

The Long-Term Effect of Weight Loss on the Prevention of Progression to Cirrhosis among Patients with Obesity and MASH-Related F3 Liver Fibrosis

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
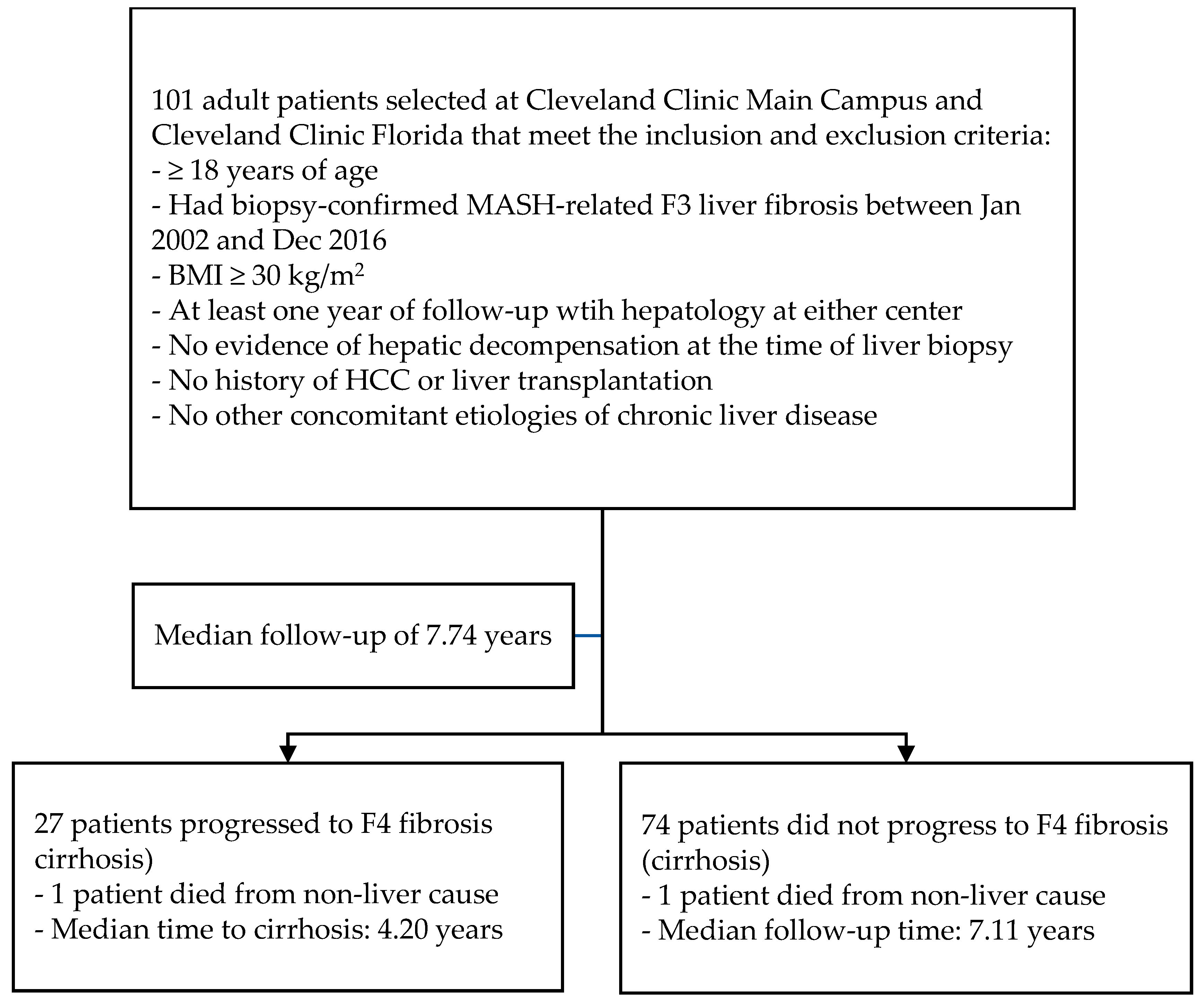
2.1. Study Design
2.2. Diagnostic Criteria and Data Collection
2.3. Study Endpoint
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multi-Society Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef] [PubMed]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Chang Liu, Y.; McCullough, A.J. Nonalcoholic Fatty Liver Disease: A Spectrum of Clinical and Pathological Severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and Validation of a Histological Scoring System for Nonalcoholic Fatty Liver Disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Dargère, D.; Paradis, V. Sampling Variability of Liver Fibrosis in Chronic Hepatitis C. Hepatology 2003, 38, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Tabas, I.; Pajvani, U.B. Mechanisms of Fibrosis Development in Nonalcoholic Steatohepatitis. Gastroenterology 2020, 158, 1913–1928. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Van Natta, M.L.; Clark, J.; Neuschwander-Tetri, B.A.; Diehl, A.; Dasarathy, S.; Loomba, R.; Chalasani, N.; Kowdley, K.; Hameed, B.; et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2021, 385, 1559–1569. [Google Scholar] [CrossRef]
- Axley, P.; Mudumbi, S.; Sarker, S.; Kuo, Y.F.; Singal, A. Patients with Stage 3 Compared to Stage 4 Liver Fibrosis Have Lower Frequency of and Longer Time to Liver Disease Complications. PLoS ONE 2018, 13, e0197117. [Google Scholar] [CrossRef]
- Loomba, R.; Adams, L.A. The 20% Rule of NASH Progression: The Natural History of Advanced Fibrosis and Cirrhosis Caused by NASH. Hepatology 2019, 70, 1885–1888. [Google Scholar] [CrossRef]
- Li, A.A.; Ahmed, A.; Kim, D. Extrahepatic Manifestations of Nonalcoholic Fatty Liver Disease. Gut Liver 2020, 14, 75–85. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Cotter, T.G.; Rinella, M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Cassader, M.; Rosina, F.; Gambino, R. Impact of Current Treatments on Liver Disease, Glucose Metabolism and Cardiovascular Risk in Non-Alcoholic Fatty Liver Disease (NAFLD): A Systematic Review and Meta-Analysis of Randomised Trials. Diabetologia 2012, 55, 885–904. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Friedman, S.L.; Diago, M.; Romero-Gomez, M. Weight Loss through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015, 149, 367–378.e5. [Google Scholar] [CrossRef] [PubMed]
- Promrat, K.; Kleiner, D.E.; Niemeier, H.M.; Jackvony, E.; Kearns, M.; Wands, J.R.; Fava, J.L.; Wing, R.R. Randomized Controlled Trial Testing the Effects of Weight Loss on Nonalcoholic Steatohepatitis. Hepatology 2010, 51, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridi, M.; Hiriart, J.B.; Lupsor-Platon, M.; Bronte, F.; Boursier, J.; Elshaarawy, O.; Marra, F.; Thiele, M.; Markakis, G.; Payance, A.; et al. Refining the Baveno VI Elastography Criteria for the Definition of Compensated Advanced Chronic Liver Disease. J. Hepatol. 2021, 74, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Montesi, L.; El Ghoch, M.; Brodosi, L.; Calugi, S.; Marchesini, G.; Grave, R.D. Long-Term Weight Loss Maintenance for Obesity: A Multidisciplinary Approach. Diabetes Metab. Syndr. Obes. 2016, 9, 37–46. [Google Scholar] [PubMed]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.; Nitta, H.; Otsuka, K.; Umemura, A.; Baba, S.; Obuchi, T.; Wakabayash, G. Bariatric Surgery and Non-Alcoholic Fatty Liver Disease: Current and Potential Future Treatments. Front. Endocrinol. 2014, 5, 164. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.-S.; Harrison, S.A. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef]
- Nevola, R.; Epifani, R.; Imbriani, S.; Tortorella, G.; Aprea, C.; Galiero, R.; Rinaldi, L.; Marfella, R.; Sasso, F.C. GLP-1 Receptor Agonists in Non-Alcoholic Fatty Liver Disease: Current Evidence and Future Perspectives. Int. J. Mol. Sci. 2023, 24, 1703. [Google Scholar] [CrossRef] [PubMed]
- Yki-Järvinen, H. Non-Alcoholic Fatty Liver Disease as a Cause and a Consequence of Metabolic Syndrome. Lancet Diabetes Endocrinol. 2014, 2, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, M.; Patel, P.; Dunn-Valadez, S.; Dao, C.; Khan, V.; Ali, H.; El-Serag, L.; Hernaez, R.; Sisson, A.; Thrift, A.P.; et al. Women Have a Lower Risk of Nonalcoholic Fatty Liver Disease but a Higher Risk of Progression vs Men: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 61–71.e15. [Google Scholar] [CrossRef] [PubMed]
- Wagenknecht, L.E.; Scherzinger, A.L.; Stamm, E.R.; Hanley, A.J.G.; Norris, J.M.; Chen, Y.D.I.; Bryer-Ash, M.; Haffner, S.M.; Rotter, J.I. Correlates and Heritability of Nonalcoholic Fatty Liver Disease in a Minority Cohort. Obesity 2009, 17, 1240–1246. [Google Scholar] [CrossRef]
- Marchesini, G.; Day, C.P.; Dufour, J.F.; Canbay, A.; Nobili, V.; Ratziu, V.; Tilg, H.; Roden, M.; Gastaldelli, A.; Yki-Jarvinen, H.; et al. EASL-EASD-EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | n = 101 1 |
|---|---|
| Gender Female Male | 72 (71%) 29 (29%) |
| Body mass index (kg/m2) | 34.38 (30.88, 40.40) |
| Age at diagnosis (year) | 53.65 (46.52, 62.07) |
| Alcohol status Never Past or Current | 65 (64%) 36 (36%) |
| Smoking status Never Past or Current | 48 (48%) 53 (52%) |
| MELD-Na score at baseline | 6.0 (6.00, 6.00) |
| Child-Turcotte-Pugh score at baseline | 5.0 (5.00, 5.00) |
| Hypertension | 81 (80%) |
| Hyperlipidemia | 75 (74%) |
| Diabetes mellitus | 66 (65%) |
| Metabolic syndrome | 85 (84%) |
| Baseline triglyceride (mg/dL) | 165.00 (115.00, 216.50) |
| Baseline LDL (mg/dL) | 102.50 (82.00, 130.75) |
| Baseline HDL (mg/dL) | 42.50 (35.00, 50.00) |
| Baseline HbA1c (%) | 6.50 (6.00, 7.50) |
| Previous bariatric surgery | 20 (20%) |
| Statin user | 35 (35%) |
| Pentoxifylline user | 25 (25%) |
| Vitamin E user | 30 (30%) |
| GLP-1 RA user | 5 (5.0%) |
| Any pharmacologic a | 66 (65%) |
| Baseline weight (kg) | 98.00 (84.80, 115.00) |
| Weight at 1 year after F3 diagnosis (kg) | 91.20 (81.50, 111.40) |
| Weight loss percentage at 1 year after F3 diagnosis (%) | 1.96 (−0.64, 8.53) |
| Weight loss levels at 1 year after F3 diagnosis 0 or weight gain 0–5% >5% | 36 (36%) 33 (33%) 32 (32%) |
| Weight at the last follow-up visit (kg) | 89.80 (77.20, 107.20) |
| Weight at the last follow-up visit (kg) | 89.80 (77.20, 107.20) |
| Weight loss at the last follow-up visit (%) | 6.07 (−0.65, 12.69) |
| Had pre-existing cardiovascular disease at baseline | 10 (9.9%) |
| Had cardiovascular event during follow-up | 16 (16%) |
| Weight at the cardio event (kg) b | 97.05 (82.67, 105.60) |
| Progression to cirrhosis | 27 (27%) |
| Weight at cirrhosis diagnosis (kg) c | 87.80 (81.15, 101.45) |
| All-cause mortality | 2 (2.0%) |
| Follow-up Time (year) | 7.74 (5.17, 9.85) |
| Progression to Cirrhosis Status | Univariable Analysis Results | ||||
|---|---|---|---|---|---|
| Characteristic, n = 101 | No, n = 74 1 | Yes, n = 27 1 | HR 2 | 95% CI 2 | p-value |
| Gender Female Male | 53 (72%) 21 (28%) | 19 (70%) 8 (30%) | __ 0.98 | __ 0.42, 2.25 | 0.96 |
| Body mass index (kg/m2) | 35.63 (31.03, 40.84) | 33.98 (28.51, 36.98) | 0.98 | 0.93, 1.04 | 0.50 |
| Age (year) | 53.44 (46.26, 59.95) | 55.71 (48.35, 64.33) | 1.03 | 0.98, 1.07 | 0.22 |
| Alcohol status Never Past or Current | 46 (62%) 28 (38%) | 19 (70%) 8 (30%) | __ 0.68 | __ 0.29, 1.57 | 0.35 |
| Smoking status Never Past or Current | 33 (45%) 41 (55) | 15 (56%) 12 (44%) | __ 0.57 | __ 0.26, 1.24 | 0.15 |
| MELD-Na Score | 6.00 (6.00, 6.00) | 6.00 (6.00, 6.00) | 1.21 | 0.72, 2.03 | 0.50 |
| Hypertension No Yes | 13 (18%) 61 (82%) | 7 (26%) 20 (74%) | __ 0.96 | __ 0.38, 2.44 | 0.93 |
| Type 2 diabetes mellitus No Yes | 28 (38%) 46 (62%) | 7 (26%) 20 (74%) | __ 1.82 | __ 0.76, 4.34 | 0.16 |
| Metabolic syndrome No Yes | 12 (16%) 62 (84%) | 4 (15%) 23 (85%) | __ 1.34 | __ 0.46, 3.95 | 0.58 |
| Baseline TC (mg/dL) | 162.50 (125.00, 219.50) | 171.00 (110.25, 204.00) | 1.00 | 1.00, 1.00 | 0.94 |
| Baseline LDL (mg/dL) | 101.50 (81.00, 119.25) | 123.00 (102.75, 143.75) | 1.02 | 1.00, 1.03 | 0.01 |
| Baseline HDL (mg/dL) | 42.00 (34.75, 49.25) | 44.00 (38.00, 51.50) | 1.00 | 0.96, 1.04 | 0.96 |
| Baseline HbA1c (%) | 6.45 (6.00, 7.48) | 6.60 (6.00, 7.60) | 1.18 | 0.84, 1.66 | 0.34 |
| Previous bariatric surgery No Yes | 56 (76%) 18 (24%) | 25 (93%) 2 (7.4%) | __ 0.35 | __ 0.08, 1.47 | 0.094 |
| Statin user No Yes | 48 (65%) 26 (35%) | 18 (67%) 9 (33%) | __ 1.13 | __ 0.50, 2.56 | 0.77 |
| Pentoxifylline user No Yes | 55 (74%) 19 (26%) | 21 (78%) 6 (22%) | __ 0.89 | 0.39, 2.46 | 0.97 |
| Vitamin E user No Yes | 53 (72%) 21 (28%) | 18 (67%) 9 (33%) | __ 1.21 | 0.52, 2.79 | 0.66 |
| GLP-1 RA user No Yes | 69 (93%) 5 (6.8%) | 27 (100%) 0 (0%) | __ 0.00 | __ 0.00, Inf | 0.25 |
| Any pharmacologic a No Yes | 27 (36%) 47 (64%) | 8 (30%) 19 (70%) | __ 1.33 | 0.58, 3.07 | 0.49 |
| Baseline weight (kg) | 103.10 (88.03, 117.15) | 90.20 (82.60, 102.30) | 1.0 | 0.98, 1.03 | 0.50 |
| Weight loss at 1 year after F3 diagnosis (%) | 2.53 (−0.28, 10.27) | 0.41 (−1.55, 4.67) | 0.98 | 0.93, 1.03 | 0.32 |
| Weight loss levels at 1 year after F3 diagnosis 0% or weight gain 0–5% >5% | 23 (31%) 25 (34%) 26 (35%) | 13 (48%) 8 (30%) 6 (22%) | __ 0.74 0.63 | __ 0.30, 1.81 0.24, 1.68 | 0.61 |
| Weight loss percentage at event b (%) | 6.23 (−0.13, 14.07) | −0.06 (−3.31, 7.24) | 0.96 | 0.92, 1.00 | 0.027 |
| Weight loss levels at event 0% or weight gain 0–5% >5% | 19 (26%) 11 (15%) 44 (59%) | 14 (52%) 5 (19%) 8 (30%) | __ 0.97 0.35 | __ 0.35, 2.72 0.14, 0.87 | 0.045 |
| Time to event (years) | 7.11 (4.93, 9.67) | 4.20 (2.83, 8.07) | |||
| Characteristics | HR 1 | 95% CI 2 | p-Value |
|---|---|---|---|
| Baseline age (years) | 1.01 | 0.95, 1.06 | 0.82 |
| BMW at baseline (kg/m2) | 1.01 | 0.94, 1.09 | 0.77 |
| MELD-Na score | 1.36 | 0.85, 2.18 | 0.10 |
| Type 2 diabetes mellitus: Yes vs. No | 3.24 | 1.21, 8.67 | 0.022 |
| LDL (mg/dL) | 1.02 | 1.01, 1.04 | 0.008 |
| Weight loss levels at event a 0–5% vs. No weight loss or weight gain >5% vs. No weight loss or weight gain | 0.94 0.29 | 0.31, 2.86 0.08–0.96 | 0.91 0.043 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niu, J.; Al-Yaman, W.; Pinyopornpanish, K.; Park, J.S.; Salazar, M.; Xiao, H.; Bena, J.; Lyu, R.; Flocco, G.; Junna, S.R.; et al. The Long-Term Effect of Weight Loss on the Prevention of Progression to Cirrhosis among Patients with Obesity and MASH-Related F3 Liver Fibrosis. Int. J. Environ. Res. Public Health 2024, 21, 708. https://doi.org/10.3390/ijerph21060708
Niu J, Al-Yaman W, Pinyopornpanish K, Park JS, Salazar M, Xiao H, Bena J, Lyu R, Flocco G, Junna SR, et al. The Long-Term Effect of Weight Loss on the Prevention of Progression to Cirrhosis among Patients with Obesity and MASH-Related F3 Liver Fibrosis. International Journal of Environmental Research and Public Health. 2024; 21(6):708. https://doi.org/10.3390/ijerph21060708
Chicago/Turabian StyleNiu, Jiafei, Wael Al-Yaman, Kanokwan Pinyopornpanish, Ji Seok Park, Miguel Salazar, Huijun Xiao, James Bena, Ruishen Lyu, Gianina Flocco, Shilpa R. Junna, and et al. 2024. "The Long-Term Effect of Weight Loss on the Prevention of Progression to Cirrhosis among Patients with Obesity and MASH-Related F3 Liver Fibrosis" International Journal of Environmental Research and Public Health 21, no. 6: 708. https://doi.org/10.3390/ijerph21060708
APA StyleNiu, J., Al-Yaman, W., Pinyopornpanish, K., Park, J. S., Salazar, M., Xiao, H., Bena, J., Lyu, R., Flocco, G., Junna, S. R., Adhami, T., Sims, O. T., & Wakim-Fleming, J. (2024). The Long-Term Effect of Weight Loss on the Prevention of Progression to Cirrhosis among Patients with Obesity and MASH-Related F3 Liver Fibrosis. International Journal of Environmental Research and Public Health, 21(6), 708. https://doi.org/10.3390/ijerph21060708