
Patient Perspectives on Portal-Based Anxiety and Depression Screening in HIV Care: A Qualitative Study Using the Consolidated Framework for Implementation Research
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Sample
2.4. Data Collection
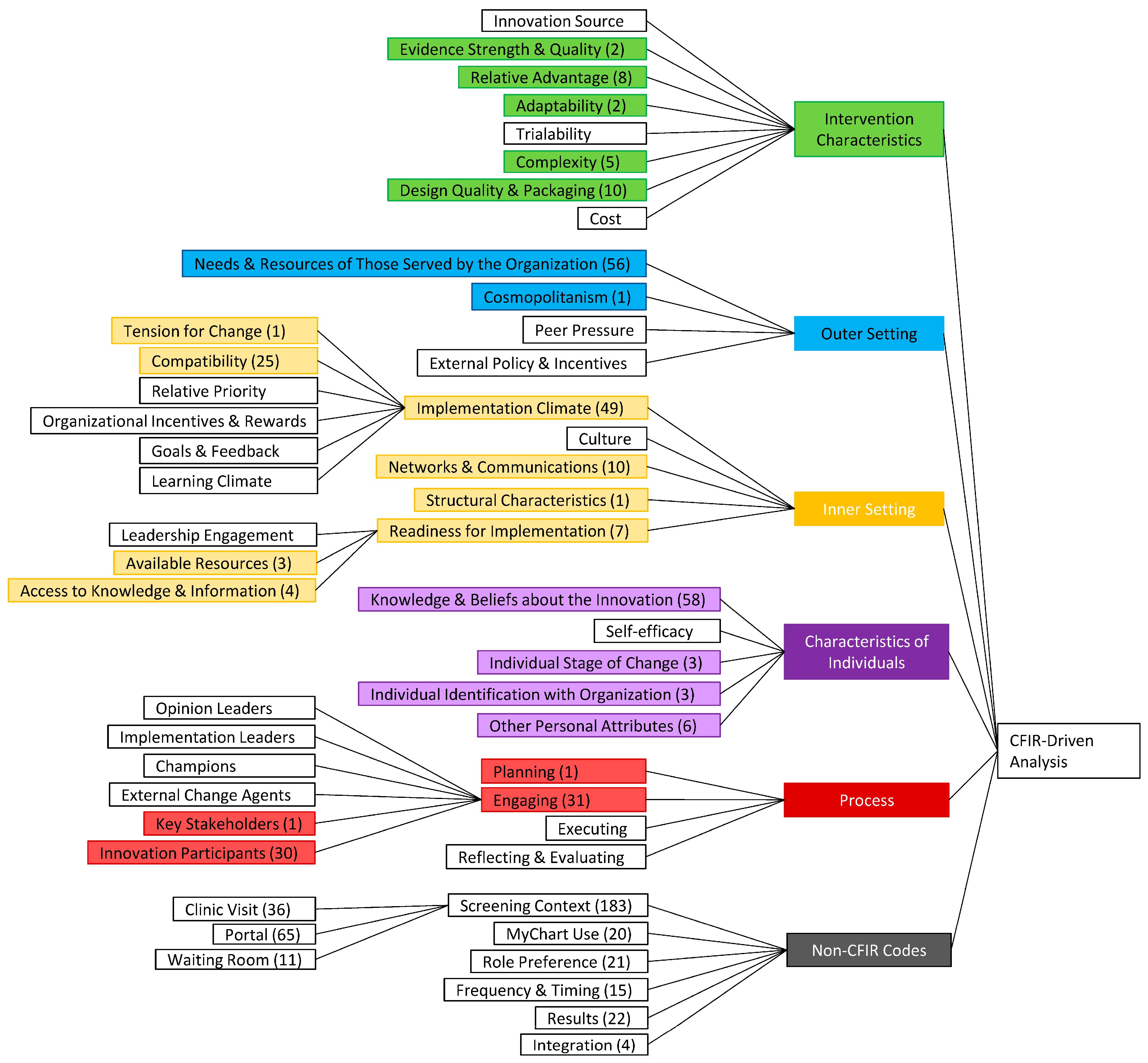
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Thematic Analysis
3.2.1. Intervention Characteristics
Facilitator: Absence of Alternative Anxiety and Depression Screening Methods
“I hid my anxiety for a long time. I was ashamed, I was afraid of talking about it. I was dealing on my own and I think somebody actually in my circle, my friends circle told me that I should look for help. And it was not easy to open up to a doctor, so if I were to do it through the chart and know that I’m going to get the right help, it will probably be a lot easier for me to do so”.Participant 1 (52 year-old male)
Facilitator: Simple and Approachable Portal Design
Facilitator: Adaptability of Screening Frequency
“I think it’s just depending on the person. Because someone might need it more than other people. Somebody else might be more reserved. Someone else might just need to talk to people and might need that assistance”.Participant 3 (41-year-old male) on preferred frequency of screening
3.2.2. Outer Setting
Barrier: Fears of Mental Health Stigmatization from the Health Care System
“…the scheduler, the person taking vitals, confirming your medication, all of that, right? I’m really not warm and fuzzy about that being who notifies you”.Participant 5 (34-year-old male)
3.2.3. Inner Setting
Facilitator: Anxiety and Depression Screening Is Highly Compatible with Routine HIV Care
“I look at the mental health care and the ID healthcare as being interlinked in the sense that better mental health care would seem like it would result in better outcomes for an ID patient and vice versa, more of that holistic approach to health and making sure that someone who is an ID clinic and does need access to mental health care is able to get those services”.Participant 5 (34-year-old male)
Barrier: Lack of Technical Support for Patient Portal Users
“I don’t know what MyChart is really designed for. Somebody said it has my team on it but nobody has ever explained to me, what you could do with MyChart other than the results and your appointments will be on MyChart”.Participant 6 (36-year-old male)
Barrier: The Portal Is an Extraneous Means of Communication with the Care Team
“I believe onsite, hands-on, in-person talk with my doctor, so I can get the information that I need. [The portal] is a great asset for people who need to use it but, me, I don’t have time for it. I have to be in person”.Participant 7 (57-year-old male)
Barrier: The Utility of Portal-Based Screening Is Dependent on Care Team Responsiveness
“…If I type that in like, “Doctor, oh, I’m having anxiety and depression today.” Then, my letter should read high rate because there is a concern here. There is an emergency here. Then, have a quick answer. Have those tools in place, so they can address those issues. If you’re going to use [the portal] have the tools”.Participant 7 (57-year-old male)
“I’ve had the feeling where I needed to talk to my doctor, right away, and I’m not able to get through the phone service. So, I go on MyChart. I usually hear back from them maybe two or three days later and I don’t really think that’s sufficient. I could have been going through really, physical and mental breakdown and I really needed to talk to my doctor have her assure me that everything is going to be okay or come in for an emergency check-in just to ease my mind and see if my anxiety is more or if my depression is more”.Participant 4 (25-year-old female)
3.2.4. Characteristics of Individuals
Facilitator: Anxiety and Depression Screening Is an Important Part of Linkage to Anxiety and Depression Treatment
“I think that we should be aware of [anxiety and depression]. That it be known that it is an illness and you need to get help if you need it. Don’t be invasive about it. You know what I’m saying? Don’t be aggressive. But I think that it should be talked about. It should be... Do you know what I’m saying? It should be confronted.”Participant 8 (38-year-old male)
“Oh, I would definitely think [screening] would be needed and would be successful and would be an asset to the treatment because when you’re going through... When you’re going through things, it’s a lot. And some people are going through so much. That’s a lot that you deal with here in this world today. And if my doctor asked anything about anxiety or depression, I would definitely be open to that.”Participant 8 (38-year-old male)
Facilitator: Screening Questions May Increase Self-Awareness of Depression and Anxiety Symptoms
“So I like that way of asking because I think even if you for example, don’t have depression related insomnia, it can help that patients start to think about maybe changes that they are experiencing that do apply”.Participant 9 (34-year-old male)
“A lot of people, they wake up and you have mood swings, you got a moody day. You might go to sleep with an attitude, and you wake up with that attitude. Sometimes, it might be part of depression and you won’t even know that it’s depression”Participant 4 (25-year-old female)
3.2.5. Process
Facilitator: Bundling Anxiety and Depression Screening as Part of a Scheduled Visit
“You wouldn’t want to send an email for the appointment reminder and then a separate email for this, right? I mean, to me it doesn’t feel like a full thought. It seems disconnected like this group’s working over here and that group’s working over there and they don’t talk and they can’t work together so you get two emails, right?”Participant 9 (34-year-old male)
Facilitator: Communicating an Action Plan for Screening Results
“My only concern will be that I just want to get the accurate help. I just don’t want to be misdiagnosed through the chart as opposed to talking to someone at the clinic.”Participant 1 (52-year-old male)
4. Discussion
4.1. Proposed Implementation Strategies
4.1.1. Strategy 1: Promote Confidentiality
4.1.2. Strategy 2: Promote Individual Adaptability
4.1.3. Strategy 3: Emphasize Linkage to Mental Health Resources within Screening Messaging
4.1.4. Strategy 4: Bundle Anxiety and Depression Screening with Appointments
4.1.5. Strategy 5: Facilitate and Promote Timely Relay of Positive Screening Results to Providers
4.1.6. Strategy 6: Minimize Electronic Patient Portal Navigation Steps
4.1.7. Strategy 7: Provide Technical Support
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Remien, R.H.; Stirratt, M.J.; Nguyen, N.; Robbins, R.N.; Pala, A.N.; Mellins, C.A. Mental health and HIV/AIDS: The need for an integrated response. AIDS 2019, 33, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Ahmadi, S.; Rahmati, J.; Hosseinifard, H.; Dehnad, A.; Aryankhesal, A.; Shabaninejad, H.; Ghasemyani, S.; Alihosseini, S.; Bragazzi, N.L.; et al. Global prevalence of depression in HIV/AIDS: A systematic review and meta-analysis. BMJ Support. Palliat. Care 2019, 9, 404. [Google Scholar] [CrossRef] [PubMed]
- Brandt, C.; Zvolensky, M.J.; Woods, S.P.; Gonzalez, A.; Safren, S.A.; O’Cleirigh, C.M. Anxiety symptoms and disorders among adults living with HIV and AIDS: A critical review and integrative synthesis of the empirical literature. Clin. Psychol. Rev. 2017, 51, 164–184. [Google Scholar] [CrossRef] [PubMed]
- Rane, M.S.; Hong, T.; Govere, S.; Thulare, H.; Moosa, M.Y.; Celum, C.; Drain, P.K. Depression and Anxiety as Risk Factors for Delayed Care-Seeking Behavior in Human Immunodeficiency Virus-Infected Individuals in South Africa. Clin. Infect. Dis. 2018, 67, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Catz, S.L.; Heckman, T.G.; Kochman, A.; Dimarco, M. Rates and correlates of HIV treatment adherence among late middle-aged and older adults living with HIV disease. Psychol. Health Med. 2001, 6, 47–58. [Google Scholar] [CrossRef]
- van Servellen, G.; Chang, B.; Garcia, L.; Lombardi, E. Individual and system level factors associated with treatment nonadherence in human immunodeficiency virus-infected men and women. AIDS Patient Care STDS 2002, 16, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Mellins, C.A.; Havens, J.F.; McCaskill, E.O.; Leu, C.S.; Brudney, K.; Chesney, M.A. Mental health, substance use and disclosure are significantly associated with the medical treatment adherence of HIV-infected mothers. Psychol. Health Med. 2002, 7, 451–460. [Google Scholar] [CrossRef]
- Nilsson Schönnesson, L.; Diamond, P.M.; Ross, M.W.; Williams, M.; Bratt, G. Baseline predictors of three types of antiretroviral therapy (ART) adherence: A 2-year follow-up. AIDS Care 2006, 18, 407–414. [Google Scholar] [CrossRef]
- Roux, P.; Carrieri, M.P.; Michel, L.; Fugon, L.; Marcellin, F.; Obadia, Y.; Spire, B. Effect of anxiety symptoms on adherence to highly active antiretroviral therapy in HIV-infected women. J. Clin. Psychiatry 2009, 70, 1328–1329. [Google Scholar] [CrossRef]
- Kosiba, J.D.; Gonzalez, A.; O’Cleirigh, C.; Safren, S.A. Medication Adherence and HIV Symptom Distress in Relation to Panic Disorder Among HIV-Positive Adults Managing Opioid Dependence. Cogn. Ther. Res. 2014, 38, 458–464. [Google Scholar] [CrossRef]
- Pence, B.W.; Gaynes, B.N.; Adams, J.L.; Thielman, N.M.; Heine, A.D.; Mugavero, M.J.; McGuinness, T.; Raper, J.L.; Willig, J.H.; Shirey, K.G.; et al. The effect of antidepressant treatment on HIV and depression outcomes: Results from a randomized trial. AIDS 2015, 29, 1975–1986. [Google Scholar] [CrossRef] [PubMed]
- Samples, H.; Stuart, E.A.; Saloner, B.; Barry, C.L.; Mojtabai, R. The Role of Screening in Depression Diagnosis and Treatment in a Representative Sample of US Primary Care Visits. J. Gen. Intern. Med. 2020, 35, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Meeks, S. Screening Older Adults for Depression: Barriers Across Clinical Discipline Training. Innov. Aging 2019, 3, igz011. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.L.; Schmidt, S.; Lund, M.B.; Haynes, T.; Ford, D.; Egwuogu, H.; Schmitz, S.; McGregor, B.; Toomer, L.; Bussey-Jones, J. Improving Depression Screening in Underserved Populations in a Large Urban Academic Primary Care Center: A Provider-Centered Analysis and Approach. Am. J. Med. Qual. 2020, 35, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Pham, M.; Dillingham, R.; McManus, K.A. Expanded HIV Clinic-Based Mental Health Care Services: Association With Viral Suppression. Open Forum Infect. Dis. 2019, 6, ofz146. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.; Quinlivan, E.B.; Bess, K.; Gaynes, B.N.; Heine, A.; Zinski, A.; Modi, R.; Pence, B.W. Implementation of PHQ-9 depression screening for HIV-infected patients in a real-world setting. J. Assoc. Nurses AIDS Care 2014, 25, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Satre, D.D.; Anderson, A.N.; Leibowitz, A.S.; Levine-Hall, T.; Slome, S.; Flamm, J.; Hare, C.B.; McNeely, J.; Weisner, C.M.; Horberg, M.A.; et al. Implementing electronic substance use disorder and depression and anxiety screening and behavioral interventions in primary care clinics serving people with HIV: Protocol for the Promoting Access to Care Engagement (PACE) trial. Contemp. Clin. Trials 2019, 84, 105833. [Google Scholar] [CrossRef] [PubMed]
- Ryan White HIV/AIDS Program Funding. Available online: https://ryanwhite.hrsa.gov/about/budget (accessed on 6 April 2022).
- Byrne, J.M.; Elliott, S.; Firek, A. Initial experience with patient-clinician secure messaging at a VA medical center. J. Am. Med. Inf. Assoc. 2009, 16, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.D.; Liebovitz, D. It Takes Two to Tango: Engaging Patients and Providers with Portals. PM R 2017, 9, S85–S97. [Google Scholar] [CrossRef]
- Wright, A.; Feblowitz, J.; Samal, L.; McCoy, A.B.; Sittig, D.F. The Medicare Electronic Health Record Incentive Program: Provider performance on core and menu measures. Health Serv. Res. 2014, 49, 325–346. [Google Scholar] [CrossRef]
- Heisey-Grove, D.; Pately, V. ONC Data Brief: Ant, Certified, and Basic: Quantifying Physician EHR Adoption through 2014; The Office of the National Coordinator for Health Information Technology: Washington, DC, USA, 2014; pp. 1–10.
- Pecina, J.; North, F.; Williams, M.D.; Angstman, K.B. Use of an on-line patient portal in a depression collaborative care management program. J. Affect. Disord. 2017, 208, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dillingham, R.; Ingersoll, K.; Flickinger, T.E.; Waldman, A.L.; Grabowski, M.; Laurence, C.; Wispelwey, E.; Reynolds, G.; Conaway, M.; Cohn, W.F. PositiveLinks: A Mobile Health Intervention for Retention in HIV Care and Clinical Outcomes with 12-Month Follow-Up. AIDS Patient Care STDS 2018, 32, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Saberi, P.; Johnson, M.O. Correlation of Internet Use for Health Care Engagement Purposes and HIV Clinical Outcomes Among HIV-Positive Individuals Using Online Social Media. J. Health Commun. 2015, 20, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Nijland, N.; van Gemert-Pijnen, J.E.; Kelders, S.M.; Brandenburg, B.J.; Seydel, E.R. Factors influencing the use of a Web-based application for supporting the self-care of patients with type 2 diabetes: A longitudinal study. J. Med. Internet Res. 2011, 13, e71. [Google Scholar] [CrossRef] [PubMed]
- Nazi, K.M.; Hogan, T.P.; McInnes, D.K.; Woods, S.S.; Graham, G. Evaluating patient access to Electronic Health Records: Results from a survey of veterans. Med. Care 2013, 51, S52–S56. [Google Scholar] [CrossRef] [PubMed]
- Ketterer, T.; West, D.W.; Sanders, V.P.; Hossain, J.; Kondo, M.C.; Sharif, I. Correlates of patient portal enrollment and activation in primary care pediatrics. Acad. Pediatr. 2013, 13, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Liang, M.; Sanchez, R.; Yu, M.; Budd, P.R.; Sprague, J.L.; Dewar, M.A. On the effect of electronic patient portal on primary care utilization and appointment adherence. BMC Med. Inf. Decis. Mak. 2018, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.E.; Huang, J.; Brand, R.J.; Neugebauer, R.; Graetz, I.; Hsu, J.; Ballard, D.W.; Grant, R. Patients with complex chronic conditions: Health care use and clinical events associated with access to a patient portal. PLoS ONE 2019, 14, e0217636. [Google Scholar] [CrossRef] [PubMed]
- Ancker, J.S.; Barrón, Y.; Rockoff, M.L.; Hauser, D.; Pichardo, M.; Szerencsy, A.; Calman, N. Use of an electronic patient portal among disadvantaged populations. J. Gen. Intern. Med. 2011, 26, 1117–1123. [Google Scholar] [CrossRef]
- Greenberg, A.J.; Falisi, A.L.; Finney Rutten, L.J.; Chou, W.S.; Patel, V.; Moser, R.P.; Hesse, B.W. Access to Electronic Personal Health Records Among Patients With Multiple Chronic Conditions: A Secondary Data Analysis. J. Med. Internet Res. 2017, 19, e188. [Google Scholar] [CrossRef]
- Luque, A.E.; van Keken, A.; Winters, P.; Keefer, M.C.; Sanders, M.; Fiscella, K. Barriers and Facilitators of Online Patient Portals to Personal Health Records Among Persons Living with HIV: Formative Research. JMIR Res. Protoc. 2013, 2, e8. [Google Scholar] [CrossRef] [PubMed]
- Quittner, A.L.; Abbott, J.; Hussain, S.; Ong, T.; Uluer, A.; Hempstead, S.; Lomas, P.; Smith, B. Integration of mental health screening and treatment into cystic fibrosis clinics: Evaluation of initial implementation in 84 programs across the United States. Pediatr. Pulmonol. 2020, 55, 2995–3004. [Google Scholar] [CrossRef] [PubMed]
- Premji, S.S.; Dobson, K.S.; Prashad, A.; Yamamoto, S.; Tao, F.; Zhu, B.; Wu, X.; Lu, M.; Shao, S. What stakeholders think: Perceptions of perinatal depression and screening in China’s primary care system. BMC Pregnancy Childbirth 2021, 21, 15. [Google Scholar] [CrossRef] [PubMed]
- Mospan, C.M.; Gillette, C.; Wilson, J.A. Patient and prescriber perceptions of depression screening within a community pharmacy setting. J. Am. Pharm. Assoc. 2020, 60, S15–S22. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J. Clarity out of chaos: Use of theory in implementation research. Psychiatry Res. 2020, 283, 112461. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, D.; Staab, E.M.; Ridgway, J.P.; Schmitt, J.; Franco, M.; Hunter, S.J.; Motley, D.; Laiteerapong, N. Population-Level Portal-Based Anxiety and Depression Screening Perspectives in HIV Care Clinicians: Qualitative Study Using the Consolidated Framework for Implementation Research. JMIR Form. Res. 2024, 8, e48935. [Google Scholar] [CrossRef]
- Franco, M.I.; Staab, E.M.; Zhu, M.; Knitter, A.; Wan, W.; Gibbons, R.; Vinci, L.; Shah, S.; Yohanna, D.; Beckman, N.; et al. Pragmatic Clinical Trial of Population Health, Portal-Based Depression Screening: The PORTAL-Depression Study. J. Gen. Intern. Med. 2023, 38, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Staab, E.M.; Franco, M.I.; Zhu, M.; Wan, W.; Gibbons, R.D.; Vinci, L.M.; Beckman, N.; Yohanna, D.; Laiteerapong, N. Population Health Management Approach to Depression Symptom Monitoring in Primary Care via Patient Portal: A Randomized Controlled Trial. Am. J. Med. Qual. 2023, 38, 188–195. [Google Scholar] [CrossRef]
- CFIR Guide. Available online: https://cfirguide.org/guide/app/#/ (accessed on 6 April 2022).
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- CFIR Constructs. Available online: https://cfirguide.org/constructs/ (accessed on 6 April 2022).
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Elsman, E.B.M.; van Munster, E.P.J.; van Nassau, F.; Verstraten, P.; van Nispen, R.M.A.; van der Aa, H.P.A. Perspectives on Implementing the Patient Health Questionnaire-4 in Low-Vision Service Organizations to Screen for Depression and Anxiety. Transl. Vis. Sci. Technol. 2022, 11, 16. [Google Scholar] [CrossRef]
- Kip, E.C.; Udedi, M.; Kulisewa, K.; Go, V.F.; Gaynes, B.N. Barriers and facilitators to implementing the HEADSS psychosocial screening tool for adolescents living with HIV/AIDS in teen club program in Malawi: Health care providers perspectives. Int. J. Ment. Health Syst. 2022, 16, 8. [Google Scholar] [CrossRef]
- Abas, M.; Nyamayaro, P.; Bere, T.; Saruchera, E.; Mothobi, N.; Simms, V.; Mangezi, W.; Macpherson, K.; Croome, N.; Magidson, J.; et al. Feasibility and Acceptability of a Task-Shifted Intervention to Enhance Adherence to HIV Medication and Improve Depression in People Living with HIV in Zimbabwe, a Low Income Country in Sub-Saharan Africa. AIDS Behav. 2018, 22, 86–101. [Google Scholar] [CrossRef]
- Bassett, S.M.; Brody, L.R.; Jack, D.C.; Weber, K.M.; Cohen, M.H.; Clark, T.M.; Dale, S.K.; Moskowitz, J.T. Feasibility and Acceptability of a Program to Promote Positive Affect, Well-Being and Gender Empowerment in Black Women Living with HIV. AIDS Behav. 2021, 25, 1737–1750. [Google Scholar] [CrossRef]
- Bassett, S.M.; Cohn, M.; Cotten, P.; Kwok, I.; Moskowitz, J.T. Feasibility and Acceptability of an Online Positive Affect Intervention for Those Living with Comorbid HIV Depression. AIDS Behav. 2019, 23, 753–764. [Google Scholar] [CrossRef]
- Junkins, A.; Psaros, C.; Ott, C.; Azuero, A.; Lambert, C.C.; Cropsey, K.; Savage, R.; Haberer, J.E.; Safren, S.A.; Kempf, M.C. Feasibility, acceptability, and preliminary impact of telemedicine-administered cognitive behavioral therapy for adherence and depression among African American women living with HIV in the rural South. J. Health Psychol. 2021, 26, 2730–2742. [Google Scholar] [CrossRef]
- Duvall, M.J.; Miller, N.E.; North, F.; Leasure, W.B.; Pecina, J.L. Portal Message Language Use Prior to Suicide, Suicide Attempts, and Hospitalization for Depression. Telemed. e-Health 2022, 28, 1143–1150. [Google Scholar] [CrossRef]
- Sankar, P.; Mora, S.; Merz, J.F.; Jones, N.L. Patient perspectives of medical confidentiality: A review of the literature. J. Gen. Intern. Med. 2003, 18, 659–669. [Google Scholar] [CrossRef]
- Jimenez, J.; Del Rio, A.; Berman, A.N.; Grande, M. Personalizing Digital Health: Adapting Health Technology Systems to Meet the Needs of Different Older Populations. Healthcare 2023, 11, 2140. [Google Scholar] [CrossRef]
- Mavandadi, S.; Wright, E.; Klaus, J.; Oslin, D. Message Framing and Engagement in Specialty Mental Health Care: A Follow-up Analysis. Psychiatr. Serv. 2018, 69, 1109–1112. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Rao, Q.; Cai, Z.; Lv, Y.; Wu, T.; Shi, Z.; Sharma, M.; Zhao, Y.; Hou, X. Effects of Goal-Framed Messages on Mental Health Education among Medical University Students: Moderating Role of Personal Involvement. Front. Public Health 2019, 7, 371. [Google Scholar] [CrossRef] [PubMed]
- Whitton, A.E.; Hardy, R.; Cope, K.; Gieng, C.; Gow, L.; MacKinnon, A.; Gale, N.; O’Moore, K.; Anderson, J.; Proudfoot, J.; et al. Mental Health Screening in General Practices as a Means for Enhancing Uptake of Digital Mental Health Interventions: Observational Cohort Study. J. Med. Internet Res. 2021, 23, e28369. [Google Scholar] [CrossRef] [PubMed]
- Simola, S.; Horhammer, I.; Xu, Y.; Barkas, A.; Fagerlund, A.J.; Hagstrom, J.; Holmroos, M.; Hagglund, M.; Johansen, M.A.; Kane, B.; et al. Patients’ Experiences of a National Patient Portal and Its Usability: Cross-Sectional Survey Study. J. Med. Internet Res. 2023, 25, e45974. [Google Scholar] [CrossRef]
- Irizarry, T.; DeVito Dabbs, A.; Curran, C.R. Patient Portals and Patient Engagement: A State of the Science Review. J. Med. Internet Res. 2015, 17, e148. [Google Scholar] [CrossRef]

{kind=link}
| Participant Characteristics (n = 12) | n (%) |
|---|---|
| Age (range) | 38.8 ± 10.5 (26–57) |
| Gender identity a | |
| Male | 10 (83.3) |
| Female | 2 (16.7) |
| Race/Ethnicity b | |
| Black | 9 (75) |
| Hispanic or Latinx | 1 (8.3) |
| Hawaiian/Pacific Islander | 1 (8.3) |
| White | 1 (8.3) |
| Sexual orientation c | |
| Gay | 6 (50) |
| Bisexual | 3 (25) |
| Heterosexual/Straight | 3 (25) |
| Prefer not to answer | 1 (8.3) |
| Years living with HIV (range, n = 10) | 10.6 ± 8.1 (1–22) |
| Anxiety or depression diagnosis | 6 (50) |
| Employment status | |
| Employed | 8 (66.7) |
| Unemployed | 3 (25) |
| Retired | 1 (8.3) |
| Marital status | |
| Single, never married | 6 (50) |
| Single, separated | 2 (16.7) |
| Unmarried, living with a partner | 3 (25) |
| Married | 1 (8.3) |
| Education | |
| High school graduate/GED | 5 (41.7) |
| Some college or technical school | 4 (33.3) |
| 4-year college degree | 3 (25) |
| Electronic portal usage | |
| Current use | 8 (67) |
| Intent to use in the future | 2 (16.7) |
| Domain | Facilitators | Barriers |
|---|---|---|
| Intervention characteristics | Absence of alternative screening methods Approachable design Perceived adaptability | Difficult-to-navigate patient portal system |
| Outer setting | Stigmatization from the healthcare system | |
| Inner setting | High compatibility with HIV care | Lack of technical support Utility dependent on care team response time Novel communication method |
| Characteristics of individuals | Screening viewed as an important part of linkage to treatment Screening may increase self-awareness | |
| Process | Bundling screening with scheduled visits Communicating an action plan for results |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walker, J.A.; Staab, E.M.; Ridgway, J.P.; Schmitt, J.; Franco, M.I.; Hunter, S.; Motley, D.; Laiteerapong, N. Patient Perspectives on Portal-Based Anxiety and Depression Screening in HIV Care: A Qualitative Study Using the Consolidated Framework for Implementation Research. Int. J. Environ. Res. Public Health 2024, 21, 692. https://doi.org/10.3390/ijerph21060692
Walker JA, Staab EM, Ridgway JP, Schmitt J, Franco MI, Hunter S, Motley D, Laiteerapong N. Patient Perspectives on Portal-Based Anxiety and Depression Screening in HIV Care: A Qualitative Study Using the Consolidated Framework for Implementation Research. International Journal of Environmental Research and Public Health. 2024; 21(6):692. https://doi.org/10.3390/ijerph21060692
Chicago/Turabian StyleWalker, Jacob A., Erin M. Staab, Jessica P. Ridgway, Jessica Schmitt, Melissa I. Franco, Scott Hunter, Darnell Motley, and Neda Laiteerapong. 2024. "Patient Perspectives on Portal-Based Anxiety and Depression Screening in HIV Care: A Qualitative Study Using the Consolidated Framework for Implementation Research" International Journal of Environmental Research and Public Health 21, no. 6: 692. https://doi.org/10.3390/ijerph21060692