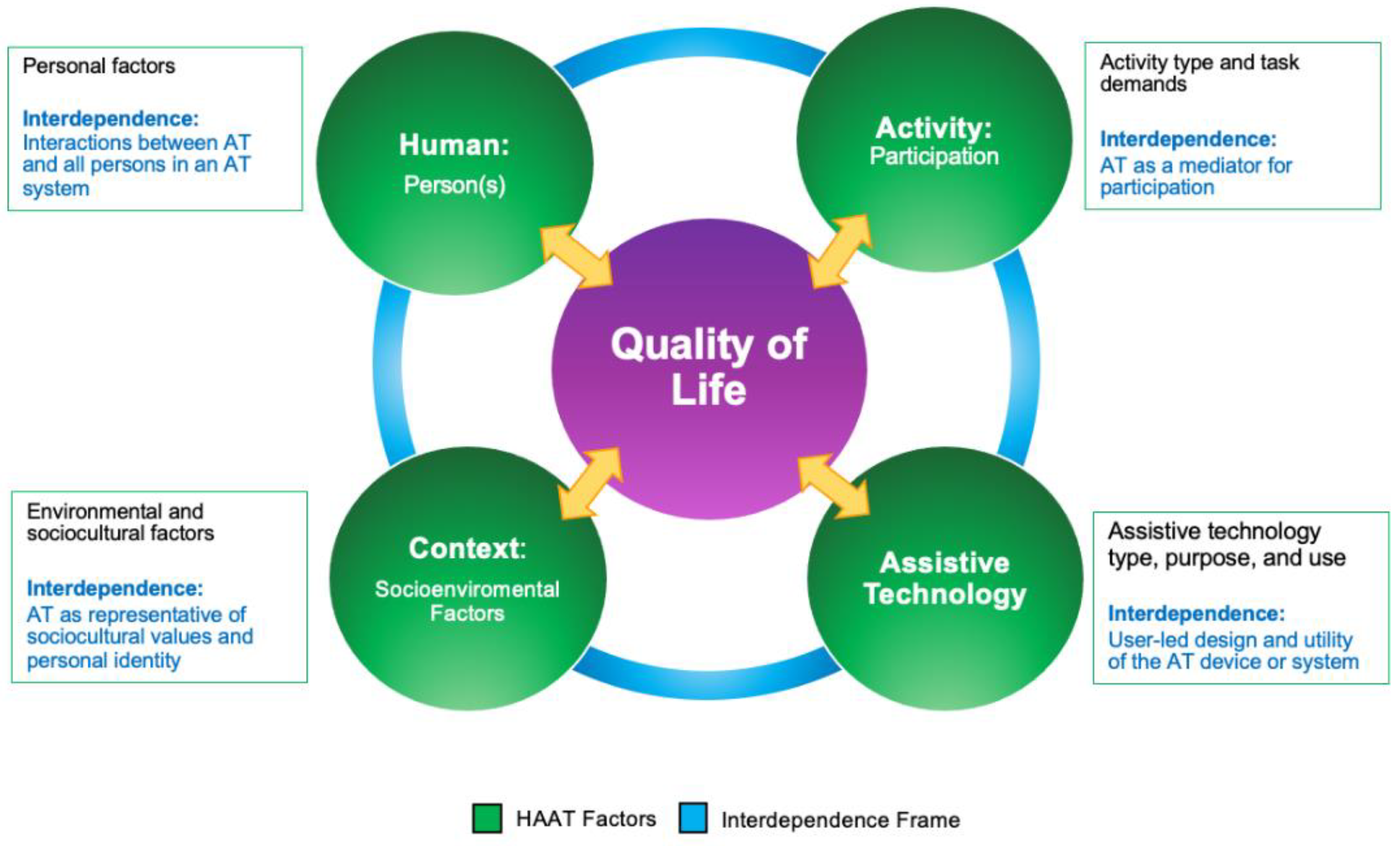
2.2. Interdependence-Human Activity Assistive Technology (iHAAT) Framework
3. Results
3.1. F-Words for Child Development
3.1.1. Functioning
3.1.2. Family
3.1.3. Fitness
3.1.4. Fun
3.1.5. Friends
3.1.6. Future
3.2. iHAAT Conceptual Framework
3.2.1. Human
3.2.2. Activity
3.2.3. Assistive Technology
3.2.4. Context
3.2.5. Well-Being
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child. Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmonson, M.; Galea, C.; Hines, A.; Langdon, K.; McNamara, M.; Paton, M.C.B.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brenna, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child. Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P. Cerebral palsy: What parents and doctors want to know. Bmj 2003, 326, 970–974. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1125882/pdf/970.pdf (accessed on 19 May 2024). [CrossRef] [PubMed]
- Bailes, A.F.; Greve, K.; Long, J.; Kurowski, B.G.; Vargus-Adams, J.; Aronow, B.; Mitelpunkt, A. Describing the Delivery of Evidence-Based Physical Therapy Intervention to Individuals with Cerebral Palsy. Pediatr. Phys. Ther. 2021, 33, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Hollung, S.J.; Hägglund, G.; Gaston, M.S.; Seid, A.K.; Lydersen, S.; Alriksson-Schmidt, A.I.; Andersen, G.L. Point prevalence and motor function of children and adolescents with cerebral palsy in Scandinavia and Scotland: A CP-North study. Dev. Med. Child. Neurol. 2021, 63, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.M.; Carlin, J.B.; Reddihough, D.S. Using the Gross Motor Function Classification System to describe patterns of motor severity in cerebral palsy. Dev. Med. Child. Neurol. 2011, 53, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, S.; Badawi, N.; Balde, I.; Goldsmith, S.; Karlsson, P.; Novak, I.; Ostojik, K.; Smithers-Sheedy, H.; Waight, E.; Murray, N.; et al. Australian Cerebral Palsy Register Report. 2018. Available online: https://cpregister.com/wp-content/uploads/2019/02/Report-of-the-Australian-Cerebral-Palsy-Register-Birth-Years-1995-2012.pdf (accessed on 20 January 2024).
- Bartlett, D.; Hanna, S.; Avery, L.; Stevenson, R.; Galuppi, B. Correlates of decline in gross motor capacity in adolescents with cerebral palsy in Gross Motor Function Classification System levels III to V: An exploratory study. Dev. Med. Child. Neurol. 2010, 52, e155–e160. [Google Scholar] [CrossRef] [PubMed]
- Bolton, M.; Donohoe, M. Ambulatory assistive devices for children and youth with cerebral palsy. In Cerebral Palsy; Miller, F., Bachrach, S.J., Lennon, N., O’Neil, M.E., Eds.; Springer Nature: Berlin/Heidelberg, Germany, 2020; pp. 2963–2975. [Google Scholar] [CrossRef]
- Maitre, N.L.; Chorna, O.; Romeo, D.M.; Guzzetta, A. A High-Risk Infant Follow-Up Program. Pediatr. Neurol. 2016, 65, 31–38. [Google Scholar] [CrossRef]
- Einspieler, C.; Bos, A.F.; Krieber-Tomantschger, M.; Alvarado, E.; Barbosa, V.M.; Bertoncelli, N.; Burger, M.; Chorna, O.; Del Secco, S.; DeRegnier, R.A.; et al. Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. J. Clin. Med. 2019, 8, 1616. [Google Scholar] [CrossRef]
- Einspieler, C.; Marschik, P.B.; Pansy, J.; Scheuchenegger, A.; Krieber, M.; Yang, H.; Kornacka, M.K.; Rowinska, E.; Soloveichik, M.; Bos, A.F. The general movement optimality score: A detailed assessment of general movements during preterm and term age. Dev. Med. Child. Neurol. 2016, 58, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Ricci, D.; Brogna, C.; Mercuri, E. Use of the Hammersmith Infant Neurological Examination in infants with cerebral palsy: A critical review of the literature. Dev. Med. Child. Neurol. 2016, 58, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Rodby-Bousquet, E.; Hägglund, G. Sitting and standing performance in a total population of children with cerebral palsy: A cross-sectional study. BMC Musculoskelet. Disord. 2010, 11, 131. [Google Scholar] [CrossRef]
- Wright, F.V.; Belbin, G.; Slack, M.; Jutai, J. An evaluation of the David Hart Walker Orthosis: A new assistive device for children with Cerebral Palsy. Physiother. Can. 1999, 51, 280–291. [Google Scholar]
- Eisenberg, S.; Zuk, L.; Carmeli, E.; Katz-Leurer, M. Contribution of stepping while standing to function and secondary conditions among children with cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Feldner, H.; Tucker, J.; Logan, S.W.; Galloway, J.C. ON Time Mobility: Advocating for Mobility Equity. Pediatr. Phys. Ther. 2022, 34, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Kretch, K.S.; Franchak, J.M.; Adolph, K.E. Crawling and walking infants see the world differently. Child. Dev. 2014, 85, 1503–1518. [Google Scholar] [CrossRef] [PubMed]
- Kermoian, R.; Campos, J.J. Locomotor experience: A facilitator of spatial cognitive development. Child. Dev. 1988, 59, 908–917. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3168629 (accessed on 19 May 2024). [CrossRef] [PubMed]
- McLean, L.; Paleg, G.; Livingstone, R. Supported-standing interventions for children and young adults with non-ambulant cerebral palsy: A scoping review. Dev. Med. Child. Neurol. 2023, 65, 754–772. [Google Scholar] [CrossRef]
- Livingstone, R.W.; Paleg, G.S. Use of overground supported-stepping devices for non-ambulant children, adolescents, and adults with cerebral palsy: A scoping review. Disabilities 2023, 3, 165–195. [Google Scholar] [CrossRef]
- Livingstone, R.; Paleg, G. Practice considerations for the introduction and use of power mobility for children. Dev. Med. Child. Neurol. 2014, 56, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Willerslev-Olsen, M.; Choe Lund, M.; Lorentzen, J.; Barber, L.; Kofoed-Hansen, M.; Nielsen, J.B. Impaired muscle growth precedes development of increased stiffness of the triceps surae musculotendinous unit in children with cerebral palsy. Dev. Med. Child. Neurol. 2018, 60, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Herskind, A.; Ritterband-Rosenbaum, A.; Willerslev-Olsen, M.; Lorentzen, J.; Hanson, L.; Lichtwark, G.; Nielsen, J.B. Muscle growth is reduced in 15-month-old children with cerebral palsy. Dev. Med. Child. Neurol. 2016, 58, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Shortland, A. Muscle deficits in cerebral palsy and early loss of mobility: Can we learn something from our elders? Dev. Med. Child. Neurol. 2009, 51 (Suppl. S4), 59–63. [Google Scholar] [CrossRef] [PubMed]
- Verschuren, O.; Smorenburg, A.R.P.; Luiking, Y.; Bell, K.; Barber, L.; Peterson, M.D. Determinants of muscle preservation in individuals with cerebral palsy across the lifespan: A narrative review of the literature. J. Cachexia Sarcopenia Muscle 2018, 9, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Handsfield, G.G.; Williams, S.; Khuu, S.; Lichtwark, G.; Stott, N.S. Muscle architecture, growth, and biological Remodelling in cerebral palsy: A narrative review. BMC Musculoskelet. Disord. 2022, 23, 233. [Google Scholar] [CrossRef] [PubMed]
- Ganz, F.; Hammam, N.; Pritchard, L. Sedentary behavior and children with physical disabilities: A scoping review. Disabil. Rehabil. 2021, 43, 2963–2975. [Google Scholar] [CrossRef] [PubMed]
- Handsfield, G.G.; Meyer, C.H.; Abel, M.F.; Blemker, S.S. Heterogeneity of muscle sizes in the lower limbs of children with cerebral palsy. Muscle Nerve 2016, 53, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.L.; Pitcher, C.A.; Williams, S.A.; Likari, M.K.; Valentine, J.P.; Shipman, P.J.; Elliott, C.M. Does muscle size matter? the relationship between muscle size and strength in children with cerebral palsy. Disabil. Rehabil. 2015, 37, 579–584. [Google Scholar] [CrossRef]
- Pitcher, C.A.; Elliott, C.M.; Valentine, J.P.; Stannage, K.; Williams, S.A.; Shipman, P.J.; Reid, S.L. Muscle morphology of the lower leg in ambulant children with spastic cerebral palsy. Muscle Nerve 2018, 58, 818–823. [Google Scholar] [CrossRef]
- Johnson, D.L.; Miller, F.; Subramanian, P.; Modlesky, C.M. Adipose Tissue Infiltration of Skeletal Muscle in Children with Cerebral Palsy. J. Pediatr. 2009, 154, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.J.; Charles-Edwards, G.D.; Keevil, S.F.; Lewis, A.P.; Gough, M.; Shortland, A.P. Intramuscular fat in ambulant young adults with bilateral spastic cerebral palsy. BMC Musculoskelet. Disord. 2014, 15, 236. [Google Scholar] [CrossRef] [PubMed]
- Marbini, A.; Ferrari, A.; Cioni, G.; Bellanova, M.F.; Fusco, C.; Gemignani, F. Immunohistochemical study of muscle biopsy in children with cerebral palsy. Brain Dev. 2002, 24, 63–66. [Google Scholar] [CrossRef]
- Smith, L.R.; Lee, K.S.; Ward, S.R.; Chambers, H.G.; Lieber, R.L. Hamstring contractures in children with spastic cerebral palsy result from a stiffer extracellular matrix and increased in vivo sarcomere length. J. Physiol. 2011, 589, 2625–2639. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.; Haskell, W.; Gamble, J.; Hamilton, R.; Brown, D.; Rinsky, L. Muscle pathology and clinical measures of disability in children with cerebral palsy. J. Orthop. Res. 1994, 12, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Massaad, A.; Assi, A.; Bakouny, Z.; Bizdikian, A.J.; Skalli, W.; Ghanem, I. Alterations of treatment-naïve pelvis and thigh muscle morphology in children with cerebral palsy. J. Biomech. 2019, 82, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Gordon, P.M.; Hurvitz, E.A. Chronic disease risk among adults with cerebral palsy: The role of premature sarcopoenia, obesity and sedentary behaviour. Obes. Rev. 2013, 14, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Won, J.H.; Jung, S.H. Bone Mineral Density in Adults with Cerebral Palsy. Front. Neurol. 2021, 12, 733322. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.H.; Dennison, E.M.; Aihie Sayer, A.; Fielding, R.; Cooper, C. Osteoporosis and sarcopenia in older age. Bone 2015, 80, 126–130. [Google Scholar] [CrossRef]
- Lee, F.; Balcazar, F.; Hsieh, K.; Sposato Bonfiglio, B.; Parker Harris, S.; Feldner, H.A. Factors impacting community living outcomes among former long-term nursing home residents using the interdependence-Human Activity Assistive Technology (iHAAT) model. Assist. Technol. 2024, 1–10. [Google Scholar] [CrossRef]
- Becker, S.J.; DeClemente-Bosco, K.; Scott, K.; Helseth, S.A.; Patel-Syed, Z.; Li, D.H. The “D&I Bridge”: Introducing a teaching tool to define the D, the I, and the why. Implement. Sci. Comm. 2024, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Paleg, G.; Livingstone, R. Evidence-informed clinical perspectives on postural management for hip health in children and adults with non-ambulant cerebral palsy. J. Pediatr. Rehabil. Med. 2022, 15, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Gorter, J.W. The “F-words” in childhood disability: I swear this is how we should think! Child. Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]
- Lee, F.N.; Feldner, H.A.; Hsieh, K.; Balcazar, F.; Bonfiglio, B.S.; Parker, S. The interdependence-Human Activity Assistive Technology Model (i-HAAT): A contemporary conceptual approach to assistive technology outcomes research. In Proceedings of the RESNA Annual Conference 2022, Washington, DC, USA (Online), 13–15 July 2022; Available online: https://www.resna.org/sites/default/files/conference/2022/ServiceDeliveryandOutcomes/85_Lee/85_Lee.pdf (accessed on 20 January 2024).
- McLean, L.; Paleg, G.; Livingstone, R. Stand up for participation and function. In Proceedings of the 38th International Seating Symposium, Pittsburgh, PA, USA, 13–15 April 2023. [Google Scholar] [CrossRef]
- Paleg, G.; Livingstone, R. Standing and stepping for participation and engagement with non-ambulant cerebral palsy. In Proceedings of the Nordic Seating Symposium 2023, Stockholm, Sweden (Online), 8–10 February 2023. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Bradbury, M.; Bennison, E.; Mason, H.; Gregory, J. Tools for participation: Living aids and the F-words for childhood development. Paediatr. Child Health 2021, 31, 352–358. [Google Scholar] [CrossRef]
- de Campos, A.C.; Hidalgo Robles, A.; Longo, E.; Shrader, C.; Paleg, G. Scoping review of early interventions for young children classified as Gross Motor Function Classification System (GMFCS) IV and V. Dev. Med. Child. Neurol. 2024, 66, 41–51. [Google Scholar] [PubMed]
- Longo, E.; Monteiro, R.; Hidalgo-Robles, A.; Paleg, G.; Shrader, C.; de Campos, A.C. Intervention ingredients and F-words in early intervention for children with cerebral palsy functioning at GMFCS IV and V: A scoping review protocol. Front. Rehabil. Sci. 2023, 4, 1110552. [Google Scholar] [CrossRef] [PubMed]
- Giesbrecht, E. Application of the Human Activity Assistive Technology model for occupational therapy research. Aust. Occup. Ther. J. 2013, 60, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.L.; Brady, E.; Branham, S.M. Interdependence as a frame for assistive technology research and design. In Proceedings of the 20th International ACM SIGACCESS Conference on Computers and Accessibility, Galway, Ireland, 22–24 October 2018; pp. 161–173. [Google Scholar] [CrossRef]
- White, G.W.; Simpson, J.L.; Gonda, C.; Ravesloot, C.; Coble, Z. Moving from independence to interdependence: A conceptual model for better understanding community participation of centers for independent living consumers. J. Disabil. Policy Stud. 2010, 20, 233–240. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. User Guide. McGill. 2018, pp. 1–11. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 20 January 2024).
- Paananen, L. Ihastuttaako Vai Vihastuttaako? Kävelyn Apuvälineeseen. Master’s Thesis, Jamk University of Applied Sciences, Jyväskylä, Finland, 2009. Available online: https://www.theseus.fi/bitstream/handle/10024/6662/Paananen_Laila.pdf?sequence=1&isAllowed=y (accessed on 20 January 2024).
- Rosenbaum, P. To enhance function, promote children’s development. Dev. Med. Child. Neurol. 2021, 63, 628. [Google Scholar] [CrossRef]
- Gibson, S.K.; Sprod, J.A.; Maher, C.A. The use of standing frames for contracture management for nonmobile children with cerebral palsy. Int. J. Rehabil. Res. 2009, 32, 316–323. [Google Scholar] [CrossRef]
- Audu, O.; Daly, C. Standing activity intervention and motor function in a young child with cerebral palsy: A case report. Physiother. Theory Pract. 2017, 33, 162–172. [Google Scholar] [CrossRef] [PubMed]
- George, F.K. The importance of static and dynamic posture: How making static equipment dynamic may improve movement and function of children with neurological impairment—A retrospective service evaluation. Assoc. Paediatr. Chart. Physiother. J. 2018, 9, 56–62. [Google Scholar]
- Sharma, M.; Bajracharya, S. Low cost modified reverse walker to assist children with cerebral palsy. RGUHS J. Allied Health Sci. 2021, 1, 18–24. Available online: https://journalgrid.com/view/article/rjahs/37 (accessed on 20 January 2024).
- Wright, F.V.; Jutai, J.W. Evaluation of the longer-term use of the David Hart Walker Orthosis by children with cerebral palsy: A 3-year prospective evaluation. Disabil. Rehabil. Assist. Technol. 2006, 1, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Martín Gómez, M.; Laguna-Mena, C.; Martín-Maroto, M.; Echevarria-Ulloa, M.; Dumitrescu, A.; Arroyo-Riaño, M. Evaluation and follow-up of NF-Walker technical aid during the transition to adult life. Dev. Med. Child. Neurol. 2021, 63 (Suppl. S2), 42. [Google Scholar] [CrossRef]
- McKeever, P.; Rossen, B.E.; Scott, H.; Robinson-Vincent, K.; Wright, V. The significance of uprightness: Parents’ reflections on children’s responses to a hands-free walker for children. Disabil. Soc. 2013, 28, 380–392. [Google Scholar] [CrossRef]
- Capati, V.; Covert, S.Y.; Paleg, G. Stander use for an adolescent with cerebral palsy at GMFCS level V with hip and knee contractures. Assist. Technol. 2020, 32, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Rivi, E.; Filippi, M.; Fornasari, E.; Mascia, M.T.; Ferrari, A.; Costi, S. Effectiveness of standing frame on constipation in children with cerebral palsy: A single-subject study. Occup. Ther. Int. 2014, 21, 115–123. [Google Scholar] [CrossRef]
- Caulton, J.M. A randomised controlled trial of standing programme on bone mineral density in non-ambulant children with cerebral palsy. Arch. Dis. Child. 2004, 89, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Han, E.Y.; Choi, J.H.; Kim, S.H.; Im, S.H. The effect of weight bearing on bone mineral density and bone growth in children with cerebral palsy. Medicine 2017, 96, 16–19. [Google Scholar] [CrossRef]
- Shin, M.J.; Shin, Y.B.; Ko, H.-Y.; Sohn, H.J.; Chang, J.H.; Kim, S.Y.; Kim, S.N.; Kim, W.; Kim, I.N. Effect on the bone mineral density according to weight-bearing exercise in children with spastic quadriplegic cerebral palsy: A preliminary study. Ann. Rehabil. Med. 2010, 34, 622–627. [Google Scholar]
- Rodríguez-Costa, I.; De la Cruz-López, I.; Fernández-Zárate, I.; Maldonado-Bascón, S.; Lafuente-Arroyo, S.; Nunez-Nagy, S. Benefits of a low-cost walking device in children with cerebral palsy: A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 2808. [Google Scholar] [CrossRef]
- Israeli-Mendlovic, H.; Mendlovic, J.; Katz-Leurer, M. Heart rate and heart rate variability parameters at rest, during activity and passive standing among children with cerebral palsy GMFCS IV-V. Dev. Neurorehabil. 2014, 17, 398–402. [Google Scholar] [CrossRef]
- Verschuren, O.; Peterson, M.D.; Leferink, S.; Darrah, J. Muscle activation and energy-requirements for varying postures in children and adolescents with cerebral palsy. J. Pediatr. 2014, 165, 1011–1016. [Google Scholar] [CrossRef]
- Verschuren, O.; Hulst, R.Y.; Voorman, J.; Pillen, S.; Luitwieler, N.; Dudink, J.; Gorter, J.W. 24-Hour activity for children with cerebral palsy: A clinical practice guide. Dev. Med. Child. Neurol. 2020, 63, 54–59. [Google Scholar] [CrossRef]
- Smati, S.; Pouliot-Laforte, A.; Chevalier, M.; Lemay, M.; Ballaz, L. Effect of power training on locomotion capacities in children with cerebral palsy with GMFCS level III–IV. Disabil. Rehabil. 2022, 45, 2329–2335. [Google Scholar] [CrossRef]
- Gannotti, M.E.; Liquori, B.M.; Thorpe, D.E.; Fuchs, R.K. Designing Exercise to Improve Bone Health among Individuals with Cerebral Palsy. Pediatr. Phys. Ther. 2021, 33, 50–56. [Google Scholar] [CrossRef]
- Rapson, R.; King, T.; Morris, C.; Jefferey, R.; Mellhuish, J.; Stephens, C.; Marsden, J. Effect of different durations of using a standing frame on the rate of hip migration in children with moderate to severe cerebral palsy: A feasibility study for a randomised controlled trial. Physiotherapy 2022, 116, 42–49. [Google Scholar] [CrossRef]
- Wright-Ott, C. Mobility Matters-Imbedding Hands-Free Locomotion Experiences into the Preschool and Elementary Curricula for Students with Severe Speech and Motor Impairment: The Bridge School Experience. Bridge School Curriculum. 2018. Available online: https://curriculum.bridgeschool.org/wp-content/uploads/sites/5/2018/06/mobility_matters.pdf (accessed on 27 January 2023).
- Goodwin, J.; Lecouturier, J.; Basu, A.; Colver, A.; Crombie, S.; Smith, J.; Howel, S.; McColl, E.; Parr, J.R.; Kolehmainen, N.; et al. Standing frames for children with cerebral palsy: A mixed-methods feasibility study. Health Technol. Assess. 2018, 22, 1–231. [Google Scholar] [CrossRef]
- Hughes, S.; Campbell, L. Children with cerebral palsy: Perspectives and experiences of using standing frames. Assoc. Paediatr. Chart. Physiother. J. 2014, 5, 30–37. [Google Scholar]
- Paleg, G.; Alitizer, W.; Malone, R.; Ballard, K.; Kreger, A. Inclination, hip abduction, orientation, and tone affect weight-bearing in pediatric standing devices. J. Pediatr. Rehabil. Med. 2021, 14, 433–441. [Google Scholar]
- Herman, D.; May, R.; Vogel, L.; Johnson, J.; Henderson, R.C. Quantifying weight-bearing by children with cerebral palsy while in passive standers. Pediatr. Phys. Ther. 2007, 19, 283–287. [Google Scholar] [CrossRef]
- Kecskemethy, H.H.; Herman, D.; May, R.; Paul, K.; Bachrach, S.J.; Henderson, R.C. Quantifying weight bearing while in passive standers and a comparison of standers. Dev. Med. Child. Neurol. 2008, 50, 520–523. [Google Scholar] [CrossRef]
- Broadbent, J.; Woollam, P.J.; Major, R.E.; Stallard, J. Technical note: A rear support walking frame for severely disabled children with cerebral palsy: Initial development. Prosthet. Orthot. Int. 2000, 24, 233–240. [Google Scholar] [CrossRef]
- Paleg, G.; Huang, M.; Vasquez Gabela, S.C.; Sprigle, S.; Livingstone, R. Comparison of the Inertial Properties and Forces Required to Initiate Movement for Three Gait Trainers. Assist. Technol. 2016, 28, 137–143. [Google Scholar] [CrossRef]
- Cowan, R.; Davis, S. Physiotherapist opinions of barriers and facilitators that affect primary caregiver engagement with the use of standing frames for children with cerebral palsy: A qualitative study. Assoc. Paediatr. Chart. Physiother. J. 2018, 9, 27–37. [Google Scholar]
- Goodwin, J.; Colver, A.; Basu, A.; Crombie, S.; Howel, D.; Parr, J.R.; McColl, E.; Kolehmainen, N.; Roberts, A.; Lecouturier, J.; et al. Understanding frames: A UK survey of parents and professionals regarding the use of standing frames for children with cerebral palsy. Child. Care Health Dev. 2018, 44, 195–202. [Google Scholar] [CrossRef]
- Goodwin, J.; Lecouturier, J.; Smith, J.; Crombie, S.; Basu, A.; Parr, J.R.; Howel, D.; McColl, E.; Roberts, A.; Miller, K.; et al. Understanding frames: A qualitative exploration of standing frame use for young people with cerebral palsy in educational settings. Child. Care Health Dev. 2019, 45, 433–439. [Google Scholar] [CrossRef]
- Bush, S.; Biggs, R. Assisted standing: Experiences of children with cerebral palsy and their physiotherapists. Assoc. Paediatr. Chart. Physiother. J. 2011, 2, 3–10. [Google Scholar]
- Daniels, N.; Gopskill, C.; Armstrong, J.; Pinnington, L.; Ward, C. An evaluation of standing frames designed for children: Preferences of users and therapists. Assoc. Paediatr. Chart. Physiother. J. 2005, 12–17. [Google Scholar]
- Taylor, K. Factors affecting prescription and implementation of standing-frame programs by school-based physical therapists for children with impaired mobility. Pediatr. Phys. Ther. 2009, 21, 282–288. [Google Scholar] [CrossRef]
- George, C.; Levin, W.; Ryan, J.M. The use and perception of support walkers for children with disabilities: A United Kingdom survey. BMC Pediatr. 2020, 20, 528. [Google Scholar] [CrossRef]
- Hornby, T.G.; Reisman, D.S.; Ward, I.G.; Scheets, P.L.; Miller, A.; Haddad, D.; Fox, E.J.; Fritz, N.E.; Hawkins, K.; Henderson, C.E.; et al. Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury. J. Neurol. Phys. Therap. 2020, 44, 49–100. [Google Scholar] [CrossRef]
- Valentín-Gudiol, M.; Mattern-Baxter, K.; Girabent-Farrés, M.; Bagur-Calafat, C.; Hadders-Algra, M.; Angulo-Barroso, R.M. Treadmill interventions in children under six years of age at risk of neuromotor delay. Cochrane Database Syst. Rev. 2017, CD009242. [Google Scholar] [CrossRef]
- Pool, D.; Valentine, J.; Taylor, N.F.; Bear, N.; Elliott, C. Locomotor and robotic assistive gait training for children with cerebral palsy. Dev. Med. Child. Neurol. 2021, 63, 328–335. [Google Scholar] [CrossRef]
- Willoughby, K.L.; Dodd, K.J.; Shields, N.; Foley, S. Efficacy of partial body weight-supported treadmill training compared with overground walking practice for children with cerebral palsy: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 333–339. [Google Scholar] [CrossRef]
- Rosen, L.; Plummer, T.; Sabet, A.; Lange, M.L.; Livingstone, R. RESNA position on the application of power mobility devices for pediatric users. Assist. Technol. 2023, 35, 14–22. [Google Scholar] [CrossRef]
- Huang, H.; Chen, C. The use of modified ride-on cars to maximize mobility and improve socialization-a group design. Res. Dev. Disabil. 2017, 61, 172–180. [Google Scholar] [CrossRef]
- Berry, E.; McLaurin, S.; Sparling, J. Parent/caregiver perspectives on the use of power wheelchairs. Pediatr. Phys. Ther. 1996, 8, 146–150. [Google Scholar] [CrossRef]
- Livingstone, R.; Bone, J.; Field, D. Beginning Power Mobility: An exploration of factors associated with child use of early power mobility devices and parent device preference. J. Rehabil. Assist. Technol. Eng. 2020, 7, 1–12. [Google Scholar] [CrossRef]
- Feldner, H.A.; Logan, S.W.; Galloway, J.C. Why the time is right for a radical paradigm shift in early powered mobility: The role of powered mobility technology devices, policy and stakeholders. Disabil. Rehabil. Assist. Technol. 2016, 11, 89–102. [Google Scholar] [CrossRef]
- Plummer, T.; Logan, S.W.; Morress, C. Explorer Mini: Infants’ Initial Experience with a Novel Pediatric Powered Mobility Device. Phys. Occup. Ther. Pediatr. 2020, 41, 192–208. [Google Scholar] [CrossRef]
- Butler, C. Effects of powered mobility on self-initiated behaviors of very young children with locomotor disability. Dev. Med. Child. Neurol. 1986, 28, 325–332. [Google Scholar] [CrossRef]
- Kuenzle, C.; Brunner, R. The effects of the Norsk Funktion-walking orthosis on the walking ability of children with cerebal palsy and severe gait impairment. J. Prosthet. Orthot. 2009, 21, 138–144. [Google Scholar] [CrossRef]
- Casey, J.; Rosenblad, A.; Rodby-Bousquet, E. Postural asymmetries, pain, and ability to change position of children with cerebral palsy in sitting and supine: A cross-sectional study. Disabil. Rehabil. 2022, 44, 2363–2371. [Google Scholar] [CrossRef]
- Livingstone, R.W.; Chin, A.J.; Paleg, G.S. Power Mobility, Supported Standing and Stepping Device Use in the First Two Years of Life: A Case Report of Twins Functioning at GMFCS V. Disabilities 2023, 3, 507–524. [Google Scholar] [CrossRef]
- Livingstone, R.W.; Paleg, G.S.; Field, D.A. Supported standing and stepping device use in young children with cerebral palsy, Gross Motor Function Classification System III, IV and V: A descriptive study. Assist. Technol. 2023, 1–11. [Google Scholar] [CrossRef]
- Logan, S.W.; Catena, M.A.; Sabet, A.; Hospodar, C.M.; Yohn, H.; Govindan, A.; Galloway, J.C. Standing Tall: Feasibility of a Modified Ride-On Car That Encourages Standing. Pediatr. Phys. Ther. 2019, 31, E6–E13. [Google Scholar] [CrossRef]
- Huang, H.H.; Hsieh, Y.H.; Chang, C.H.; Tsai, W.Y.; Huang, C.K.; Chen, C.L. Ride-on car training using sitting and standing postures for mobility and socialization in young children with motor delays: A randomized controlled trial. Disabil. Rehabil. 2023, 45, 1453–1460. [Google Scholar] [CrossRef]
- Huang, H.H.; Chu, Y.-W.; Chan, Y.-T.; Chen, C.-L. A pilot randomised controlled trial of ride-on cars and postural combinations of standing and sitting for mobility and social function in toddlers with motor delays. Disabil. Rehabil. Assist. Technol. 2024. [Google Scholar] [CrossRef]
- Macias-Merlo, L.; Bagur-Calafat, C.; Girabent-Farrés, M.; Stuberg, W.A. Effects of the standing program with hip abduction on hip acetabular development in children with spastic diplegia cerebral palsy. Disabil. Rehabil. 2016, 38, 1075–1081. [Google Scholar] [CrossRef]
- Macias-Merlo, L.; Bagur-Calafat, C.; Girabent-Farrés, M.; Stuberg, W.A. Standing programs to promote hip flexibility in children with spastic diplegic cerebral palsy. Pediatr. Phys. Ther. 2015, 27, 243–249. [Google Scholar] [CrossRef]
- Barton, C.; Buckley, J.; Samia, P.; Williams, F.; Taylor, S.R.; Lindoewood, R. The efficacy of appropriate paper-based technology for Kenyan children with cerebral palsy. Disabil. Rehabil. Assist. Technol. 2022, 17, 927–937. [Google Scholar] [CrossRef]
- Walle, E.A. Infant social development across the transition from crawling to walking. Front. Psychol. 2016, 7, 960. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paleg, G.S.; Williams, S.A.; Livingstone, R.W. Supported Standing and Supported Stepping Devices for Children with Non-Ambulant Cerebral Palsy: An Interdependence and F-Words Focus. Int. J. Environ. Res. Public Health 2024, 21, 669. https://doi.org/10.3390/ijerph21060669
Paleg GS, Williams SA, Livingstone RW. Supported Standing and Supported Stepping Devices for Children with Non-Ambulant Cerebral Palsy: An Interdependence and F-Words Focus. International Journal of Environmental Research and Public Health. 2024; 21(6):669. https://doi.org/10.3390/ijerph21060669
Chicago/Turabian StylePaleg, Ginny S., Sian A. Williams, and Roslyn W. Livingstone. 2024. "Supported Standing and Supported Stepping Devices for Children with Non-Ambulant Cerebral Palsy: An Interdependence and F-Words Focus" International Journal of Environmental Research and Public Health 21, no. 6: 669. https://doi.org/10.3390/ijerph21060669
APA StylePaleg, G. S., Williams, S. A., & Livingstone, R. W. (2024). Supported Standing and Supported Stepping Devices for Children with Non-Ambulant Cerebral Palsy: An Interdependence and F-Words Focus. International Journal of Environmental Research and Public Health, 21(6), 669. https://doi.org/10.3390/ijerph21060669