
Treating Mental Health and Quality of Life in Older Cancer Patients with Cognitive Behavioral Therapy: A Systematic Review and Meta-Analysis

 and
and
Abstract
1. Introduction
2. Materials and Methods
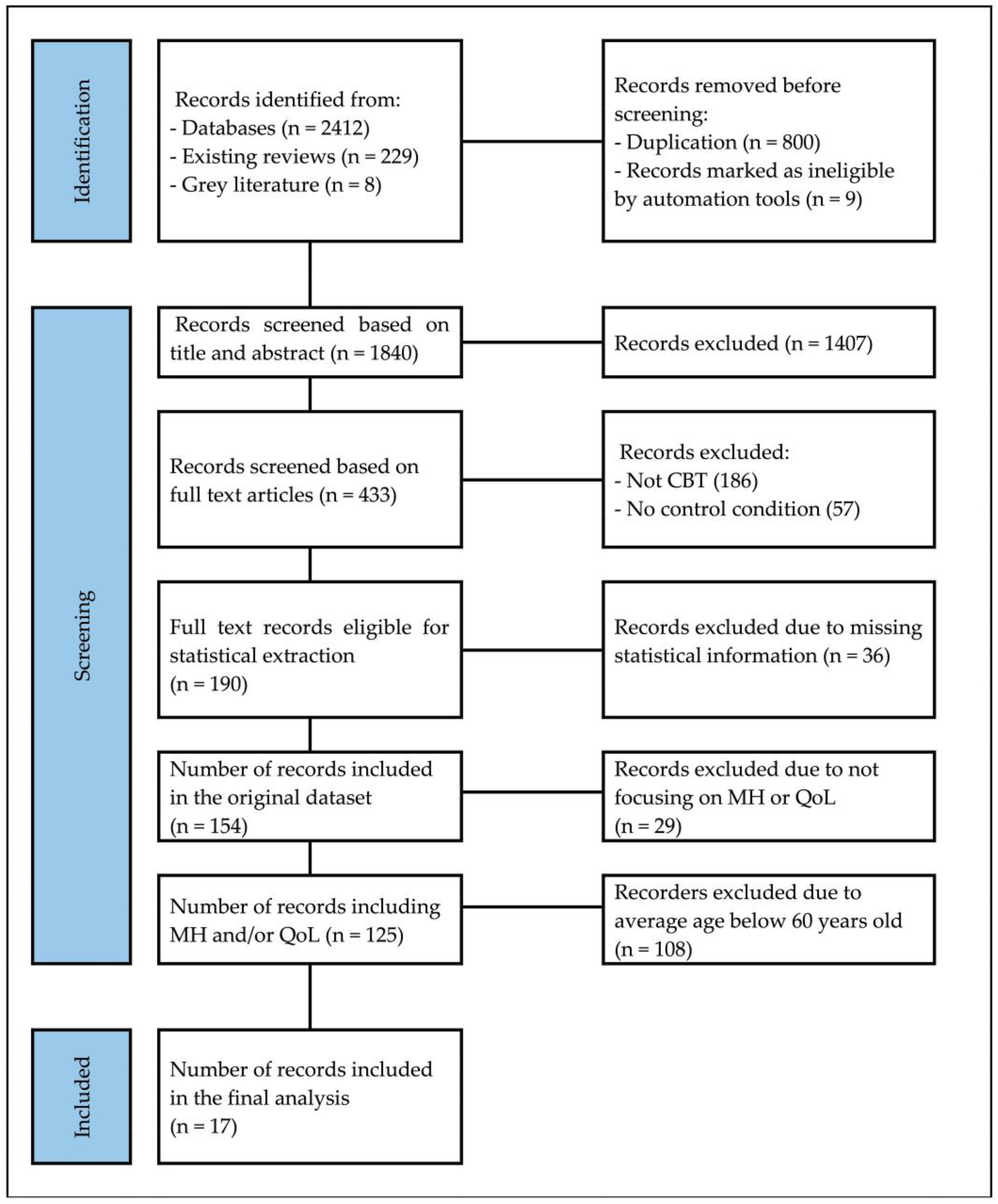
2.1. Search Procedures and Inclusion Criteria
2.2. Population, Intervention, and Outcome Measures
2.3. Data Extraction
2.4. Meta-Analytic Procedures
3. Results
3.1. Study Characteristics
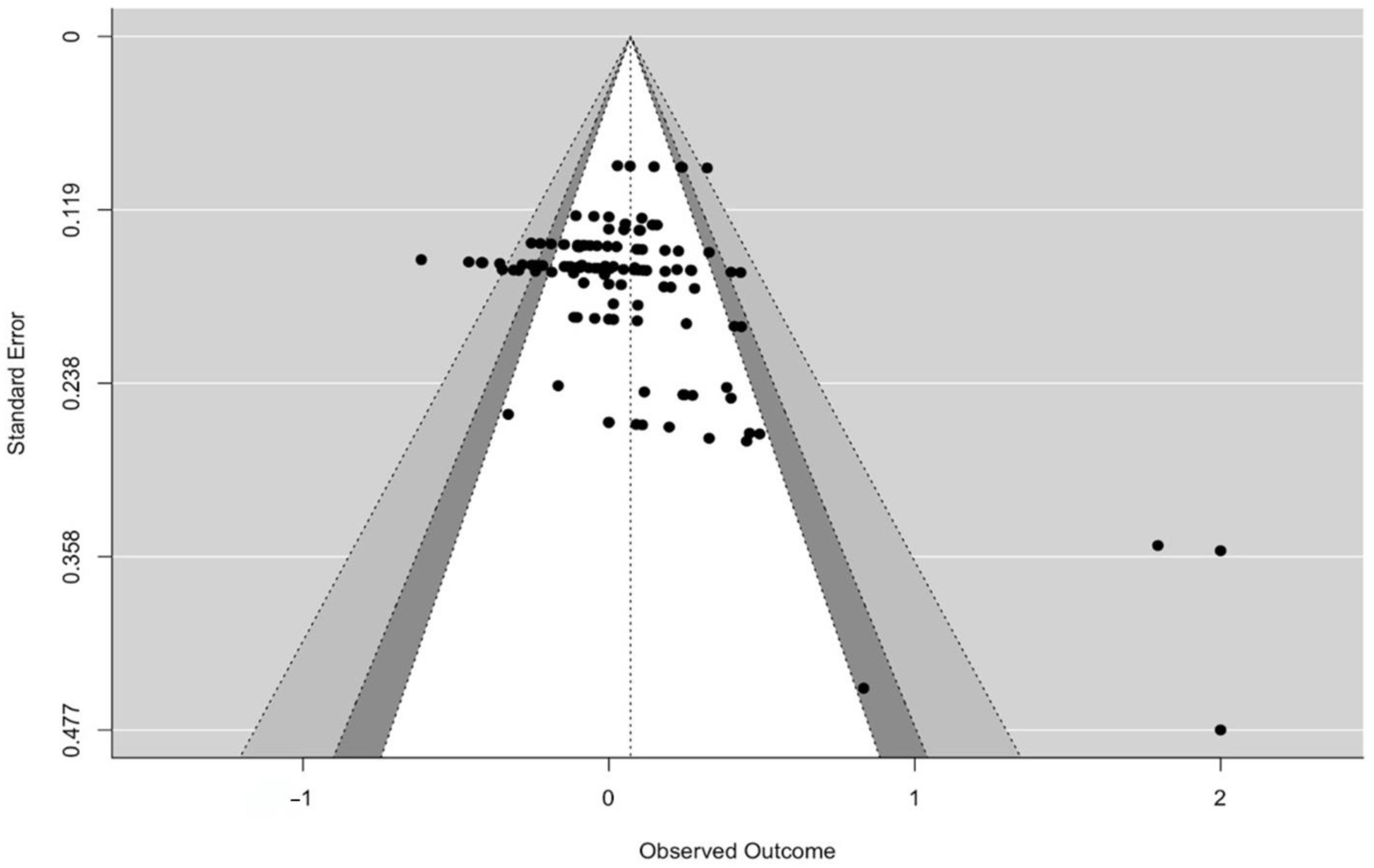
3.2. Publication Bias
3.3. Risk of Bias
3.4. Meta-Analytic Results
3.5. Moderator Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- National Cancer Institute. Age and Cancer Risk. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age (accessed on 27 May 2024).
- Hoffe, S.; Balducci, L. Cancer and age: General considerations. Clin. Geriatr. Med. 2012, 28, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Grassi, L.; Spiegel, D.; Riba, M. Advancing psychosocial care in cancer patients. F1000Research 2017, 6, 2083. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.; Suleman, S.; Hyde, N.; Hodgkiss, A. Depression and anxiety in patients with cancer. BMJ 2018, 361, k1415. [Google Scholar] [CrossRef] [PubMed]
- Tauber, N.M.; O’Toole, M.S.; Dinkel, A.; Galica, J.; Humphris, G.; Lebel, S.; Maheu, C.; Ozakinci, G.; Prins, J.; Sharpe, L.; et al. Effect of Psychological Intervention on Fear of Cancer Recurrence: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2019, 37, 2899–2915. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Weaver, A.; Walling, E.; Zebrack, B.; Jackson Levin, N.; Stuchell, B.; Himle, J. Evaluating an engaging and coach-assisted online cognitive behavioral therapy for depression among adolescent and young adult cancer survivors: A pilot feasibility trial. J. Psychosoc. Oncol. 2023, 41, 20–42. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.; Sawyer, A.T.; Fang, A. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Bártolo, A.; Santos, I.M.; Pereira, A.; Monteiro, S. Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 3424. [Google Scholar] [CrossRef]
- Kishita, N.; Laidlaw, K. Cognitive behaviour therapy for generalized anxiety disorder: Is CBT equally efficacious in adults of working age and older adults? Clin. Psychol. Rev. 2017, 52, 124–136. [Google Scholar] [CrossRef]
- Werson, A.D.; Meiser-Stedman, R.; Laidlaw, K. A meta-analysis of CBT efficacy for depression comparing adults and older adults. J. Affect. Disord. 2022, 319, 189–201. [Google Scholar] [CrossRef]
- Laidlaw, K. A deficit in psychotherapeutic care for older people with depression and anxiety. Gerontology 2013, 59, 549–556. [Google Scholar] [CrossRef]
- Areán, P.A.; Alvidrez, J.; Barrera, A.; Robinson, G.S.; Hicks, S. Would older medical patients use psychological services? Gerontologist 2002, 42, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, C.S.; Scott, T.; Mather, A.; Sareen, J. Older adults’ help-seeking attitudes and treatment beliefs concerning mental health problems. Am. J. Geriatr. Psychiatry 2008, 16, 1010–1019. [Google Scholar] [CrossRef] [PubMed]
- Greer, J.A.; Jacobs, J.; Pensak, N.; MacDonald, J.J.; Fuh, C.X.; Perez, G.K.; Ward, A.; Tallen, C.; Muzikansky, A.; Traeger, L.; et al. Randomized Trial of a Tailored Cognitive-Behavioral Therapy Mobile Application for Anxiety in Patients with Incurable Cancer. Oncologist 2019, 24, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Espie, C.A.; Fleming, L.; Cassidy, J.; Samuel, L.; Taylor, L.M.; White, C.A.; Douglas, N.J.; Engleman, H.M.; Kelly, H.L.; Paul, J. Randomized controlled clinical effectiveness trial of cognitive behavior therapy compared with treatment as usual for persistent insomnia in patients with cancer. J. Clin. Oncol. 2008, 26, 4651–4658. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, C.; Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Efficacy of cognitive-behavioral therapy for insomnia in women treated for nonmetastatic breast cancer. J. Consult. Clin. Psychol. 2003, 71, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Randomized study on the efficacy of cognitive-behavioral therapy for insomnia secondary to breast cancer, part I: Sleep and psychological effects. J. Clin. Oncol. 2005, 23, 6083–6096. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing and health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 27 May 2024).
- Srivastava, S.; Sulaiman, K.M.; Drishti, D.; Muhammad, T. Factors associated with psychiatric disorders and treatment seeking behaviour among older adults in India. Sci. Rep. 2021, 11, 24085. [Google Scholar] [CrossRef] [PubMed]
- Schaun, G.Z.; Bamman, M.M.; Andrade, L.S.; David, G.B.; Krüger, V.L.; Marins, E.F.; Nunes, G.N.; Häfele, M.S.; Mendes, G.F.; Gomes, M.L.B.; et al. High-velocity resistance training mitigates physiological and functional impairments in middle-aged and older adults with and without mobility-limitation. Geroscience 2022, 44, 1175–1197. [Google Scholar] [CrossRef] [PubMed]
- Lachman, M.E. Adult Development, Psychology of. In International Encyclopedia of the Social & Behavioral Sciences; Smelser, N.J., Baltes, P.B., Eds.; Pergamon: Oxford, UK, 2001; pp. 135–139. [Google Scholar]
- Zhang, H.; Cheng, P.; Huang, L. The Impact of the Medical Insurance System on the Health of Older Adults in Urban China: Analysis Based on Three-Period Panel Data. Int. J. Environ. Res. Public. Health 2023, 20, 3817. [Google Scholar] [CrossRef]
- Singh, S.; Bajorek, B. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm. Pr. 2014, 12, 489. [Google Scholar] [CrossRef]
- The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, NY, USA, 2019.
- Hedges, L.V.; Tipton, E.; Johnson, M.C. Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 2010, 1, 39–65. [Google Scholar] [CrossRef] [PubMed]
- Tipton, E.; Pustejovsky, J.E. Small-Sample Adjustments for Tests of Moderators and Model Fit Using Robust Variance Estimation in Meta-Regression. J. Educ. Behav. Stat. 2015, 40, 604–634. [Google Scholar] [CrossRef]
- Publication Bias in Research Synthesis: Sensitivity Analysis Using A Priori Weight Functions. Psychol. Methods 2005, 10, 428–443. [CrossRef] [PubMed]
- Hall, J.; Kellett, S.; Berrios, R.; Bains, M.K.; Scott, S. Efficacy of Cognitive Behavioral Therapy for Generalized Anxiety Disorder in Older Adults: Systematic Review, Meta-Analysis, and Meta-Regression. Am. J. Geriatr. Psychiatry 2016, 24, 1063–1073. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.C.; Byrne, G.J. Interventions for generalized anxiety disorder in older adults: Systematic review and meta-analysis. J. Anxiety Disord. 2012, 26, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gorenstein, E.E.; Papp, L.A. Cognitive-behavioral therapy for anxiety in the elderly. Curr. Psychiatry Rep. 2007, 9, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.G.; Marti, C.N.; Bruce, M.L.; Hegel, M.T.; Wilson, N.L.; Kunik, M.E. Six-month postintervention depression and disability outcomes of in-home telehealth problem-solving therapy for depressed, low-income homebound older adults. Depress. Anxiety 2014, 31, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.; Wu, S.; Zuverink, A.; Tomasino, K.N.; An, R.; Himle, J.A. Internet-delivered cognitive behavioral therapies for late-life depressive symptoms: A systematic review and meta-analysis. Aging Ment. Health 2020, 24, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Kao, Y.C.; Lee, Y.C.; Tai, S.A.; Mendez, S.R.; Sasaki, K.; Tang, W.; Papatheodorou, S. Remote cognitive behavioral therapy for older adults with anxiety symptoms: A systematic review and meta-analysis. J. Telemed. Telecare, 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Siegel, C.; Dorner, T.E. Information technologies for active and assisted living-Influences to the quality of life of an ageing society. Int. J. Med. Inf. 2017, 100, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Schulte, N.; Elting, F.; Winkler, E.C.; Hetjens, S.; Berger, A.K.; Zschäbitz, S.; Hofmann, J.; Hofmann, J.; Hilbertz, L.; et al. Sequential Geriatric Assessment in Older Patients with Colorectal Cancer during Chemotherapy: Subgroup Analysis of a Prospective, Multicenter Study EpiReal 75. Oncol. Res. Treat. 2022, 45, 670–680. [Google Scholar] [CrossRef]
- Rønning, B.; Wyller, T.B.; Jordhøy, M.S.; Nesbakken, A.; Bakka, A.; Seljeflot, I.; Kristjansson, S.R. Frailty indicators and functional status in older patients after colorectal cancer surgery. J. Geriatr. Oncol. 2014, 5, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Meert, G.; Kenis, C.; Milisen, K.; Debruyne, P.R.; De Groof, I.; Focan, C.; Cornélis, F.; Verschaeve, V.; Bachmann, C.; Bron, D.; et al. Functional status in older patients with cancer and a frailty risk profile: A multicenter observational study. J. Geriatr. Oncol. 2022, 13, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Honorato, M.; Calderón, O.; Rojas, V.; Fasce, G.; Bartolotti, C.; Caglevic, C. Considerations and analysis of the implementation of oncogeriatrics in Chile and its importance: Review of current literature. Front. Aging 2023, 4, 1141792. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; Flannery, M.A.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Dale, W.; Klepin, H.D.; Williams, G.R.; Alibhai, S.M.H.; Bergerot, C.; Brintzenhofeszoc, K.; Hopkins, J.O.; Jhawer, M.P.; Katheria, V.; Loh, K.P.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Systemic Cancer Therapy: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 4293–4312. [Google Scholar] [CrossRef]
- Cosco, T.D.; Howse, K.; Brayne, C. Healthy ageing, resilience and wellbeing. Epidemiol. Psychiatr. Sci. 2017, 26, 579–583. [Google Scholar] [CrossRef]
- United States Census Bureau. 2023 National Population Projections Tables: Main Series. In Projected Population by Age Group and Sex; United States Census Bureau: Washington, DC, USA, 2023. [Google Scholar]
- National Cancer Institute. Annual Report to the Nation 2022: Overall Cancer Statistics. Available online: https://seer.cancer.gov/report_to_nation/statistics.html (accessed on 27 May 2024).

{kind=link}
{kind=link}
| Estimate | N/K | df | 95% CI | p Value | |
|---|---|---|---|---|---|
| Overall | 0.19 | 17/124 | 15 | 0.0166–0.364 | 0.0399 * |
| Subgroup analysis with treatment modality | |||||
| Individual Based | 0.27 | 10/44 | 8.45 | −0.0621–0.602 | 0.0983 |
| Small group based | 0.038 | 6/65 | 4.45 | −0.129–0.205 | 0.573 |
| Individual Based Combined with Small Group Based | Due to the small sample size (1/4), we are not able to analyze this subgroup. | ||||
| Family Based | Due to the small sample size (1/9), we are not able to analyze this subgroup. | ||||
| Subgroup analysis with the delivery format | |||||
| In-person Therapy | 0.17 | 8/61 | 6.24 | −0.0336–0.373 | 0.0876 |
| Mixed In-person and Tech | 0.103 | 4/22 | 2.63 | −0.131–0.337 | 0.239 |
| Tech-only Interpersonal | 0.0384 | 5/39 | 3.73 | −0.205–0.282 | 0.678 |
| Technology Interpersonal and Pre-programmed | Due to the small sample size (1/2), we are not able to analyze this subgroup. | ||||
| Subgroup analysis with the number of diagnoses | |||||
| Multiple | 0.238 | 5/24 | 3.64 | −0.297–0.773 | 0.275 |
| Single | 0.182 | 12/100 | 10.5 | −0.0308–0.394 | 0.0862 |
| Subgroup analysis with cancer treatment stage | |||||
| Ongoing Curative Treatment | 0.173 | 9/59 | 7.21 | 0.0117–0.335 | 0.0388 * |
| Post-treatment Survivorship | 0.679 | 3/18 | 1.99 | −1.71–3.07 | 0.344 |
| Mixed | −0.0369 | 3/39 | 1.9 | −0.721–0.648 | 0.831 |
| Not described | Due to the small sample size (2/8), we are not able to analyze this subgroup. | ||||
| Subgroup analysis with outcome | |||||
| Mental Health | 0.217 | 16/84 | 14.2 | 0.00662–0.426 | 0.044 * |
| Quality of Life | 0.686 | 8/40 | 5.81 | −0.0766–0.214 | 0.29 |
| Estimate | N/K | df | 95% CI | p Value | |
|---|---|---|---|---|---|
| Treatment modality (ref: Individual based) | 0.282 | 16/122 | 8.01 | −0.0591–0.623 | 0.093 |
| Family based | −0.177 | 16/122 | 8.01 | −0.5184–0.164 | 0.265 |
| Individual based combined with small group based | −0.157 | 16/122 | 8.01 | −0.4982–0.184 | 0.319 |
| Small group based | −0.227 | 16/122 | 9.55 | −0.6058–0.152 | 0.211 |
| Delivery format (ref: In-person) | 0.1669 | 17/124 | 6.22 | −0.0394–0.373 | 0.09556 |
| Mixed in-person and tech | −0.0145 | 17/124 | 5.11 | −0.02887–0.260 | 0.89769 |
| Tech-only interpersonal and pre-programmed | 1.7307 | 17/124 | 6.22 | 1.5244–1.937 | <0.001 *** |
| Tech-only interpersonal | −0.1290 | 17/124 | 8.97 | −0.4015–0.143 | 0.31168 |
| Number of Diagnoses (ref: Multiple) | 0.2196 | 17/214 | 3.54 | −0.292–0.731 | 0.286 |
| Single | −0.0345 | 17/214 | 6.44 | −0.518–0.449 | 0.869 |
| Cancer stage (ref: Mixed) | −0.0252 | 17/214 | 1.94 | −0.736–0.686 | 0.890 |
| Not described | 0.1048 | 17/214 | 2.31 | −0.510–0.719 | 0.577 |
| Ongoing curative treatment | 0.2235 | 17/214 | 3.37 | −0.316–0.763 | 0.294 |
| Post-treatment survivorship | 0.5693 | 17/214 | 3.73 | −0.800–1.938 | 0.305 |
| Outcome (ref: Quality of life) | 0.103 | 17/124 | 4.55 | −0.0826–0.289 | 0.206 |
| Mental Health | 0.112 | 17/124 | 6.66 | −0.1353–0.360 | 0.316 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Keefe, K.; Chen, M.; Lesser, K.J.; DuVall, A.S.; Dils, A.T. Treating Mental Health and Quality of Life in Older Cancer Patients with Cognitive Behavioral Therapy: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2024, 21, 881. https://doi.org/10.3390/ijerph21070881
O’Keefe K, Chen M, Lesser KJ, DuVall AS, Dils AT. Treating Mental Health and Quality of Life in Older Cancer Patients with Cognitive Behavioral Therapy: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2024; 21(7):881. https://doi.org/10.3390/ijerph21070881
Chicago/Turabian StyleO’Keefe, Kathryn, Meiyan Chen, Kevin J. Lesser, Adam S. DuVall, and Alexander T. Dils. 2024. "Treating Mental Health and Quality of Life in Older Cancer Patients with Cognitive Behavioral Therapy: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 21, no. 7: 881. https://doi.org/10.3390/ijerph21070881
APA StyleO’Keefe, K., Chen, M., Lesser, K. J., DuVall, A. S., & Dils, A. T. (2024). Treating Mental Health and Quality of Life in Older Cancer Patients with Cognitive Behavioral Therapy: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 21(7), 881. https://doi.org/10.3390/ijerph21070881