

Mental Health Applications of Generative AI and Large Language Modeling in the United States



Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
4.1. Limitations
4.2. Recommendations
- Increasing AI awareness among the general public will fuel the transition from traditional therapeutics to AI-assisted therapeutics in the area of mental health that practitioners can act on.
- Improve health literacy about the understanding of the mental health condition to know more about what they are experiencing in LLM, and elevating this.
- Increase dynamic interplay between humans and AI rather than replacing healthcare practitioners, leveraging the strengths of each.
- Differentiate between AI detection of physical and mental health problems that are similar, such as atrial fibrillation versus anxiety.
- Increase the use of AI gradually to address gaps created from the mental health profession shortage.
- Apply potential advancement and application of AI in mental health sectors, by using AI-based tools to empower patients.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- He, J.; Baxter, S.L.; Xu, J.; Xu, J.; Zhou, X.; Zhang, K. The practical implementation of artificial intelligence technologies in medicine. Nat. Med. 2019, 25, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-P.O.; Liu, H.; Ting, D.S.J.; Jeon, S.; Chan, R.V.P.; Kim, J.E.; Sim, D.A.; Thomas, P.B.M.; Lin, H.; Chen, Y.; et al. Digital technology, tele-medicine and artificial intelligence in ophthalmology: A global perspective. Prog. Retin. Eye Res. 2021, 82, 100900. [Google Scholar] [CrossRef] [PubMed]
- Thirunavukarasu, A.J.; Ting, D.S.J.; Elangovan, K.; Gutierrez, L.; Tan, T.F.; Ting, D.S.W. Large language models in medicine. Nat. Med. 2023, 29, 1930–1940. [Google Scholar] [CrossRef] [PubMed]
- Skalidis, I.; Cagnina, A.; Fournier, S. Use of large language models for evidence-based cardiovascular medicine. Eur. Heart J.-Digit. Health 2023, 4, 368–369. [Google Scholar] [CrossRef] [PubMed]
- Patel, U.K.; Anwar, A.; Saleem, S.; Malik, P.; Rasul, B.; Patel, K.; Yao, R.; Seshadri, A.; Yousufuddin, M.; Arumaithurai, K. Artificial intelligence as an emerging technology in the current care of neurological disorders. J. Neurol. 2021, 268, 1623–1642. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.Z.; Prakash, K.B.; Huang, W.M.; Tan, C.H. Harnessing artificial intelligence in radiology to augment population health. Front. Med. Technol. 2023, 5, 1281500. [Google Scholar] [CrossRef] [PubMed]
- Shaban-Nejad, A.; Michalowski, M.; Buckeridge, D.L. Health intelligence: How artificial intelligence transforms population and personalized health. NPJ Digit. Med. 2018, 1, 53. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Yao, B.; Dong, Y.; Yu, H.; Hendler, J.; Dey, A.K.; Wang, D. Leveraging large language models for mental health prediction via online text data. arXiv 2023, arXiv:2307.14385. [Google Scholar]
- Guo, X.; Sun, Y.; Vosoughi, S. Emotion-based modeling of mental disorders on social media. In Proceedings of the IEEE/WIC/ACM International Conference on Web Intelligence and Intelligent Agent Technology, Melbourne, VIC, Australia, 14–17 December 2021; pp. 8–16. [Google Scholar]
- Tutun, S.; Johnson, M.E.; Ahmed, A.; Albizri, A.; Irgil, S.; Yesilkaya, I.; Ucar, E.N.; Sengun, T.; Harfouche, A. An AI-based decision support system for predicting mental health disorders. Inf. Syst. Front. 2023, 25, 1261–1276. [Google Scholar] [CrossRef] [PubMed]
- Shimron, E.; Perlman, O. AI in MRI: Computational frameworks for a faster, optimized, and automated imaging workflow. Bioengineering 2023, 10, 492. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. World Mental Health Report: Transforming Mental Health for All. 16 June 2022. Available online: https://www.who.int/publications/i/item/9789240049338 (accessed on 15 March 2024).
- Basu, K.; Sinha, R.; Ong, A.; Basu, T. Artificial intelligence: How is it changing medical sciences and its future? Indian J. Dermatol. 2020, 65, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Banerjee, S.; Gonzales-Lagos, R.; Szirony, G.M. Depression increases the risk of mortality among people living with diabetes: Results from national health and nutrition examination survey, USA. Diabetes Metab. Syndr. Clin. Res. Rev. 2023, 17, 102892. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Burkholder, G.; Sana, B.; Szirony, G.M. Social Isolation as a predictor for mortality: Implications for COVID-19 prognosis. MedRxiv 2020. [Google Scholar] [CrossRef]
- Stern, S.; Linker, S.; Vadodaria, K.C.; Marchetto, M.C.; Gage, F.H. Prediction of response to drug therapy in psychiatric disorders. Open Biol. 2018, 8, 180031. [Google Scholar] [CrossRef] [PubMed]
- Canady, V.A. Depression rates soaring, especially among women, youth. Ment. Health Wkly. 2023, 33, 7–8. [Google Scholar] [CrossRef]
- Gallup Organization. U.S. Depression Rates Reach New Highs; Gallup Organization: Washington, DC, USA, 2023; Available online: https://news.gallup.com/poll/505745/depression-rates-reach-new-highs.aspx (accessed on 12 May 2024).
- Substance Use and Mental Health Service Administration (SAMHSA). Projections of National Expenditures for Treatment of Mental and Substance Use Disorders, 2010–2020; HHS Publication No. SMA-14-4883; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018. [Google Scholar]
- Regier, D.A.; Goldberg, I.D.; Taube, C.A. The de facto US mental health services system: A public health perspective. In Mental Health Care and Social Policy; Routledge: London, UK, 2022; pp. 105–126. [Google Scholar]
- Cabrera, J.; Loyola, M.S.; Magaña, I.; Rojas, R. Ethical dilemmas, mental health, artificial intelligence, and llm-based chatbots. In Proceedings of the International Work-Conference on Bioinformatics and Biomedical Engineering, Gran Canaria, Spain, 12–14 July 2023; Springer Nature: Cham, Switzerland, 2023; pp. 313–326. [Google Scholar]
- Radwan, A.; Amarneh, M.; Alawneh, H.; Ashqar, H.I.; AlSobeh, A.; Magableh, A.A.A.R. Predictive Analytics in Mental Health Leveraging LLM Embeddings and Machine Learning Models for Social Media Analysis. Int. J. Web Serv. Res. (IJWSR) 2024, 21, 1–22. [Google Scholar] [CrossRef]
- Ivanov, I.; Schwartz, J.M. Why Psychotropic Drugs Don’t Cure Mental Illness-But Should They? Front. Psychiatry 2021, 12, 579566. [Google Scholar] [CrossRef] [PubMed]
- Rane, N.L.; Tawde, A.; Choudhary, S.P.; Rane, J. Contribution and performance of ChatGPT and other Large Language Models (LLM) for scientific and research advancements: A double-edged sword. Int. Res. J. Mod. Eng. Technol. Sci. 2023, 5, 875–899. [Google Scholar]
- Hoffmann, J.A.; Attridge, M.M.; Carroll, M.S.; Simon, N.-J.E.; Beck, A.F.; Alpern, E.R. Association of youth suicides and county-level mental health professional shortage areas in the US. JAMA Pediatr. 2023, 177, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.; Shi, Y.; Du, Z.; Wu, J.; Fu, K.; Dou, Y.; Wang, Z. Supporting the Demand on Mental Health Services with AI-Based Conversational Large Language Models (LLMs). BioMedInformatics 2023, 4, 8–33. [Google Scholar] [CrossRef]
- Elyoseph, Z.; Hadar-Shoval, D.; Asraf, K.; Lvovsky, M. ChatGPT outperforms humans in emotional awareness evaluations. Front. Psychol. 2023, 14, 1199058. [Google Scholar] [CrossRef] [PubMed]
- Elyoseph, Z.; Levkovich, I.; Shinan-Altman, S. Assessing prognosis in depression: Comparing perspectives of AI models, mental health professionals and the general public. Fam. Med. Community Health 2024, 12 (Suppl. S1), e002583. [Google Scholar] [CrossRef] [PubMed]
- Daneshvar, H.; Boursalie, O.; Samavi, R.; Doyle, T.E.; Duncan, L.; Pires, P.; Sassi, R. SOK: Application of machine learning models in child and youth mental health decision-making. In Artificial Intelligence for Medicine; Academic Press: Cambridge, MA, USA, 2024; pp. 113–132. [Google Scholar]
- Lossio-Ventura, J.A.; Weger, R.; Lee, A.Y.; Guinee, E.P.; Chung, J.; Atlas, L.; Linos, E.; Pereira, F. A comparison of ChatGPT and fine-tuned open pre-trained transformers (opt) against widely used sentiment analysis tools: Sentiment analysis of COVID-19 survey data. JMIR Ment. Health. 2024, 11, e50150. [Google Scholar] [CrossRef] [PubMed]
- Levkovich, I.; Elyoseph, Z. suicide risk assessments through the eyes of ChatGPT-3.5 versus ChatGPT-4: Vignette study. JMIR Ment. Health 2023, 10, e51232. [Google Scholar] [CrossRef] [PubMed]
- Carson, N.J.; Mullin, B.; Sanchez, M.J.; Lu, F.; Yang, K.; Menezes, M.; Cook, B.L. Identification of suicidal behavior among psychiatrically hospitalized adolescents using natural language processing and machine learning of electronic health records. PLoS ONE 2019, 14, e0211116. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Yoon, H.; Lee, S.; Park, S.; Liu, Y.; Choi, J.D.; Lee, S.J. Fedtherapist: Mental health monitoring with user-generated linguistic expressions on smartphones via federated learning. arXiv 2023, arXiv:2310.16538. [Google Scholar]
- Sarkar, S.; Gaur, M.; Chen, L.K.; Garg, M.; Srivastava, B. A review of the explainability and safety of conversational agents for mental health to identify avenues for improvement. Front. Artif. Intell. 2023, 6, 1229805. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Dunn, P.; Conard, S.; Ng, R. Large language modeling and classical AI methods for the future of healthcare. J. Med. Surg. Public Health 2023, 1, 100026. [Google Scholar] [CrossRef]
- Eichstaedt, J.C.; Smith, R.J.; Merchant, R.M.; Ungar, L.H.; Crutchley, P.; Preoţiuc-Pietro, D.; Asch, D.A.; Schwartz, H.A. Facebook language predicts depression in medical records. Proc. Natl. Acad. Sci. USA 2018, 115, 11203–11208. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Y.; Koul, A.; Singla, R.; Ijaz, M.F. Artificial intelligence in disease diagnosis: A systematic literature review, synthesizing framework and future research agenda. J. Ambient. Intell. Humaniz. Comput. 2023, 14, 8459–8486. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.-S. Do People Use ChatGPT to Replace Doctor? A Google Trends Analysis. Ann. Biomed. Eng. 2023, 51, 2652–2653. [Google Scholar] [CrossRef] [PubMed]
- van Heerden, A.C.; Pozuelo, J.R.; Kohrt, B.A. Global mental health services and the impact of artificial intelligence–powered large language models. JAMA Psychiatry 2023, 80, 662–664. [Google Scholar] [CrossRef] [PubMed]
- Heston, T.F. Safety of large language models in addressing depression. Cureus 2023, 15, e50729. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Siemon, D.; Gnewuch, U.; Robra-Bissantz, S. Designing personality-adaptive conversational agents for mental health care. Inf. Syst. Front. 2022, 24, 923–943. [Google Scholar] [CrossRef] [PubMed]
- Völkel, S.T.; Meindl, S.; Hussmann, H. Manipulating and evaluating levels of personality perceptions of voice as-sistants through enactment-based dialogue design. In Proceedings of the CUI 2021-3rd Conference on Conversational User Interfaces, Bilbao, Spain, 27–29 July 2021; pp. 1–12. [Google Scholar]
- Habbal, A.; Ali, M.K.; Abuzaraida, M.A. Artificial Intelligence Trust, Risk and Security Management (AI TRiSM): Frameworks, applications, challenges and future research directions. Expert Syst. Appl. 2024, 240, 122442. [Google Scholar] [CrossRef]
- Timmons, A.C.; Duong, J.B.; Fiallo, N.S.; Lee, T.; Vo, H.P.Q.; Ahle, M.W.; Comer, J.S.; Brewer, L.C.; Frazier, S.L.; Chaspari, T. A Call to Action on Assessing and Mitigating Bias in Artificial Intelligence Applications for Mental Health. Perspect. Psychol. Sci. 2023, 18, 1062–1096. [Google Scholar] [CrossRef] [PubMed]
- Kuzlu, M.; Fair, C.; Guler, O. Role of Artificial Intelligence in the Internet of Things (IoT) cybersecurity. Discov. Internet Things 2021, 1, 7. [Google Scholar] [CrossRef]
- Guembe, B.; Azeta, A.; Misra, S.; Osamor, V.C.; Fernandez-Sanz, L.; Pospelova, V. The emerging threat of ai-driven cyber attacks: A review. Appl. Artif. Intell. 2022, 36, 2037254. [Google Scholar] [CrossRef]
- Polito, C.; Pupillo, L. Artificial Intelligence and Cybersecurity. Intereconomics 2024, 59, 10–13. [Google Scholar] [CrossRef]
- Humphreys, D.; Koay, A.; Desmond, D.; Mealy, E. AI hype as a cyber security risk: The moral responsibility of implementing generative AI in business. AI Ethics 2024, 1–14. [Google Scholar] [CrossRef]
- Pulyala, S.R. The Future of SIEM in a Machine Learning-Driven Cybersecurity Landscape. Turk. J. Comput. Math. Educ. (TURCOMAT) 2023, 14, 1309–1314. [Google Scholar] [CrossRef]
- Gadyatskaya, O.; Papuc, D. ChatGPT Knows Your Attacks: Synthesizing Attack Trees Using LLMs. In Proceedings of the International Conference on Data Science and Artificial Intelligence, Bangkok, Thailand, 27–30 November 2023; Springer Nature: Singapore, 2023; pp. 245–260. [Google Scholar]
- Sharman, R. Data Challenges and Societal Impacts—The Case in Favor of the Blueprint for an AI Bill of Rights (Keynote Remarks). In Proceedings of the International Conference on Big Data Analytics, Hyderabad, India, 19–22 December 2022; Springer Nature: Cham, Switzerland, 2022; pp. 3–15. [Google Scholar]
- Hine, E.; Floridi, L. The Blueprint for an AI Bill of Rights: In search of enaction, at risk of inaction. Minds Mach. 2023, 33, 285–292. [Google Scholar] [CrossRef]
- Zhu, Y.; Wen, H.; Wu, J.; Zhao, R. Online data poisoning attack against edge AI paradigm for IoT-enabled smart city. Math. Biosci. Eng. 2023, 20, 17726–17746. [Google Scholar] [CrossRef] [PubMed]
- Adomaitis, L.; Oak, R. Ethics of adversarial machine learning and data poisoning. Digit. Soc. 2023, 2, 8. [Google Scholar] [CrossRef]
- Sangwan, R.S.; Badr, Y.; Srinivasan, S.M. Cybersecurity for AI systems: A survey. J. Cybersecur. Priv. 2023, 3, 166–190. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Google Trends Search Term | Date | RSV Min/Max |
|---|---|---|
| AI | 1 January 23 | 28 (min) |
| 16 April 23 | 100 (max) | |
| AI and Mental Health | 22 January 23 | 19 (min) |
| 15 October 23 | 100 (max) | |
| AI and Depression | 17 December 23 | 23 (max) |
| 12 November23 | 100 (max) | |
| AI and Anxiety | 8 January 23 | 17 (min) |
| 26 November23 | 100 (max) |
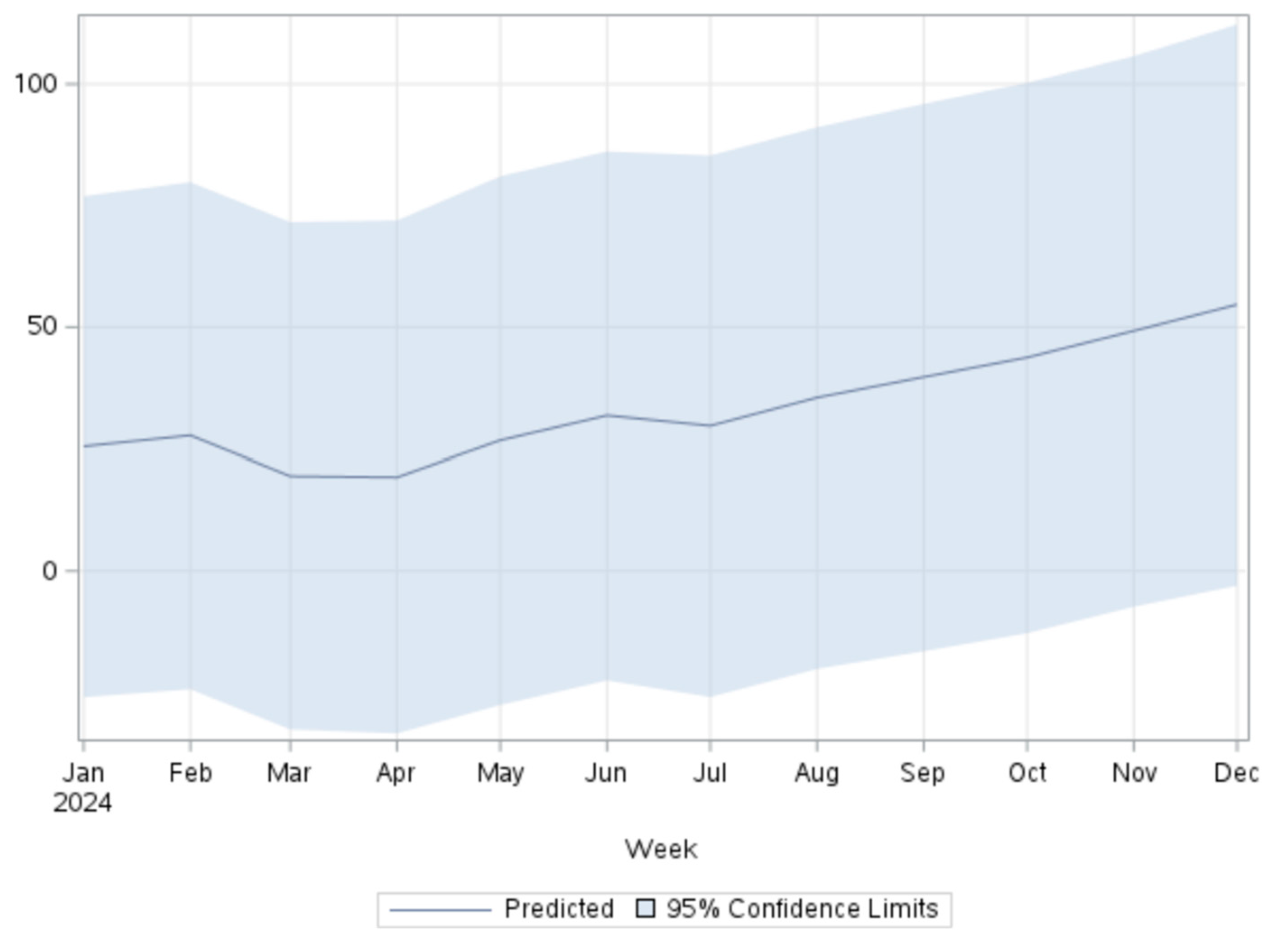
| Month | Relative Search Volume |
|---|---|
| January 2024 | 25.5 |
| February 2024 | 27.7 |
| March 2024 | 19.5 |
| April 2024 | 19.3 |
| May 2024 | 26.7 |
| June 2024 | 31.8 |
| July 2024 | 29.7 |
| August 2024 | 35.5 |
| September 2024 | 39.7 |
| October 2024 | 47.7 |
| November 2024 | 49.2 |
| December 2024 | 54.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banerjee, S.; Dunn, P.; Conard, S.; Ali, A. Mental Health Applications of Generative AI and Large Language Modeling in the United States. Int. J. Environ. Res. Public Health 2024, 21, 910. https://doi.org/10.3390/ijerph21070910
Banerjee S, Dunn P, Conard S, Ali A. Mental Health Applications of Generative AI and Large Language Modeling in the United States. International Journal of Environmental Research and Public Health. 2024; 21(7):910. https://doi.org/10.3390/ijerph21070910
Chicago/Turabian StyleBanerjee, Sri, Pat Dunn, Scott Conard, and Asif Ali. 2024. "Mental Health Applications of Generative AI and Large Language Modeling in the United States" International Journal of Environmental Research and Public Health 21, no. 7: 910. https://doi.org/10.3390/ijerph21070910
APA StyleBanerjee, S., Dunn, P., Conard, S., & Ali, A. (2024). Mental Health Applications of Generative AI and Large Language Modeling in the United States. International Journal of Environmental Research and Public Health, 21(7), 910. https://doi.org/10.3390/ijerph21070910