
Identifying Populations at Risk for Lung Cancer Mortality from the National Health and Nutrition Examination Survey (2001–2018) Using the 2021 USPSTF Screening Guidelines


Abstract
1. Introduction
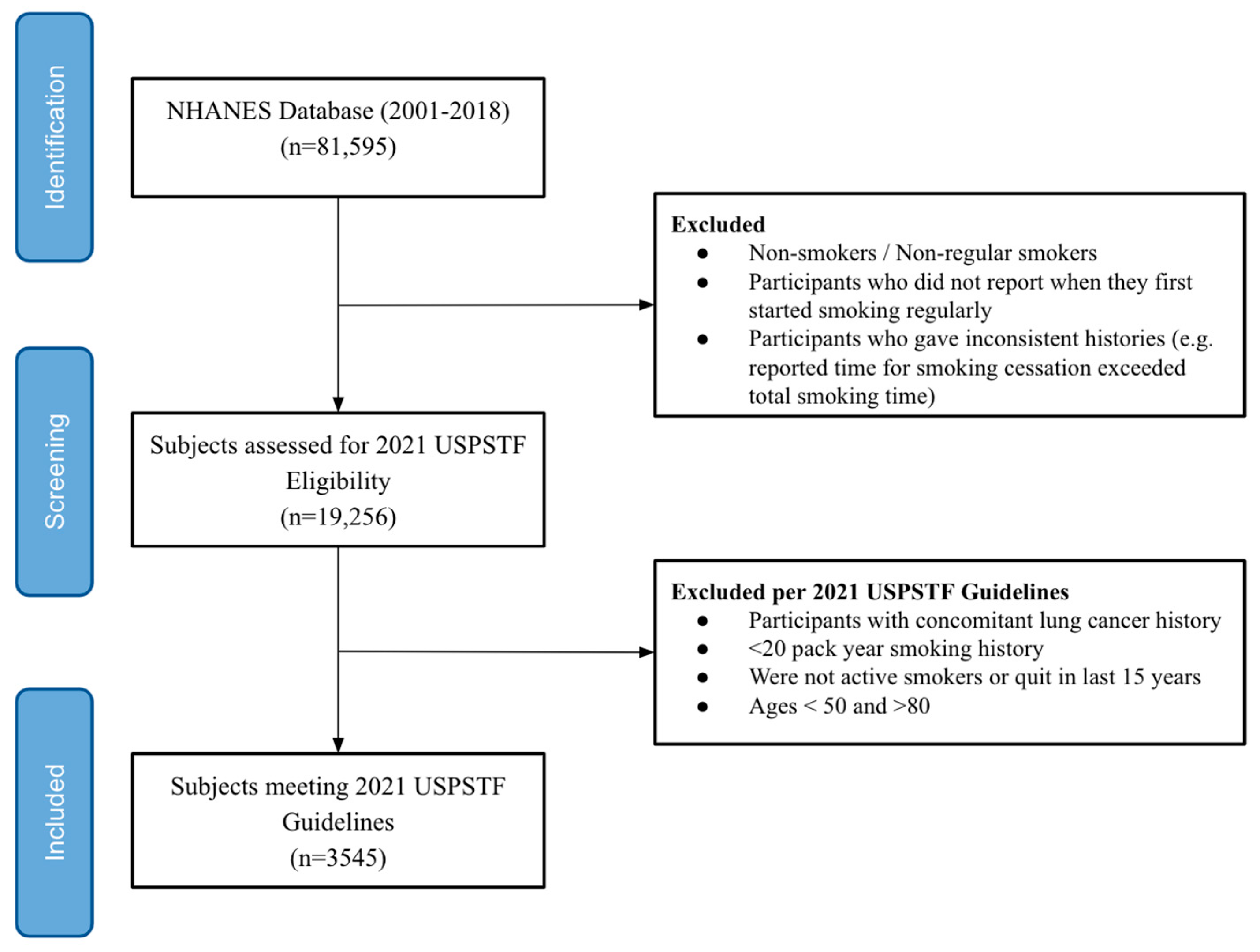
2. Materials and Methods
3. Results
3.1. Risk of Lung Cancer Death by Gender
3.2. Risk of Lung Cancer Death by Race
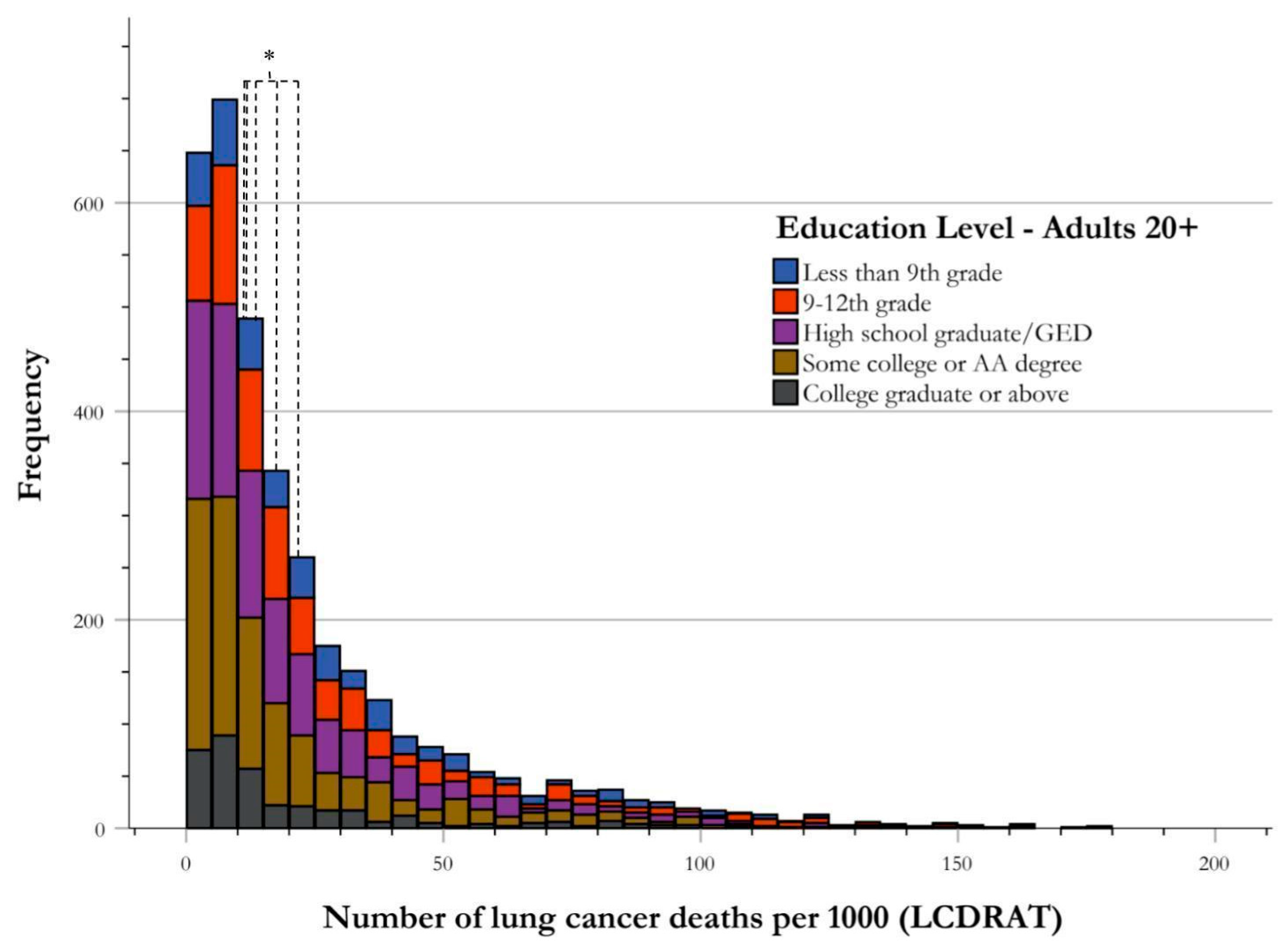
3.3. Risk of Lung Cancer Death by Education Attainment Level
3.4. Risk of Lung Cancer Death by Presence of Emotional Support
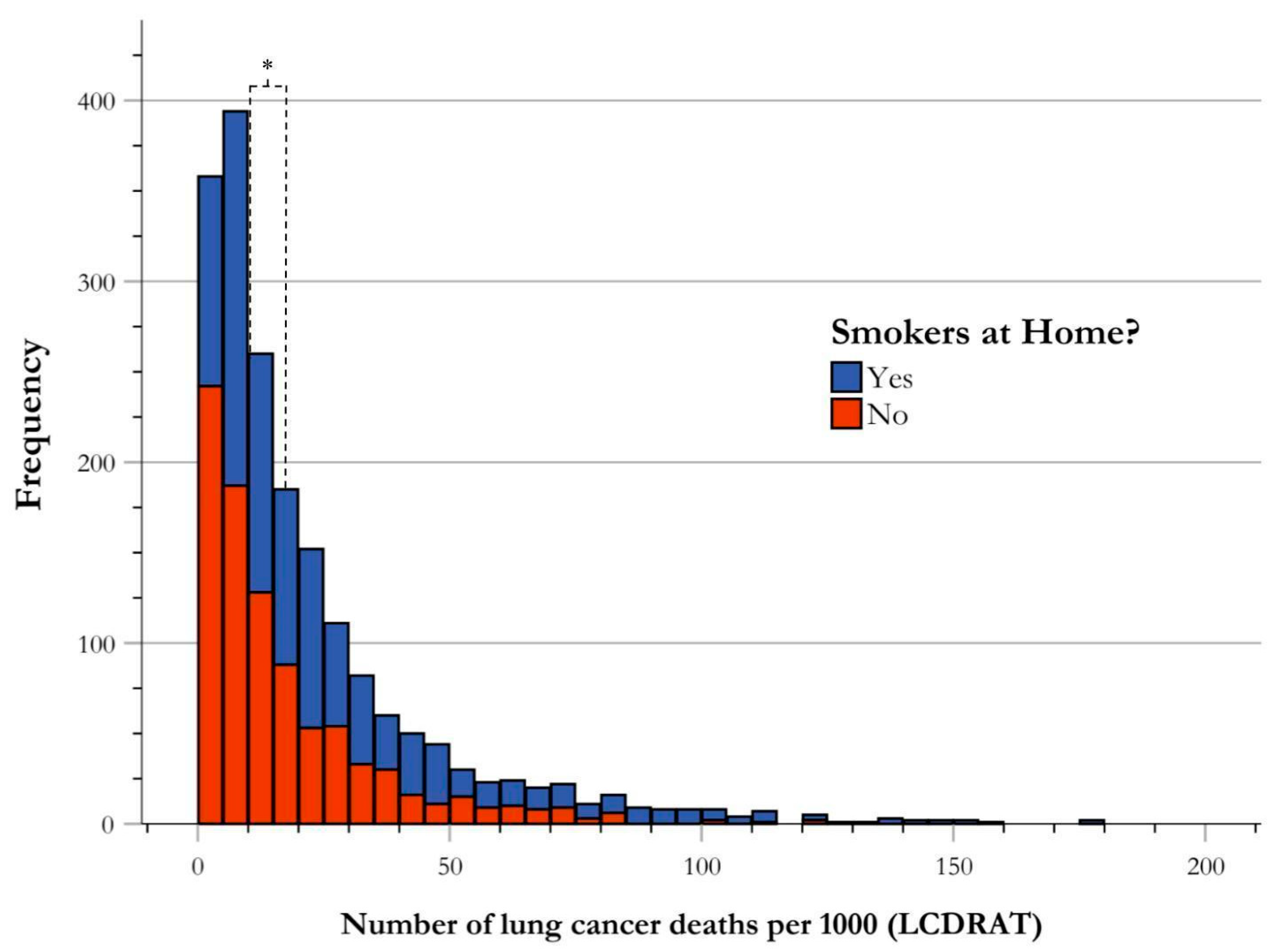
3.5. Risk of Lung Cancer Death by Secondhand Smoke Exposure
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmad, F.B.; Cisewski, J.A.; Xu, J.; Anderson, R.N. Provisional Mortality Data—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 488–492. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Haddad, D.N.; Sandler, K.L.; Henderson, L.M.; Rivera, M.P.; Aldrich, M.C. Disparities in Lung Cancer Screening: A Review. Ann. Am. Thorac. Soc. 2020, 17, 399–405. [Google Scholar] [CrossRef]
- Melamed, M.R.; Flehinger, B.J.; Zaman, M.B.; Heelan, R.T.; Perchick, W.A.; Martini, N. Screening for early lung cancer. Results of the Memorial Sloan-Kettering study in New York. Chest 1984, 86, 44–53. [Google Scholar] [CrossRef]
- Zhao, Y.R.; Xie, X.; de Koning, H.J.; Mali, W.P.; Vliegenthart, R.; Oudkerk, M. NELSON lung cancer screening study. Cancer Imaging 2011, 11, S79–S84. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, P.F.; Church, T.R.; Izmirlian, G.; Kramer, B.S. The National Lung Screening Trial: Results stratified by demographics, smoking history, and lung cancer histology. Cancer 2013, 119, 3976–3983. [Google Scholar] [CrossRef]
- United States Preventive Services Taskforce. Lung Cancer: Screening. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung-cancer-screening (accessed on 2 April 2024).
- Meza, R.; Jeon, J.; Toumazis, I.; ten Haaf, K.; Cao, P.; Bastani, M.; Han, S.S.; Blom, E.F.; Jonas, D.E.; Feuer, E.J.; et al. Evaluation of the Benefits and Harms of Lung Cancer Screening With Low-Dose Computed Tomography: Modeling Study for the US Preventive Services Task Force. JAMA 2021, 325, 988–997. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute Division of Cancer Epidemiology and Genetics. Risk-based NLST Outcomes Tool (RNOT). Available online: https://cdas.cancer.gov/nlst/ (accessed on 2 April 2024).
- Katki, H.A.; Kovalchik, S.A.; Berg, C.D.; Cheung, L.C.; Chaturvedi, A.K. Development and Validation of Risk Models to Select Ever-Smokers for CT Lung Cancer Screening. JAMA 2016, 315, 2300–2311. [Google Scholar] [CrossRef]
- American Lung Association. Available online: https://www.lung.org/lung-health-diseases/lung-disease-lookup/lung-cancer/screening-resources/state-lung-cancer-screening (accessed on 7 June 2024).
- World Trade Center Health Program. Available online: https://www.cdc.gov/wtc/fs_lung_cancer.html (accessed on 7 June 2024).
- Yale Medicine. Available online: https://www.yalemedicine.org/departments/lung-cancer-screening-program (accessed on 7 June 2024).
- USCF Health. Available online: https://www.ucsfhealth.org/clinics/lung-cancer-screening-program (accessed on 7 June 2024).
- Lin, J.J.; Mhango, G.; Wall, M.M.; Lurslurchachai, L.; Bond, K.T.; Nelson, J.E.; Berman, A.R.; Salazar-Schicchi, J.; Powell, C.; Keller, S.M.; et al. Cultural factors associated with racial disparities in lung cancer care. Ann. Am. Thorac. Soc. 2014, 11, 489–495. [Google Scholar] [CrossRef]
- Jonnalagadda, S.; Lin, J.J.; Nelson, J.E.; Powell, C.A.; Salazar-Schicchi, J.; Berman, A.R.; Keller, S.M.; Smith, C.B.; Lurslurchachai, L.; Halm, E.A.; et al. Racial and ethnic differences in beliefs about lung cancer care. Chest 2012, 142, 1251–1258. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention/National Center for Health Statistics. National Health and Nutrition Examination Survey Overview; National Center for Health Statistics: Hyattsville, MD, USA, 2022. [Google Scholar]
- National Cancer Institute Division of Cancer Epidemiology and Genetics. Lung Cancer Risk Models for Screening (R Package: Icrisks). Available online: https://dceg.cancer.gov/tools/risk-assessment/lcrisks (accessed on 2 April 2024).
- National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 7 June 2024).
- Amicizia, D.; Piazza, M.F.; Marchini, F.; Astengo, M.; Grammatico, F.; Battaglini, A.; Schenone, I.; Sticchi, C.; Lavieri, R.; Di Silverio, B.; et al. Systematic Review of Lung Cancer Screening: Advancements and Strategies for Implementation. Healthcare 2023, 11, 2085. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Liu, J.; Chen, Y.; Liu, Z.; Xia, H.; Xu, H. Gender disparities in lung cancer incidence in the United States during 2001–2019. Sci. Rep. 2023, 13, 12581. [Google Scholar] [CrossRef]
- Rogers, C.R.; Rogers, T.N.; Matthews, P.; Le Duc, N.; Zickmund, S.; Powell, W.; Thorpe, R.J., Jr.; McKoy, A.; Davis, F.A.; Okuyemi, K.; et al. Psychosocial determinants of colorectal Cancer screening uptake among African-American men: Understanding the role of masculine role norms, medical mistrust, and normative support. Ethn. Health 2022, 27, 1103–1122. [Google Scholar] [CrossRef] [PubMed]
- Mahalik, J.R.; Burns, S.M.; Syzdek, M. Masculinity and perceived normative health behaviors as predictors of men’s health behaviors. Soc. Sci. Med. 2007, 64, 2201–2209. [Google Scholar] [CrossRef]
- Hammond, W.P.; Matthews, D.; Mohottige, D.; Agyemang, A.; Corbie-Smith, G. Masculinity, medical mistrust, and preventive health services delays among community-dwelling African-American men. J. Gen. Intern. Med. 2010, 25, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Stabellini, N.; Bruno, D.S.; Dmukauskas, M.; Barda, A.J.; Cao, L.; Shanahan, J.; Waite, K.; Montero, A.J.; Barnholtz-Sloan, J.S. Sex Differences in Lung Cancer Treatment and Outcomes at a Large Hybrid Academic-Community Practice. JTO Clin. Res. Rep. 2022, 3, 100307. [Google Scholar] [CrossRef] [PubMed]
- Carter-Harris, L.; Slaven, J.E., 2nd; Monahan, P.O.; Draucker, C.B.; Vode, E.; Rawl, S.M. Understanding lung cancer screening behaviour using path analysis. J. Med. Screen 2020, 27, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.; Judd, J.; Chin, S.; Ragin, C. Disparities in Lung Cancer Treatment. Curr. Oncol. Rep. 2022, 24, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Powell, W.; Richmond, J.; Mohottige, D.; Yen, I.; Joslyn, A.; Corbie-Smith, G. Medical Mistrust, Racism, and Delays in Preventive Health Screening among African-American Men. Behav. Med. 2019, 45, 102–117. [Google Scholar] [CrossRef]
- Hardy, D.; Liu, C.C.; Xia, R.; Cormier, J.N.; Chan, W.; White, A.; Burau, K.; Du, X.L. Racial disparities and treatment trends in a large cohort of elderly black and white patients with nonsmall cell lung cancer. Cancer 2009, 115, 2199–2211. [Google Scholar] [CrossRef]
- Zhou, H.; Zhang, Y.; Liu, J.; Yang, Y.; Fang, W.; Hong, S.; Chen, G.; Zhao, S.; Zhang, Z.; Shen, J.; et al. Education and lung cancer: A Mendelian randomization study. Int. J. Epidemiol. 2019, 48, 743–750. [Google Scholar] [CrossRef] [PubMed]
- McCutchan, G.; Hiscock, J.; Hood, K.; Murchie, P.; Neal, R.D.; Newton, G.; Thomas, S.; Thomas, A.M.; Brain, K. Engaging high-risk groups in early lung cancer diagnosis: A qualitative study of symptom presentation and intervention preferences among the UK’s most deprived communities. BMJ Open 2019, 9, e025902. [Google Scholar] [CrossRef] [PubMed]
- Aslam, F.N.; Manochakian, R.; Lou, Y.; Colon-Otero, G.; Sher, T. Trends in participant race and sex reporting in lung cancer phase III clinical trials. Cancer Rep. 2023, 6 (Suppl. 1), e1856. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Omeogu, C.H.; Islam, J.Y.; Joshi, A.R.; Akinyemiju, T.F. Association of area-level socioeconomic status and non-small cell lung cancer stage by race/ethnicity and health care-level factors: Analysis of the National Cancer Database. Cancer 2022, 128, 3099–3108. [Google Scholar] [CrossRef] [PubMed]
- Leuven, E.; Plug, E.; Rønning, M. Education and cancer risk. Labour. Econ. 2016, 43, 106–121. [Google Scholar] [CrossRef]
- Hovanec, J.; Siemiatycki, J.; Conway, D.I.; Olsson, A.; Stücker, I.; Guida, F.; Jöckel, K.-H.; Pohlabeln, H.; Ahrens, W.; Brüske, I.; et al. Lung cancer and socioeconomic status in a pooled analysis of case-control studies. PLoS ONE 2018, 13, e0192999. [Google Scholar] [CrossRef] [PubMed]
- Park, E.R.; Japuntich, S.J.; Traeger, L.; Cannon, S.; Pajolek, H. Disparities between blacks and whites in tobacco and lung cancer treatment. Oncologist 2011, 16, 1428–1434. [Google Scholar] [CrossRef]
- Asomaning, K.; Miller, D.P.; Liu, G.; Wain, J.C.; Lynch, T.J.; Su, L.; Christiani, D.C. Second hand smoke, age of exposure and lung cancer risk. Lung Cancer 2008, 61, 13–20. [Google Scholar] [CrossRef]
- Avila, J.C.; Lee, S.; Osuoha, E.; Maglalang, D.D.; Sokolovsky, A.; Ahluwalia, J.S. Socioeconomic status across the life course and smoking cessation among older adult smokers in the U.S. Addict. Behav. 2022, 135, 107454. [Google Scholar] [CrossRef]
- Braun, M.; Klingelhöfer, D.; Oremek, G.M.; Quarcoo, D.; Groneberg, D.A. Influence of Second-Hand Smoke and Prenatal Tobacco Smoke Exposure on Biomarkers, Genetics and Physiological Processes in Children-An Overview in Research Insights of the Last Few Years. Int. J. Environ. Res. Public Health 2020, 17, 3212. [Google Scholar] [CrossRef]
- Ge, C.; Peters, S.; Olsson, A.; Portengen, L.; Schuz, J.; Almansa, J.; Ahrens, W.; Bencko, V.; Benhamou, S.; Boffetta, P.; et al. Diesel Engine Exhaust Exposure, Smoking, and Lung Cancer Subtype Risks. A Pooled Exposure-Response Analysis of 14 Case-Control Studies. Am. J. Respir. Crit. Care Med. 2020, 202, 402–411. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Respiratory Medicine. The world is failing on silicosis. Lancet Respir. Med. 2019, 7, 283. [Google Scholar] [CrossRef] [PubMed]
- Alspaugh, A.; Lanshaw, N.; Kriebs, J.; Van Hoover, C. Universal Health Care for the United States: A Primer for Health Care Providers. J. Midwifery Womens Health 2021, 66, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Diaz, A.; Pawlik, T.M. Insurance status and high-volume surgical cancer: Access to high-quality cancer care. Cancer 2021, 127, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Perraillon, M.C.; Myerson, R. The Impact of Medicare Health Insurance Coverage on Lung Cancer Screening. Med. Care 2022, 60, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.J.; Schlick, C.J.R.; Feinglass, J.; Mulcahy, M.F.; Benson, A.B.; Kircher, S.M.; Yang, T.D.; Odell, D.D.; Bilimoria, K.; Merkow, R.P. Failure to administer recommended chemotherapy: Acceptable variation or cancer care quality blind spot? BMJ Qual. Saf. 2020, 29, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Matthews, S.; Qureshi, N.; Levin, J.S.; Eberhart, N.K.; Breslau, J.; McBain, R.K. Financial Interventions to Improve Screening in Primary Care: A Systematic Review. Am. J. Prev. Med. 2024, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.; Bhandari, S.; Pinkston, C.; Oechsli, M.; Kloecker, G. Lung Cancer Screening Registry Reveals Low-dose CT Screening Remains Heavily Underutilized. Clin. Lung Cancer 2020, 21, e206–e211. [Google Scholar] [CrossRef] [PubMed]
- Doubeni, C.A.; Wilkinson, J.M.; Korsen, N.; Midthun, D.E. Lung Cancer Screening Guidelines Implementation in Primary Care: A Call to Action. Ann. Fam. Med. 2020, 18, 196–201. [Google Scholar] [CrossRef]
- Choi, E.; Ding, V.Y.; Luo, S.J.; ten Haaf, K.; Wu, J.T.; Aredo, J.V.; Wilkens, L.R.; Freedman, N.D.; Backhus, L.M.; Leung, A.N.; et al. Risk Model–Based Lung Cancer Screening and Racial and Ethnic Disparities in the US. JAMA Oncol. 2023, 9, 1640–1648. [Google Scholar] [CrossRef]
- Shehata, S.A.; Toraih, E.A.; Ismail, E.A.; Hagras, A.M.; Elmorsy, E.; Fawzy, M.S. Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk. Cancers 2023, 15, 4525. [Google Scholar] [CrossRef] [PubMed]
- Besaratinia, A.; Tommasi, S. Vaping epidemic: Challenges and opportunities. Cancer Causes Control 2020, 31, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Laguna, J.C.; Garcia-Pardo, M.; Alessi, J.; Barrios, C.; Singh, N.; Al-Shamsi, H.O.; Loong, H.; Ferriol, M.; Recondo, G.; Mezquita, L. Geographic differences in lung cancer: Focus on carcinogens, genetic predisposition, and molecular epidemiology. Ther. Adv. Med. Oncol. 2024, 16, 17588359241231260. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number | Percent |
|---|---|---|
| Gender | ||
| Male | 2271 | 64.1 |
| Female | 1274 | 35.9 |
| Ethnicity/Race | ||
| African American | 801 | 22.6 |
| Hispanic | 463 | 13.1 |
| Non-Hispanic White | 2017 | 56.9 |
| Other Ethnicity | 264 | 7.4 |
| Educational Attainment | ||
| <9th Grade | 440 | 12.4 |
| 9th Grade to 12th Grade | 725 | 20.5 |
| High School Graduate/GED | 984 | 27.8 |
| Some College/AA Degree | 1031 | 29.1 |
| College Graduate and above | 364 | 10.3 |
| Has a history of COPD or Emphysema * | 881 | 24.9 |
| Age in years | ||
| 50–60 | 1204 | 34 |
| 61–70 | 1389 | 39.2 |
| 71–80 | 851 | 24 |
| Body Mass Index (kg/m2) | ||
| <20 kg/m2 | 219 | 6.2 |
| 20–25 kg/m2 | 894 | 25.2 |
| 26–30 kg/m2 | 1200 | 33.9 |
| >31 kg/m2 | 1232 | 34.8 |
| Smoking History, in pack-years (py) | ||
| 20–30 py | 994 | 28 |
| 31–50 py | 1420 | 40.1 |
| 51–70 py | 638 | 18 |
| 71+ py | 493 | 13.9 |
| Variable | Description. |
|---|---|
| Age | Taken from the age at the time of screening. Variable RIDAGEYR. |
| Gender | Gender was taken from sex assigned at birth. Variable RIAGENDR. |
| Ethnicity/Race | Ethnicity/Race was obtained from participants’ asked identity. Variable RIDRETH1. |
| Educational Attainment | Educational attainment was obtained from participants’ asked education level for adults. Variable DMDEDUC2. |
| Quit years | Quit years were calculated from time since quit smoking, converted to years. Patients were asked in days, months, or years their total quit time. Variables SMQ852U for units, and SMQ852Q for total time quit. |
| Smoke Years | Smoke years were calculated from age participants regularly smoked (variable SMD030), subtracted from age at exam (variable RIDAGEYR), subtracted from quit years calculated. |
| Cigarettes per day | This was obtained from the number of cigarettes actively smoked per day (variable SMD070), or cigarettes smoked when last quit (variable SMD057). |
| COPD or emphysema history | COPD or emphysema history was acquired from questions in the medical conditions section of the NHANES database; questions asked if participant was ever told they had a history of COPD, emphysema, or chronic bronchitis; compiled from variables MCQ160G, MCQ160K, MCQ160O, and MCQ160P. |
| Body Mass Index (BMI) | Body mass index in kg/m2, taken from the NHANES variable BMXBMI. |
| Ethnicity/Race | Significance | Adjusted Significance * |
|---|---|---|
| Non-Hispanic White vs. Hispanic | p < 0.001 | p < 0.001 |
| Non-Hispanic White vs. African American | p = 0.002 | p = 0.013 |
| Hispanic vs. Other Race | p = 0.951 | p = 1.000 |
| Education Level | ||
| <9th grade vs. 9th–12th grade | p = 0.006 | p = 0.008 |
| 9th–12th grade vs. High School Graduate/GED | p < 0.001 | p < 0.001 |
| High School Graduate/GED vs. Some College or AA Degree | p < 0.001 | p < 0.001 |
| Some College or AA Degree vs. College Graduate and Above | p = 0.586 | p = 0.586 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tieu, V.; MacDowell, S.; Tibi, S.; Ventayen, B.; Agarwal, M. Identifying Populations at Risk for Lung Cancer Mortality from the National Health and Nutrition Examination Survey (2001–2018) Using the 2021 USPSTF Screening Guidelines. Int. J. Environ. Res. Public Health 2024, 21, 781. https://doi.org/10.3390/ijerph21060781
Tieu V, MacDowell S, Tibi S, Ventayen B, Agarwal M. Identifying Populations at Risk for Lung Cancer Mortality from the National Health and Nutrition Examination Survey (2001–2018) Using the 2021 USPSTF Screening Guidelines. International Journal of Environmental Research and Public Health. 2024; 21(6):781. https://doi.org/10.3390/ijerph21060781
Chicago/Turabian StyleTieu, Vivian, Samuel MacDowell, Sedra Tibi, Bradley Ventayen, and Mukesh Agarwal. 2024. "Identifying Populations at Risk for Lung Cancer Mortality from the National Health and Nutrition Examination Survey (2001–2018) Using the 2021 USPSTF Screening Guidelines" International Journal of Environmental Research and Public Health 21, no. 6: 781. https://doi.org/10.3390/ijerph21060781
APA StyleTieu, V., MacDowell, S., Tibi, S., Ventayen, B., & Agarwal, M. (2024). Identifying Populations at Risk for Lung Cancer Mortality from the National Health and Nutrition Examination Survey (2001–2018) Using the 2021 USPSTF Screening Guidelines. International Journal of Environmental Research and Public Health, 21(6), 781. https://doi.org/10.3390/ijerph21060781