
Predicting Post-Disaster Post-Traumatic Stress Disorder Symptom Trajectories: The Role of Pre-Disaster Traumatic Experiences
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Outcome
2.1.2. Primary Exposure
2.1.3. Covariates
2.2. Analysis
3. Results
3.1. Preliminary Analyses
3.2. Latent Class Growth Analysis
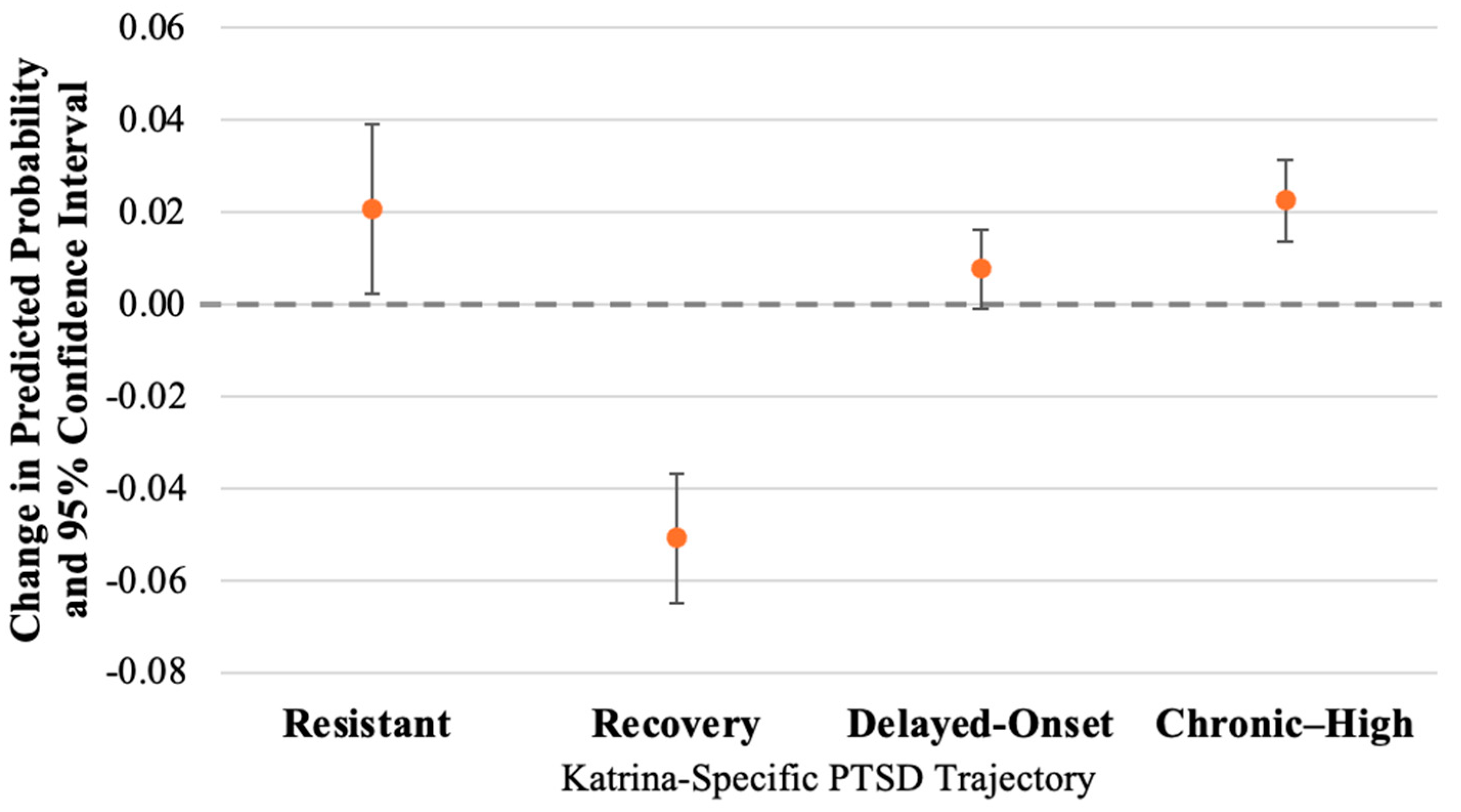
3.3. Predictors of Trajectory Membership
4. Discussion
5. Limitations and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation—IPCC; Cambridge University Press: Cambridge, UK, June 2012; p. 582. Available online: https://www.ipcc.ch/report/managing-the-risks-of-extreme-events-and-disasters-to-advance-climate-change-adaptation/ (accessed on 5 May 2021).
- Disasters in Numbers 2022. Centre for Research on the Epidemiology of Disasters (CRED). 2022. Available online: https://cred.be/sites/default/files/2022_EMDAT_report.pdf (accessed on 7 August 2023).
- Thompson, A. A Running List of Record-Breaking Natural Disasters in 2020—Scientific American. 2020. Available online: https://www.scientificamerican.com/article/a-running-list-of-record-breaking-natural-disasters-in-2020/ (accessed on 29 November 2020).
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Goldstein, R.B.; Smith, S.M.; Chou, S.P.; Saha, T.D.; Jung, J.; Zhang, H.; Pickering, R.P.; Ruan, W.J.; Huang, B.; Grant, B.F. The epidemiology of DSM-5 posttraumatic stress disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Benjet, C.; Bromet, E.J.; Cardoso, G.; Degenhardt, L.; de Girolamo, G.; Dinolova, R.V.; Ferry, F.; et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur. J. Psychotraumatol. 2017, 8 (Suppl. S5), 1353383. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Nandi, A.; Vlahov, D. The Epidemiology of Post-Traumatic Stress Disorder after Disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Post-Traumatic Stress Disorder. National Insitute of Mental Health. Available online: https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd/ (accessed on 5 May 2021).
- Koenen, K.C.; Ratanatharathorn, A.; Ng, L.; McLaughlin, K.A.; Bromet, E.J.; Stein, D.J.; Karam, E.G.; Meron Ruscio, A.; Benjet, C.; Scott, K.; et al. Posttraumatic stress disorder in the World Mental Health Surveys. Psychol. Med. 2017, 47, 2260–2274. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A. Loss, trauma and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 Disaster Victims Speak: Part I. An Empirical Review of the Empirical Literature, 1981–2001. Psychiatry Interpers. Biol. Process. 2002, 65, 207–239. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A. Resilience in the Face of Potential Trauma. Curr. Dir. Psychol. Sci. 2005, 14, 135–138. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Mancini, A.D. The Human Capacity to Thrive in the Face of Potential Trauma. Pediatrics 2008, 121, 369–375. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Mancini, A.D. Beyond resilience and PTSD: Mapping the heterogeneity of responses to potential trauma. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 74–83. [Google Scholar] [CrossRef]
- Norris, F.H.; Tracy, M.; Galea, S. Looking for resilience: Understanding the longitudinal trajectories of responses to stress. Soc. Sci. Med. 2009, 68, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Breslau, N.; Peterson, E.L.; Schultz, L.R. A second look at prior trauma and the posttraumatic stress disorder effects of subsequent trauma: A prospective epidemiological study. Arch. Gen. Psychiatry 2008, 65, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Brewin, C.R.; Andrews, B.; Valentine, J.D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J. Consult. Clin. Psychol. 2000, 68, 748–766. [Google Scholar] [CrossRef] [PubMed]
- Yehuda, R.; Flory, J.D.; Pratchett, L.C.; Buxbaum, J.; Ising, M.; Holsboer, F. Putative biological mechanisms for the association between early life adversity and the subsequent development of PTSD. Psychopharmacology 2010, 212, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; McGrath, J.A.; Young, M.N.; Kwok, R.K.; Engel, L.S.; Galea, S.; Sandler, D.P. Cumulative Disaster Exposure and Mental and Physical Health Symptoms Among a Large Sample of Gulf Coast Residents. J. Trauma. Stress 2019, 32, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.L. Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. J. Trauma. Stress 1992, 5, 377–391. [Google Scholar] [CrossRef]
- Ruggiero, K.J.; Armstadter, A.B.; Acierno, R.; Kilpatrick, D.G.; Resnick, H.S.; Tracy, M.; Galea, S. Social and Psychological Resources Associated with Health Status in a Representative Sample of Adults Affected by the 2004 Florida Hurricanes. Psychiatry Interpers. Biol. Process. 2009, 72, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Karam, E.G.; Friedman, M.J.; Hill, E.D.; Kessler, R.C.; McLaughlin, K.A.; Petukhova, M.; Sampson, L.; Shahly, V.; Angermeyer, M.C.; Bromet, E.J.; et al. Cumulative Traumas and Risk Thresholds: 12-Month Ptsd in the World Mental Health (WMH) Surveys. Depress. Anxiety 2014, 31, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Waters, M.C. Life after Hurricane Katrina: The Resilience in Survivors of Katrina (RISK) Project. Sociol. Forum. 2016, 31 (Suppl. S1), 750–769. [Google Scholar] [CrossRef]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale—Revised. In Assessing Psychological Trauma and PTSD; Guilford Press: New York, NY, USA, 1997; pp. 399–411. [Google Scholar]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric Properties of the Life Events Checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Benjet, C.; Bromet, E.; Karam, E.G.; Kessler, R.C.; McLaughlin, K.A.; Ruscio, A.M.; Shahly, V.; Stein, D.J.; Petukhova, M.; Hill, E.; et al. The epidemiology of traumatic event exposure worldwide: Results from the World Mental Health Survey Consortium. Psychol. Med. 2016, 46, 327–343. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Walsh, K.; Uddin, M.; Galea, S.; Koenen, K.C. Bidirectional relationships between trauma exposure and posttraumatic stress: A longitudinal study of Detroit residents. J. Abnorm. Psychol. 2014, 123, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R.; Resnick, H.; Kilpatrick, D.G. A prospective examination of PTSD symptoms as risk factors for subsequent exposure to potentially traumatic events among women. J. Abnorm. Psychol. 2009, 118, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R.; Resnick, H.; Kilpatrick, D.G. Factors associated with chronicity in posttraumatic stress disorder: A prospective analysis of a national sample of women. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 43–49. [Google Scholar] [CrossRef]
- Raker, E.J.; Lowe, S.R.; Arcaya, M.C.; Johnson, S.T.; Rhodes, J.; Waters, M.C. Twelve years later: The long-term mental health consequences of Hurricane Katrina. Soc. Sci. Med. 2019, 242, 112610. [Google Scholar] [CrossRef] [PubMed]
- Paxson, C.; Fussell, E.; Rhodes, J.; Waters, M. Five years later: Recovery from post traumatic stress and psychological distress among low-income mothers affected by Hurricane Katrina. Soc. Sci. Med. 2012, 74, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Arcaya, M.C.; Lowe, S.R.; Rhodes, J.E.; Waters, M.C.; Subramanian, S.V. Association of PTSD symptoms with asthma attacks among hurricane Katrina survivors. J. Trauma Stress. 2014, 27, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Brodie, M.; Weltzien, E.; Altman, D.; Blendon, R.J.; Benson, J.M. Experiences of Hurricane Katrina evacuees in Houston shelters: Implications for future planning. Am. J. Public Health 2006, 96, 1402–1408. [Google Scholar] [CrossRef]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. In Advances in Personal Relationships: A Research Annual; Jones, W.H., Perlman, D., Eds.; JAI Press: Greenwich, CT, USA, 1987; pp. 37–67. [Google Scholar]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Kessler, R.C.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Bromet, E.; Cuitan, M.; Furukawa, T.A.; Gureje, O.; Hinkov, H.; Hu, C.Y.; et al. Screening for serious mental illness in the general population with the K6 screening scale: Results from the WHO World Mental Health (WMH) survey initiative. Int. J. Methods Psychiatr. Res. 2011, 20, 62. [Google Scholar] [CrossRef]
- Vermunt, J.K. Latent Class Modeling with Covariates: Two Improved Three-Step Approaches. Polit. Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Frankfurt, S.; Frazier, P.; Syed, M.; Jung, K.R. Using Group-Based Trajectory and Growth Mixture Modeling to Identify Classes of Change Trajectories. Couns. Psychol. 2016, 44, 622–660. [Google Scholar] [CrossRef]
- Andruff, H.; Carraro, N.; Thompson, A.; Gaudreau, P.; Louvet, B. Latent Class Growth Modelling: A Tutorial. Tutor. Quant. Methods Psychol. 2009, 5, 11–24. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. A Note on a Stata Plugin for Estimating Group-based Trajectory Models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Nguena Nguefack, H.L.; Pagé, M.G.; Katz, J.; Choinière, M.; Vanasse, A.; Dorais, M.; Samb, O.M.; Lacasse, A. Trajectory Modelling Techniques Useful to Epidemiological Research: A Comparative Narrative Review of Approaches. Clin. Epidemiol. 2020, 12, 1205–1222. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.; Hoekstra, T. Classifying developmental trajectories over time should be done with great caution: A comparison between methods. J. Clin. Epidemiol. 2012, 65, 1078–1087. [Google Scholar] [CrossRef]
- van der Nest, G.; Lima Passos, V.; Candel, M.J.J.M.; van Breukelen, G.J.P. An overview of mixture modelling for latent evolutions in longitudinal data: Modelling approaches, fit statistics and software. Adv. Life Course Res. 2020, 43, 100323. [Google Scholar] [CrossRef] [PubMed]
- Herle, M.; Micali, N.; Abdulkadir, M.; Loos, R.; Bryant-Waugh, R.; Hübel, C.; Bulik, C.M.; De Stavola, B.L. Identifying typical trajectories in longitudinal data: Modelling strategies and interpretations. Eur. J. Epidemiol. 2020, 35, 205–222. [Google Scholar] [CrossRef]
- Conley, A.H.; Overstreet, C.M.; Hawn, S.E.; Kendler, K.S.; Dick, D.M.; Amstadter, A.B. Prevalence and predictors of sexual assault among a college sample. J. Am. Coll. Health 2017, 65, 41–49. [Google Scholar] [CrossRef]
- Galatzer-Levy, I.; Huang, S.; Bonanno, G. Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clin. Psychol. Rev. 2018, 63, 41–55. [Google Scholar] [CrossRef]
- Harville, E.W.; Shankar, A.; Dunkel Schetter, C.; Lichtveld, M. Cumulative effects of the Gulf oil spill and other disasters on mental health among reproductive-aged women: The Gulf Resilience on Women’s Health study. Psychol. Trauma Theory Res. Pract. Policy 2017, 10, 533–541. [Google Scholar] [CrossRef]
- Ersing, R.L.; Pearce, C.; Collins, J.; Saunders, M.E.; Polen, A. Geophysical and Social Influences on Evacuation Decision-Making: The Case of Hurricane Irma. Atmosphere 2020, 11, 851. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Mean (SD) or % | ||
|---|---|---|
| Baseline sociodemographics | ||
| Age (years) | 25.14 (4.46) | |
| Non-Hispanic Black | 86.1% | |
| Married or cohabitating | 23.7% | |
| Number of public benefits received (range: 0–4) | 0.94 (0.71) | |
| Pre-Katrina perceived social support (range: 1–4) | 3.20 (0.44) | |
| Pre-Katrina psychological distress (range: 0–24) | 4.97 (4.18) | |
| Pre-Katrina trauma exposure | ||
| Experienced any pre-Katrina trauma | 61.3% | |
| Number of pre-Katrina traumas experienced (range: 0–14) | 1.66 (1.98) | |
| Number of pre-Katrina assaultive traumas experienced (range: 0–5) | 0.80 (1.12) | |
| Number of pre-Katrina non-assaultive traumas experienced (range: 0–9) | 0.87 (1.20) | |
| Katrina-related trauma and hardship | ||
| Number of Katrina-related traumas (range: 0–8) | 3.00 (2.29) | |
| Family member or friend died due to Katrina | 39.3% | |
| Moderate or severe home damage due to Katrina | 83.4% | |
| Post-Katrina trauma exposure | ||
| Experienced any post-Katrina trauma | 87.4% | |
| Number of post-Katrina traumas experienced (range: 0–15) | 2.60 (1.99) | |
| Katrina-specific post-traumatic stress disorder 1 (PTSD) | ||
| Time 1 (one year post-Katrina) | 48.1% | |
| Time 2 (four years post-Katrina) | 35.8% | |
| Time 3 (12 years post-Katrina) | 18.7% | |
| Number of Classes | AIC | BIC | Adj. BIC | Mean Posterior Probability (SD) |
|---|---|---|---|---|
| 1 | −2662.18 | −2669.07 | −2670.51 | -- |
| 2 | −2528.34 | −2542.11 | −2545.00 | 0.91 (0.04) |
| 3 | −2516.81 | −2537.46 | −2541.79 | 0.80 (0.10) |
| 4 | −2494.79 | −2522.34 | −2528.11 | 0.79 (0.06) |
| 5 | −2493.54 | −2527.97 | −2535.18 | 0.70 (0.08) |
| 6 | −2496.54 | −2537.85 | −2546.51 | 0.51 (0.29) |
| 7 | −2499.54 | −2547.74 | −2557.84 | 0.35 (0.30) |
| 8 | −2502.54 | −2557.62 | −2569.17 | 0.32 (0.31) |
| 9 | −2505.54 | −2567.51 | −2580.49 | 0.27 (0.29) |
| 10 | −2504.06 | −2572.92 | −2587.35 | 0.30 (0.33) |
| Number of Classes | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 100.0% | |||||||||
| 2 | 71.8% | 28.2% | ||||||||
| 3 | 59.8% | 22.3% | 17.9% | |||||||
| 4 | 49.0% | 8.0% | 29.3% | 13.7% | ||||||
| 5 | 32.5% | 33.3% | 7.8% | 13.3% | 13.2% | |||||
| 6 | 15.5% | 7.8% | 17.0% | 33.3% | 13.3% | 13.2% | ||||
| 7 | 15.4% | 7.8% | 17.1% | 16.1% | 17.2% | 13.3% | 13.2% | |||
| 8 | 12.5% | 7.8% | 10.8% | 9.2% | 15.4% | 17.8% | 13.3% | 13.2% | ||
| 9 | 11.5% | 7.8% | 11.7% | 9.3% | 10.9% | 11.7% | 10.6% | 13.3% | 13.2% | |
| 10 | 8.6% | 9.6% | 8.0% | 13.7% | 10.7% | 12.2% | 9.5% | 12.6% | 13.8% | 1.3% |
| Trajectory Group | |||||
|---|---|---|---|---|---|
| Resistant (n = 357, 49.0%) | Recovery (n = 213, 29.3%) | Delayed-Onset (n = 58, 8.0%) | Chronic–High (n = 100, 13.7%) | ||
| Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | ||
| Baseline sociodemographics | |||||
| Age (years) | 24.58 (4.18) | 25.54 (4.70) | 26.03 (5.05) | 26.35 (4.24) | |
| Non-Hispanic Black | 80.2% | 91.0% | 92.7% | 92.8% | |
| Married or cohabitating | 26.3% | 20.2% | 22.8% | 22.2% | |
| Number of public benefits received (range: 0–4) | 0.86 (0.74) | 0.99 (0.70) | 0.97 (0.59) | 1.09 (0.70) | |
| Pre-Katrina perceived social support (range: 1–4) | 3.27 (0.42) | 3.15 (0.47) | 3.17 (0.41) | 3.09 (0.45) | |
| Pre-Katrina psychological distress (range: 0–24) | 4.31 (3.70) | 5.53 (4.34) | 5.32 (4.62) | 5.92 (4.82) | |
| Pre-Katrina trauma exposure | |||||
| Experienced any pre-Katrina trauma | 58.2% | 59.6% | 70.2% | 69.2% | |
| Number of pre-Katrina traumas experienced (range: 0–14) | 1.45 (1.82) | 1.47 (1.61) | 2.04 (2.05) | 2.52 (2.75) | |
| Number of pre-Katrina assaultive traumas experienced (range: 0–5) | 0.67 (0.99) | 0.71 (1.01) | 1.09 (1.24) | 1.18 (1.50) | |
| Number of pre-Katrina non-assaultive traumas experienced (range: 0–9) | 0.77 (1.15) | 0.77 (1.01) | 0.95 (1.12) | 1.33 (1.59) | |
| Katrina-related trauma and hardship | |||||
| Number of Katrina-related traumas (range: 0–8) | 2.27 (1.93) | 3.41 (2.32) | 3.46 (2.29) | 4.46 (2.44) | |
| Family member or friend died due to Katrina | 26.1% | 50.2% | 35.1% | 65.0% | |
| Moderate or severe home damage due to Katrina | 78.3% | 89.1% | 77.4% | 92.7% | |
| Post-Katrina trauma exposure | |||||
| Experienced any post-Katrina trauma | 86.2% | 86.9% | 93.0% | 89.0% | |
| Number of post-Katrina traumas experienced (range: 0–15) | 2.19 (1.66) | 2.66 (1.94) | 3.28 (2.10) | 3.45 (2.55) | |
| Katrina-specific post-traumatic stress disorder (PTSD) | |||||
| Time 1 (one year post-Katrina) | 0.82 (0.59) | 2.12 (0.64) | 1.14 (0.59) | 2.82 (0.53) | |
| Time 2 (four years post-Katrina) | 0.57 (0.52) | 1.61 (0.68) | 1.39 (0.76) | 2.69 (0.62) | |
| Time 3 (twelve years post-Katrina) | 0.21 (0.34) | 0.43 (0.46) | 2.17 (0.60) | 1.87 (0.76) | |
| Trajectory Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Resistant | Recovery | Delayed-Onset | Chronic–High | |||||||
| Crude | Fully Adjusted | Crude | Fully Adjusted | Crude | Fully Adjusted | Crude | Fully Adjusted | |||
| Pre-Katrina Trauma Exposure 1 | ||||||||||
| Predicted probability at mean level of pre-Katrina trauma exposure | 0.50 (0.46, 0.53) | 0.50 (0.46, 0.53) | 0.30 (0.26, 0.33) | 0.30 (0.26, 0.33) | 0.08 (0.06, 0.10) | 0.08 (0.06, 0.10) | 0.13 (0.10, 0.15) | 0.13 (0.11, 0.15) | ||
| Predicted probability at 1 SD above mean | 0.45 (0.39, 0.50) | 0.52 (0.46, 0.57) | 0.27 (0.22, 0.32) | 0.24 (0.20, 0.29) | 0.10 (0.07, 0.13) | 0.09 (0.06, 0.12) | 0.18 (0.14, 0.22) | 0.15 (0.12, 0.19) | ||
| Difference | −0.05 (−0.07, −0.03) | 0.02 (0.002, 0.04) | −0.02 (−0.04, −0.01) | −0.05 (−0.06, −0.04) | 0.02 (0.01, 0.03) | 0.01 (−0.001, 0.02) | 0.05 (0.04, 0.07) | 0.02 (0.01, 0.03) | ||
| Percent change in probability | −10.1% | 4.2% | −7.4% | −17.2% | 21.3% | 9.7% | 43.0% | 17.3% | ||
| Pre-Katrina Assaultive Trauma Exposure | ||||||||||
| Predicted probability at mean level of pre-Katrina assaultive trauma exposure | 0.50 (0.46, 0.53) | 0.49 (0.46, 0.53) | 0.30 (0.26, 0.33) | 0.29 (0.26, 0.33) | 0.08 (0.06, 0.10) | 0.08 (0.06, 0.10) | 0.13 (0.10, 0.15) | 0.13 (0.11, 0.16) | ||
| Predicted probability at 1 SD above mean | 0.45 (0.39, 0.50) | 0.49 (0.43, 0.55) | 0.28 (0.23, 0.33) | 0.27 (0.22, 0.32) | 0.10 (0.07, 0.13) | 0.10 (0.06, 0.13) | 0.18 (0.14, 0.21) | 0.14 (0.11, 0.18) | ||
| Difference | −0.05 (−0.07, −0.03) | −0.003 (−0.03, 0.02) | −0.02 (−0.03, −0.002) | −0.02 (−0.04, −0.01) | 0.02 (0.01, 0.03) | 0.02 (0.01, 0.03) | 0.05 (0.03, 0.06) | 0.01 (0.001, 0.02) | ||
| Percent change in probability | −10.1% | −0.6% | −5.7% | −8.3% | 26.4% | 22.2% | 35.5% | 7.5% | ||
| Pre-Katrina Non-Assaultive Trauma Exposure | ||||||||||
| Predicted probability at mean level of pre-Katrina non-assaultive trauma exposure | 0.50 (0.46, 0.53) | 0.49 (0.46, 0.53) | 0.29 (0.26, 0.33) | 0.29 (0.26, 0.33) | 0.08 (0.06, 0.10) | 0.08 (0.06, 0.10) | 0.13 (0.10, 0.15) | 0.13 (0.11, 0.16) | ||
| Predicted probability at 1 SD above mean | 0.46 (0.41, 0.52) | 0.52 (0.47, 0.57) | 0.27 (0.22, 0.33) | 0.26 (0.21, 0.31) | 0.09 (0.06, 0.12) | 0.07 (0.05, 0.10) | 0.18 (0.14, 0.21) | 0.15 (0.11, 0.18) | ||
| Difference | −0.04 (−0.05, −0.02) | 0.03 (0.01, 0.05) | −0.02 (−0.04, −0.002) | −0.04 (−0.05, −0.02) | 0.01 (−0.002, 0.02) | −0.01 (−0.01, −0.001) | 0.05 (0.03, 0.06) | 0.02 (0.01, 0.02) | ||
| Percent change in probability | −7.1% | 5.7% | −6.6% | −12.5% | 9.5% | −8.9% | 36.5% | 12.2% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, S.T.; Mason, S.M.; Erickson, D.; Slaughter-Acey, J.C.; Waters, M.C. Predicting Post-Disaster Post-Traumatic Stress Disorder Symptom Trajectories: The Role of Pre-Disaster Traumatic Experiences. Int. J. Environ. Res. Public Health 2024, 21, 749. https://doi.org/10.3390/ijerph21060749
Johnson ST, Mason SM, Erickson D, Slaughter-Acey JC, Waters MC. Predicting Post-Disaster Post-Traumatic Stress Disorder Symptom Trajectories: The Role of Pre-Disaster Traumatic Experiences. International Journal of Environmental Research and Public Health. 2024; 21(6):749. https://doi.org/10.3390/ijerph21060749
Chicago/Turabian StyleJohnson, Sydney T., Susan M. Mason, Darin Erickson, Jaime C. Slaughter-Acey, and Mary C. Waters. 2024. "Predicting Post-Disaster Post-Traumatic Stress Disorder Symptom Trajectories: The Role of Pre-Disaster Traumatic Experiences" International Journal of Environmental Research and Public Health 21, no. 6: 749. https://doi.org/10.3390/ijerph21060749