
A Randomized Clinical Trial of a Quitline Vaping Cessation Intervention: Baseline Characteristics of Young Adult Exclusive E-Cigarette Users Seeking Treatment


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
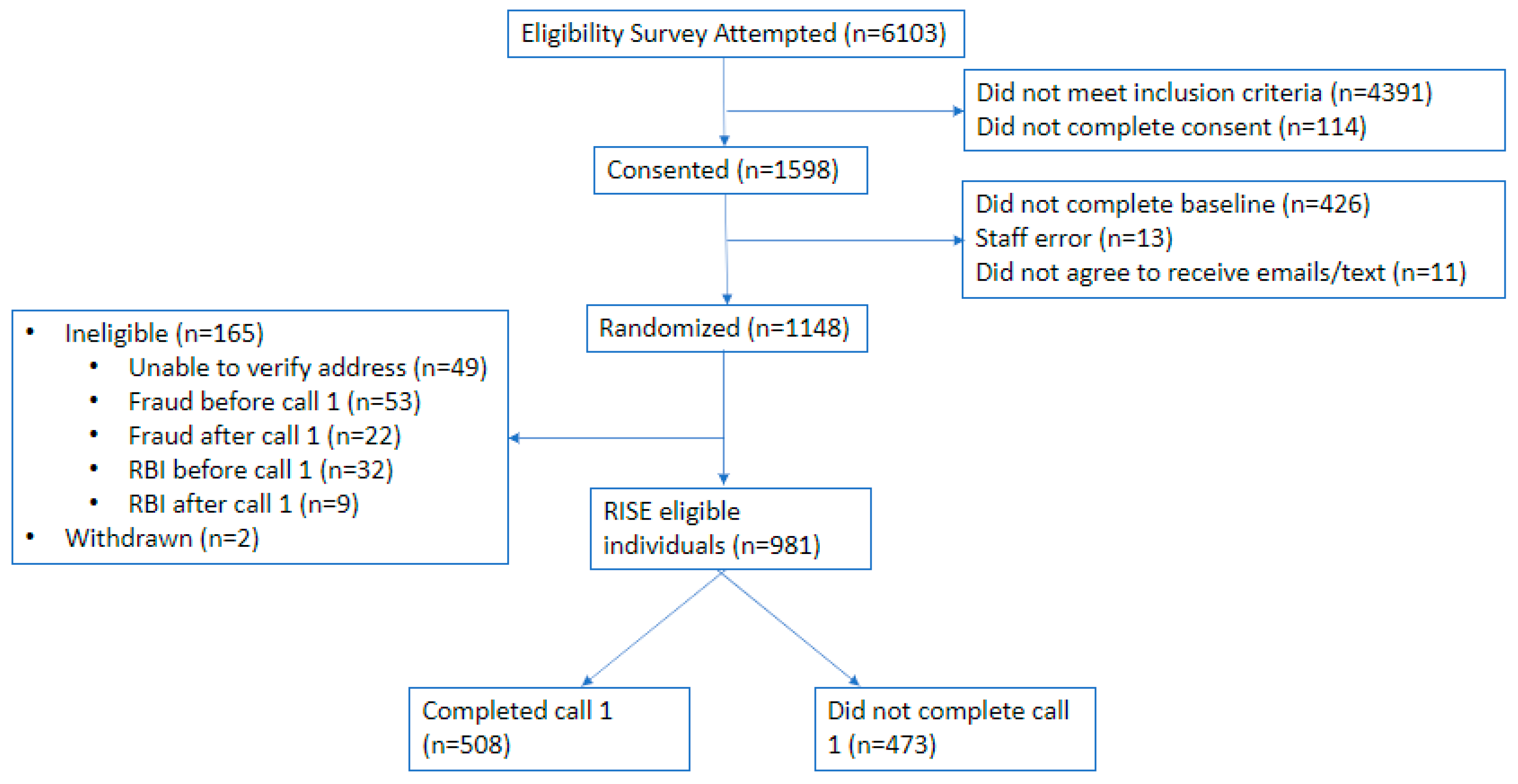
2.2. Procedures
2.3. Measures
2.4. Analysis
3. Results
3.1. Demographic Comparisons
3.2. Behavioral Health Comparisons
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boakye, E.; Osuji, N.; Erhabor, J.; Obisesan, O.; Osei, A.D.; Mirbolouk, M.; Stokes, A.C.; Dzaye, O.; El Shahawy, O.; Hirsch, G.A. Assessment of Patterns in E-Cigarette use among Adults in the US, 2017–2020. JAMA Netw. Open 2022, 5, e2223266. [Google Scholar] [CrossRef]
- Obisesan, O.H.; Osei, A.D.; Uddin, S.M.I.; Dzaye, O.; Mirbolouk, M.; Stokes, A.; Blaha, M.J. Trends in E-Cigarette use in Adults in the United States, 2016–2018. JAMA Intern. Med. 2020, 180, 1394–1398. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Leventhal, A.M. Prevalence of E-Cigarette use among Adults in the United States, 2014–2018. JAMA 2019, 322, 1824–1827. [Google Scholar] [CrossRef] [PubMed]
- Kramarow, E.A.; Elgaddal, N. Current Electronic Cigarette use among Adults Aged 18 and Over: United States, 2021. Natl. Cent. Health Stat. 2023, 475, 129966. [Google Scholar]
- Mok, Y.; Jeon, J.; Levy, D.T.; Meza, R. Associations between E-Cigarette use and E-Cigarette Flavors with Cigarette Smoking Quit Attempts and Quit Success: Evidence from a US Large, Nationally Representative 2018–2019 Survey. Nicotine Tob. Res. 2023, 25, 541–552. [Google Scholar] [CrossRef]
- Cuccia, A.F.; Patel, M.; Amato, M.S.; Stephens, D.K.; Yoon, S.N.; Vallone, D.M. Quitting E-Cigarettes: Quit Attempts and Quit Intentions among Youth and Young Adults. Prev. Med. Rep. 2021, 21, 101287. [Google Scholar] [CrossRef] [PubMed]
- Graham, A.L.; Jacobs, M.A.; Amato, M.S. Engagement and 3-Month Outcomes from a Digital E-Cigarette Cessation Program in a Cohort of 27 000 Teens and Young Adults. Nicotine Tob. Res. 2020, 22, 859–860. [Google Scholar] [CrossRef]
- Berg, C.J.; Krishnan, N.; Graham, A.L.; Abroms, L.C. A Synthesis of the Literature to Inform Vaping Cessation Interventions for Young Adults. Addict. Behav. 2021, 119, 106898. [Google Scholar] [CrossRef]
- Villanti, A.C.; West, J.C.; Klemperer, E.M.; Graham, A.L.; Mays, D.; Mermelstein, R.J.; Higgins, S.T. Smoking-Cessation Interventions for U.S. Young Adults: Updated Systematic Review. Am. J. Prev. Med. 2020, 59, 123–136. [Google Scholar] [CrossRef]
- Sanchez, S.; Kaufman, P.; Pelletier, H.; Baskerville, B.; Feng, P.; O’Connor, S.; Schwartz, R.; Chaiton, M. Is Vaping Cessation Like Smoking Cessation? A Qualitative Study Exploring the Responses of Youth and Young Adults Who Vape E-Cigarettes. Addict. Behav. 2021, 113, 106687. [Google Scholar] [CrossRef]
- Graham, A.L.; Cha, S.; Papandonatos, G.D.; Amato, M.S.; Jacobs, M.A.; Abroms, L.C.; Berg, C.J. E-Cigarette and Combusted Tobacco Abstinence among Young Adults: Secondary Analyses from a US-Based Randomized Controlled Trial of Vaping Cessation. Prev. Med. 2022, 165 Pt B, 107119. [Google Scholar] [CrossRef]
- Abdoli, N.; Sadeghi-Bahmani, D.; Salari, N.; Khodamoradi, M.; Farnia, V.; Jahangiri, S.; Brühl, A.B.; Dürsteler, K.M.; Stanga, Z.; Brand, S. Nomophobia (no Mobile Phone Phobia) and Psychological Health Issues among Young Adult Students. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1762–1775. [Google Scholar] [CrossRef] [PubMed]
- Dias, J. Gen Z Developing Fear of Phone Calls, or “Phone Phobia”. Available online: https://www.cbsnews.com/newyork/news/gen-z-developing-fear-of-phone-calls-or-phone-phobia/ (accessed on 24 January 2024).
- U.S. Department of Health and Human Services. E-Cigarette use among Youth and Young Adults: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2016. [Google Scholar]
- Fiore, M.C.; Jaén, C.R. A Clinical Blueprint to Accelerate the Elimination of Tobacco Use. JAMA 2008, 299, 2083–2085. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. End Nicotine Addiction in Children and Teens (ENACT); American Heart Association: Dallas, TX, USA, 2020. [Google Scholar]
- Palmer, A.M.; Price, S.N.; Foster, M.G.; Sanford, B.T.; Fucito, L.M.; Toll, B.A. Urgent Need for Novel Investigations of Treatments to Quit E-Cigarettes: Findings from a Systematic Review. Cancer Prev. Res. 2022, 15, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Hollis, J.F.; McAfee, T.A.; Fellows, J.L.; Zbikowski, S.M.; Stark, M.; Riedlinger, K. The Effectiveness and Cost Effectiveness of Telephone Counselling and the Nicotine Patch in a State Tobacco Quitline. Tob. Control 2007, 16, i53–i59. [Google Scholar] [CrossRef] [PubMed]
- Orleans, C.T.; Schoenbach, V.J.; Wagner, E.H.; Quade, D.; Salmon, M.A.; Pearson, D.C.; Fiedler, J.; Porter, C.Q.; Kaplan, B.H. Self-Help Quit Smoking Interventions: Effects of Self-Help Materials, Social Support Instructions, and Telephone Counseling. J. Consult. Clin. Psychol. 1991, 59, 439. [Google Scholar] [CrossRef] [PubMed]
- Hartmann-Boyce, J. Telephone Counselling for Smoking Cessation. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019. [Google Scholar]
- Zhu, S.; Anderson, C.M.; Tedeschi, G.J.; Rosbrook, B.; Johnson, C.E.; Byrd, M.; Gutiérrez-Terrell, E. Evidence of Real-World Effectiveness of a Telephone Quitline for Smokers. N. Engl. J. Med. 2002, 347, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services National Institutes of Health, National Institute on Drug Abuse; United States Department of Health and Human Services, Food and Drug Administration, Center for Tobacco Products. Population Assessment of Tobacco and Health (PATH) Study [United States] Restricted-Use Files; The National Addiction & HIV Data Archive Program: Ann Arbor, MI, USA, 2023. [Google Scholar]
- Hamilton, C.M.; Strader, L.C.; Pratt, J.G.; Maiese, D.; Hendershot, T.; Kwok, R.K.; Hammond, J.A.; Huggins, W.; Jackman, D.; Pan, H. The PhenX Toolkit: Get the most from Your Measures. Am. J. Epidemiol. 2011, 174, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Westat. Final Adult Interview Wave 7. 2021, 2022. Available online: https://www.icpsr.umich.edu (accessed on 25 July 2023).
- Ramo, D.E.; Hall, S.M.; Prochaska, J.J. Reliability and Validity of Self-Reported Smoking in an Anonymous Online Survey with Young Adults. Health Psychol. 2011, 30, 693–701. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Staples, L.G.; Dear, B.F.; Gandy, M.; Fogliati, V.; Fogliati, R.; Karin, E.; Nielssen, O.; Titov, N. Psychometric Properties and Clinical Utility of Brief Measures of Depression, Anxiety, and General Distress: The PHQ-2, GAD-2, and K-6. Gen. Hosp. Psychiatry 2019, 56, 13–18. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Greenland, S.; Senn, S.J.; Rothman, K.J.; Carlin, J.B.; Poole, C.; Goodman, S.N.; Altman, D.G. Statistical Tests, p Values, Confidence Intervals, and Power: A Guide to Misinterpretations. Eur. J. Epidemiol. 2016, 31, 337–350. [Google Scholar] [CrossRef]
- Foulds, J.; Veldheer, S.; Yingst, J.; Hrabovsky, S.; Wilson, S.J.; Nichols, T.T.; Eissenberg, T. Development of a Questionnaire for Assessing Dependence on Electronic Cigarettes among a Large Sample of Ex-Smoking E-Cigarette Users. Nicotine Tob. Res. 2015, 17, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Patient-Reported Outcomes Measurement Information System. PROMIS Nicotine Dependence Scoring Manual. 2023. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4189402/ (accessed on 24 January 2024).
- Dwyer, J.B.; McQuown, S.C.; Leslie, F.M. The Dynamic Effects of Nicotine on the Developing Brain. Pharmacol. Ther. 2009, 122, 125–139. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Bashar, M.A.; Srivastava, A.; Singh, A. Nomophobia: No Mobile Phone Phobia. J. Fam. Med. Prim. Care 2019, 8, 1297–1300. [Google Scholar] [CrossRef] [PubMed]
- Vickerman, K.A.; Carpenter, K.M.; Raskob, M.K.; Nash, C.M.; Vargas-Belcher, R.A.; Beebe, L.A. Vaping and E-Cigarettes within the Evolving Tobacco Quitline Landscape. Am. J. Prev. Med. 2021, 60, S142–S153. [Google Scholar] [CrossRef]
- Boal, A.L.; Abroms, L.C.; Simmens, S.; Graham, A.L.; Carpenter, K.M. Combined Quitline Counseling and Text Messaging for Smoking Cessation: A Quasi-Experimental Evaluation. Nicotine Tob. Res. 2016, 18, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- The Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A Clinical Practice Guideline for Treating Tobacco use and Dependence: 2008 Update: A U.S. Public Health Service Report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar] [CrossRef]
- Colston, D.C.; Cruz, J.L.; Simard, B.J.; Fleischer, N.L. A Systematic Review Evaluating Disparities in State-Run Quitline Utilization and Effectiveness in the United States. AJPM Focus 2023, 2, 100042. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014. [Google Scholar]
- Amato, M.S.; Bottcher, M.M.; Cha, S.; Jacobs, M.A.; Pearson, J.L.; Graham, A.L. “It’s Really Addictive and I’m Trapped:” A Qualitative Analysis of the Reasons for Quitting Vaping among Treatment-Seeking Young People. Addict. Behav. 2021, 112, 106599. [Google Scholar] [CrossRef]
- Glasser, A.M.; Hinton, A.; Wermert, A.; Macisco, J.; Nemeth, J.M. Characterizing Tobacco and Marijuana use among Youth Combustible Tobacco Users Experiencing Homelessness–considering Product Type, Brand, Flavor, Frequency, and Higher-Risk use Patterns and Predictors. BMC Public Health 2022, 22, 820. [Google Scholar] [CrossRef]
- Ramo, D.E.; Liu, H.; Prochaska, J.J. Tobacco and Marijuana use among Adolescents and Young Adults: A Systematic Review of their Co-Use. Clin. Psychol. Rev. 2012, 32, 105–121. [Google Scholar] [CrossRef]
- Roberts, M.E.; Tackett, A.P.; Singer, J.M.; Wagner, D.D.; Lu, B.; Wagener, T.L.; Brinkman, M.; Klein, E.G.; Vickerman, K.A.; Wold, L.E. Dual use of E-Cigarettes and Cannabis among Young People in America: A New Public Health Hurdle? J. Stud. Alcohol Drugs 2022, 83, 768–770. [Google Scholar] [CrossRef]
- Bennett, M.; Speer, J.; Taylor, N.; Alexander, T. Changes in E-Cigarette use among Youth and Young Adults during the COVID-19 Pandemic: Insights into Risk Perceptions and Reasons for Changing use Behavior. Nicotine Tob. Res. 2023, 25, 350–355. [Google Scholar] [CrossRef]
- Heffner, J.L.; Watson, N.L.; Dahne, J.; Croghan, I.; Kelly, M.M.; McClure, J.B.; Bars, M.; Thrul, J.; Meier, E. Recognizing and Preventing Participant Deception in Online Nicotine and Tobacco Research Studies: Suggested Tactics and a Call to Action. Nicotine Tob. Res. 2021, 23, 1810–1812. [Google Scholar] [CrossRef] [PubMed]
- Solomon, L.J.; Hughes, J.R.; Livingston, A.; Naud, S.; Callas, P.W.; Peters, E.N.; Kamon, J.; Etter, J. Cognitive Barriers to Calling a Smoking Quitline. Nicotine Tob. Res. 2009, 11, 1339–1346. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Demographics | Participants (n = 508) | Non-Participants (n = 473) | Total (n = 981) |
|---|---|---|---|
| Age | |||
| 18–21 | 57.1% (290) | 52.2% (247) | 54.7% (537) |
| 22–24 | 42.9% (218) | 47.8% (226) | 45.3% (444) |
| Gender | |||
| Female | 71.3% (362) | 74.0% (350) | 72.6% (712) |
| Male | 24.8% (126) | 22.4% (106) | 23.7% (232) |
| Transgender female | 0.2% (1) | 0.6% (3) | 0.4% (4) |
| Transgender male | 2.0% (10) | 1.5% (7) | 1.7% (17) |
| Other Identity | 1.8% (9) | 1.5% (7) | 1.6% (16) |
| Race | |||
| Caucasian (only) | 69.0% (350) | 71.1% (334) | 70.0% (684) |
| Black/African (only) | 8.5% (43) | 9.6% (45) | 9.0% (88) |
| Hispanic/Latinx (only) | 9.5% (48) | 7.5% (35) | 8.5% (83) |
| All others | 13.0% (66) | 11.9% (56) | 12.5% (122) |
| Education | |||
| ≤High school graduate | 15.1% (76) | 17.2% (81) | 16.1% (157) |
| Some college/vocational training | 59.3% (299) | 55.3% (260) | 57.4% (559) |
| ≥College graduate | 25.6% (129) | 27.5% (129) | 26.5% (258) |
| Participants (n = 508) | Non-Participants (n = 473) | Total (n = 981) | |
|---|---|---|---|
| EC use | |||
| 30 out of 30 days | 77.9% (395) | 77.4% (366) | 77.7% (761) |
| <every day | 22.1% (112) | 22.6% (107) | 22.4% (219) |
| EC use duration | |||
| 12 months or more | 86.4% (439) | 87.3% (413) | 86.9% (852) |
| 6–12 months | 6.9% (35) | 6.6% (31) | 6.7% (66) |
| <6 months | 6.7% (34) | 6.1% (29) | 6.4% (63) |
| Type of EC device | |||
| Disposable | 61.0% (303) | 53.9% (252) | 57.5% (555) |
| Buy pre-filled cartridges | 22.5% (112) | 28.6% (134) | 25.5% (246) |
| Refill independently | 16.5% (82) | 17.5% (82) | 17.0% (164) |
| Penn State Dependence scale | |||
| Missing | 19.7% (100) | 22.8% (108) | 21.2% (208) |
| 0–3 (not dependent) | 0 (0%) | 0 (0%) | 0 (0%) |
| 4–8 (low) | 5.9% (24) | 7.7% (28) | 6.7% (52) |
| 9–12 (medium) | 22.3% (91) | 22.5% (82) | 22.4% (173) |
| 13+ (high) | 71.8% (293) | 69.9% (255) | 70.95 (548) |
| PROMIS-E | |||
| T-scores | 58.6 (8.3) | 58.6 (8.6) | 58.6 (8.5) |
| Missing | 2.2% (11) | 2.1% (10) | 2.1% (21) |
| Motivation to quit scale (with 10 rated as highly likely) | 7.8 (1.7) | 7.7 (1.8) | 7.8 (1.7) |
| Reasons for quitting | |||
| Freedom from addiction | 91.1% (463) | 86.3% (408) | 88.8% (871) |
| Health concerns | 87.8% (446) | 87.3% (413) | 87.6% (859) |
| Cost | 74.2% (377) | 72.5% (343) | 73.4% (720) |
| Others’ impression | 36.6% (186) | 35.1% (166) | 35.9% (352) |
| Other reasons | 7.8% (40) | 7.0% (33) | 7.4% (73) |
| Ever try to quit vaping | 88.1% (446) | 86.5% (405) | 87.4% (851) |
| Previous quit attempts | |||
| 1–2 | 34.2% (150) | 37.4% (150) | 35.7% (300) |
| 3–4 | 41.5% (182) | 42.6% (171) | 42.0% (353) |
| 5+ | 24.4% (107) | 20.0% (80) | 22.3% (187) |
| Longest EC abstinence | |||
| <24 h | 10.2% (52) | 12.7% (60) | 11.4% (112) |
| 1–6 days | 35.1% (178) | 39.5% (186) | 37.2% (364) |
| 7–30 days | 20.7% (105) | 17.8% (84) | 19.3% (189) |
| 1–3 months | 16.5% (84) | 11.2% (53) | 14.0% (137) |
| >3 months | 17.5% (89) | 18.9% (89) | 18.2% (178) |
| Ever use of any aid to quit vaping | 30.5% (155) | 32.6% (154) | 31.5% (309) |
| Ever use of nicotine replacement therapy (NRT) to quit vaping | 28.2% (143) | 30.4% (144) | 29.3% (287) |
| Current cessation aid use | |||
| Any cessation aid | 5.5% (28) | 9.7% (46) | 7.5% (74) |
| Patch | 1.2% (6) | 3.2% (15) | 2.1% (21) |
| Gum | 2.2% (11) | 4.4% (21) | 3.3% (32) |
| Lozenge | 2.0% (10) | 2.3% (11) | 2.1% (21) |
| Any NRT (P/G/L) | 3.7% (19) | 6.8% (32) | 5.2% (51) |
| Participants (n = 508) | Non-Participants (n = 473) | Total (n = 981) | |
|---|---|---|---|
| PHQ-2 ≥ 3 (depression) | 42.9% (218) | 46.7% (221) | 44.8% (439) |
| GAD-2 ≥ 3 (anxiety) | 52.0% (264) | 59.0% (279) | 55.4% (543) |
| PSS-4 ≥ 6 (stress) | 73.0% (371) | 73.2% (346) | 73.1% (717) |
| Any alcohol use in the past month | |||
| None (0 days) | 18.5% (93) | 20.1% (94) | 19.2% (187) |
| 1–2 days | 25.0% (126) | 18.6% (87) | 21.9% (213) |
| 3–5 days | 21.2% (107) | 24.8% (116) | 22.9% (223) |
| 6–9 days | 17.9% (90) | 18.2% (85) | 18.0% (175) |
| 10+ days | 17.5% (88) | 18.4% (86) | 17.9% (174) |
| Frequency of binge drinking in the past month | |||
| None (0 days) | 43.7% (221) | 41.1% (193) | 42.4% (414) |
| 1–2 days | 29.3% (148) | 27.5% (129) | 28.4% (277) |
| 3–5 days | 14.2% (72) | 17.2% (81) | 15.7% (153) |
| 6–9 days | 7.9% (40) | 8.5% (40) | 8.2% (80) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, E.G.; Shoben, A.B.; Carpenter, K.M.; Mullis, K.; Nemeth, J.M.; Mayers, E.; Vickerman, K.A. A Randomized Clinical Trial of a Quitline Vaping Cessation Intervention: Baseline Characteristics of Young Adult Exclusive E-Cigarette Users Seeking Treatment. Int. J. Environ. Res. Public Health 2024, 21, 809. https://doi.org/10.3390/ijerph21060809
Klein EG, Shoben AB, Carpenter KM, Mullis K, Nemeth JM, Mayers E, Vickerman KA. A Randomized Clinical Trial of a Quitline Vaping Cessation Intervention: Baseline Characteristics of Young Adult Exclusive E-Cigarette Users Seeking Treatment. International Journal of Environmental Research and Public Health. 2024; 21(6):809. https://doi.org/10.3390/ijerph21060809
Chicago/Turabian StyleKlein, Elizabeth G., Abigail B. Shoben, Kelly M. Carpenter, Kristina Mullis, Julianna M. Nemeth, Elizabeth Mayers, and Katrina A. Vickerman. 2024. "A Randomized Clinical Trial of a Quitline Vaping Cessation Intervention: Baseline Characteristics of Young Adult Exclusive E-Cigarette Users Seeking Treatment" International Journal of Environmental Research and Public Health 21, no. 6: 809. https://doi.org/10.3390/ijerph21060809
APA StyleKlein, E. G., Shoben, A. B., Carpenter, K. M., Mullis, K., Nemeth, J. M., Mayers, E., & Vickerman, K. A. (2024). A Randomized Clinical Trial of a Quitline Vaping Cessation Intervention: Baseline Characteristics of Young Adult Exclusive E-Cigarette Users Seeking Treatment. International Journal of Environmental Research and Public Health, 21(6), 809. https://doi.org/10.3390/ijerph21060809