

Aerobic Exercise in the Aquatic Environment Suppresses the Plasma Renin Activity in Individuals with Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Methods
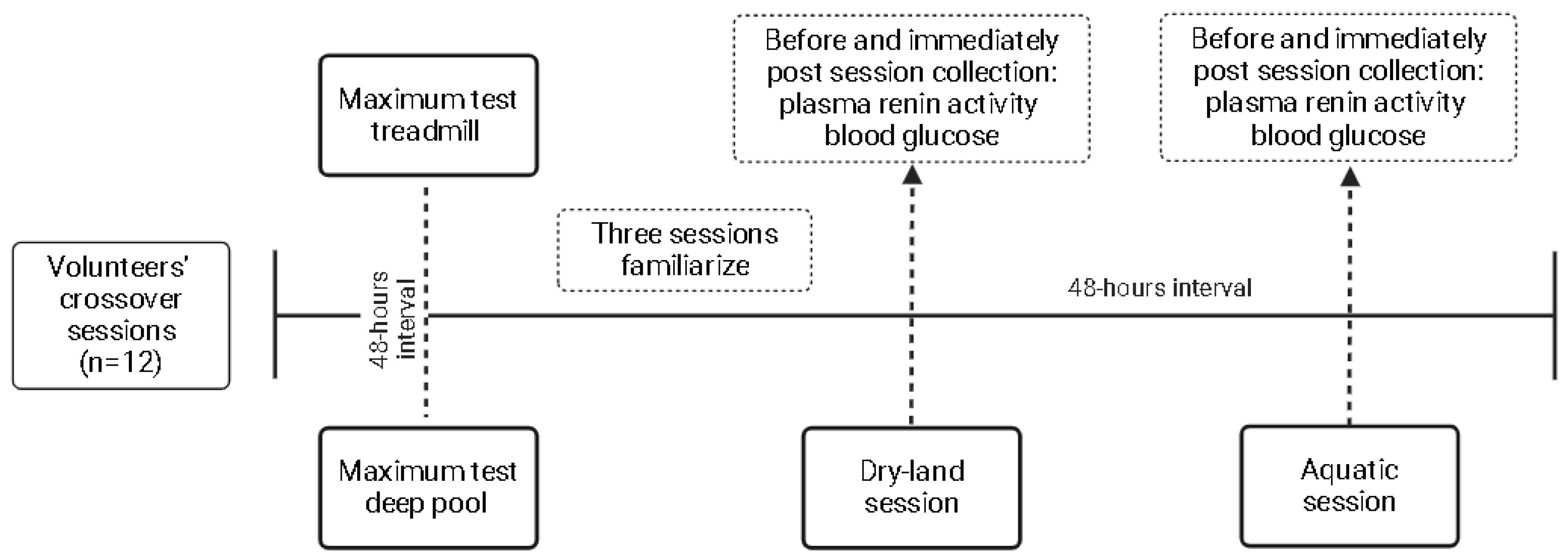
2.1. Study Design
2.2. Participants
2.3. Interventions
2.4. Assessments for Sample Characterization and Exercise Prescription
2.5. Outcomes Assessment
2.6. Statistical Analysis
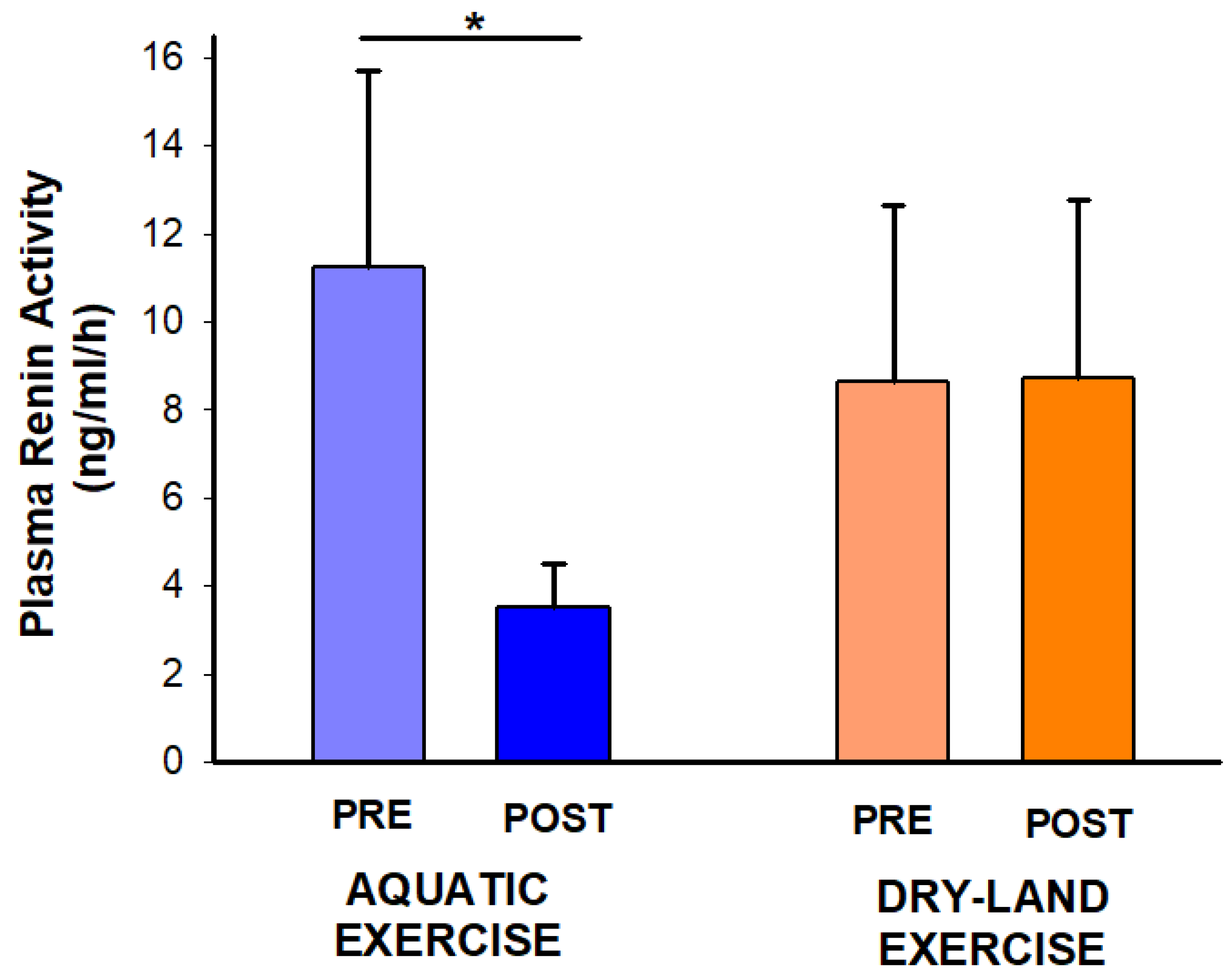
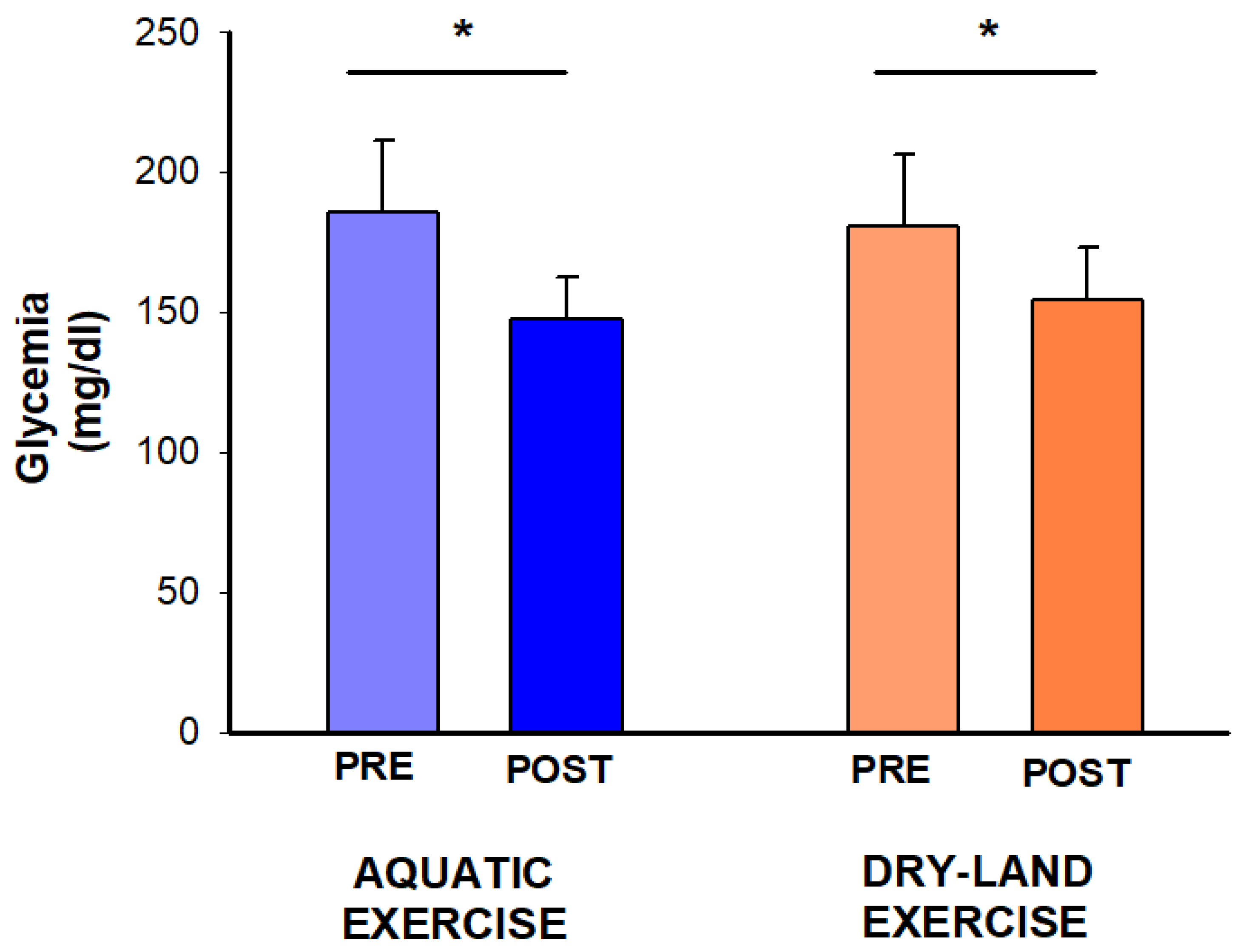
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, E.; Bonifazi, A.; Monami, M. Comparison between different types of exercise training in patients with type 2 diabetes mellitus: A systematic review and network metanalysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Pan, B.; Ge, L.; Xun, Y.-Q.; Chen, Y.-J.; Gao, C.-Y.; Han, X.; Zuo, L.-Q.; Shan, H.-Q.; Yang, K.-H.; Ding, G.-W.; et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 72. [Google Scholar] [CrossRef] [PubMed]
- Michaelidou, M.; Pappachan, J.M.; Jeeyavudeen, M.S. Management of diabesity: Current concepts. World J. Diabetes 2023, 14, 396. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2024, 44 (Suppl. S1), S1–S322. [Google Scholar]
- Delevatti, R.S.; Alberton, C.L.; Kanitz, A.C.; Marson, E.C.; Kruel, L.F.M. Vertical ground reaction force during land- and water-based exercise performed by patients with type 2 diabetes. Med. Sport. 2015, 8, 2501–2508. [Google Scholar]
- Delevatti, R.; Marson, E.; Kruel, L. Effect of aquatic exercise training on lipids profile and glycaemia: A systematic review. Rev. Andal. Med. Deport. 2015, 8, 163–170. [Google Scholar] [CrossRef]
- Pendergast, D.R.; Moon, R.E.; Krasney, J.J.; Held, H.E.; Zamparo, P. Human Physiology in an Aquatic Environment. Compr. Physiol. 2015, 5, 1705–1750. [Google Scholar] [CrossRef]
- Gabrielsen, A.; Pump, B.; Bie, P.; Christensen, N.J.; Warberg, J.; Norsk, P. Atrial distension, haemodilution, and acute control of renin release during water immersion in humans. Acta Physiol. Scand. 2002, 174, 91–99. [Google Scholar] [CrossRef]
- Ribeiro-Oliveira, A.; Nogueira, A.I.; Pereira, R.M.; Boas, W.W.V.; Dos Santos, R.A.S.; Simões e Silva, A.C. The renin-angiotensin system and diabetes: An update. Vasc. Health Risk Manag. 2008, 4, 787–803. [Google Scholar]
- Goossens, G.H. The renin-angiotensin system in the pathophysiology of type 2 diabetes. Obes. Facts 2012, 5, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Leung, P.; Carlsson, P. Tissue renin-angiotensin system: Its expression, localization, regulation and potential role in the pancreas. J. Mol. Endocrinol. 2001, 26, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, P.O.; Berne, C.; Jansson, L. Angiotensin II and the endocrine pancreas: Effects on islet blood flow and insulin secretion in rats. Diabetologia 1998, 41, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Delevatti, R.S.; Kanitz, A.C.; Alberton, C.L.; Marson, E.C.; Lisboa, S.C.; Pinho, C.D.F.; Lovatel, G.A.; Korb, A.; Bertoldi, K.; Macedo, R.C.; et al. Glucose control can be similarly improved after aquatic or dry-land aerobic training in patients with type 2 diabetes: A randomized clinical trial. J. Sci. Med. Sport 2016, 19, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Delevatti, R.S.; Pinho, C.D.F.; Kanitz, A.C.; Alberton, C.L.; Marson, E.C.; Bregagnol, L.P.; Lisboa, S.C.; Schaan, B.D.; Kruel, L.F.M. Glycemic reductions following water- and land-based exercise in patients with type 2 diabetes mellitus. Complement. Ther. Clin. Pract. 2016, 24, 73–77. [Google Scholar] [CrossRef]
- Verma, S.; Gupta, M.; Holmes, D.T.; Xu, L.; Teoh, H.; Gupta, S.; Yusuf, S.; Lonn, E.M. Plasma renin activity predicts cardiovascular mortality in the Heart Outcomes Prevention Evaluation (HOPE) study. Eur. Heart J. 2011, 32, 2135–2142. [Google Scholar] [CrossRef] [PubMed]
- Howley, E.T.; Bassett, D.R.; Welch, H.G. Criteria for maximal oxygen uptake: Review and commentary. Med. Sci. Sports Exerc. 1995, 27, 1292–1301. [Google Scholar] [CrossRef]
- Kanitz, A.C.; Reichert, T.; Liedtke, G.V.; Pinto, S.S.; Alberton, C.L.; Antunes, A.H.; Cadore, E.L.; Kruel, L.F.M. Maximal and anaerobic threshold cardiorespiratory responses during deep-water running. Rev. Bras. Cineantropomet. Desempenho Hum. 2015, 17, 41–50. [Google Scholar] [CrossRef]
- Eston, R.G.; Reilly, T. Kinanthropometry and Exercise Physiology Laboratory Manual; Routledge: London, UK, 2001; Volume 1. [Google Scholar]
- Magalhães, D.M.; Nunes-Silva, A.; Rocha, G.C.; Vaz, L.N.; de Faria, M.H.S.; Vieira, E.L.M.; Rocha, N.P.; e Silva, A.C.S. Two protocols of aerobic exercise modulate the counter-regulatory axis of the renin-angiotensin system. Heliyon 2020, 6, e03208. [Google Scholar] [CrossRef]
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/MAS Axis of the Renin-Angiotensin System: Focus on Angiotensin-(1-7). Physiol. Rev. 2018, 98, 505–553. [Google Scholar] [CrossRef]
- Burden, A.C.; Thurston, H. Plasma renin activity in diabetes mellitus. Clin. Sci. 1979, 56, 255–259. [Google Scholar] [CrossRef]
- Goessler, K.; Polito, M.; Cornelissen, V.A. Effect of exercise training on the renin-angiotensin-aldosterone system in healthy individuals: A systematic review and meta-analysis. Hypertens. Res. 2016, 39, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Coruzzi, P.; Novarini, A.; Musiari, L.; Rossi, E.; Borghetti, A. Effects of ‘Central Hypervolemia’ by Water Immersion on Renin-Aldosterone System and ACTH-Cortisol Axis in Hemodialyzed Patients. Nephron 1984, 36, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M. Cardiovascular and renal effects of head-out water immersion in man: Application of the model in the assessment of volume homeostasis. Circ. Res. 1976, 39, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Delevatti, R.S.; Netto, N.; Heberle, I.; Bracht, C.G.; Santiago, É.; Lisboa, S.D.C.; Costa, R.R.; Hübner, A.; Fossati, M.; Kruel, L.F.M. Acute and chronic glycemic effects of aerobic training in patients with type 2 diabetes. Rev. Bras. Atividade Física Saúde 2018, 23, 1–8. [Google Scholar] [CrossRef]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Middle-Aged and Older Patients with Type 2 Diabetes: A Randomized Controlled Crossover Trial of the Acute Effects of Treadmill Walking on Glycemic Control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef]
- Santiago, É.; Delevatti, R.S.; Bracht, C.G.; Netto, N.; Lisboa, S.C.; Vieira, A.F.; Costa, R.R.; Hübner, A.; Fossati, M.A.; Kruel, L.F.M. Acute glycemic and pressure responses of continuous and interval aerobic exercise in patients with type 2 diabetes. Clin. Exp. Hypertens. 2018, 40, 179–185. [Google Scholar] [CrossRef]
- Terada, T.; Friesen, A.; Chahal, B.S.; Bell, G.J.; McCargar, L.J.; Boulé, N.G. Exploring the Variability in Acute Glycemic Responses to Exercise in Type 2 Diabetes. J. Diabetes Res. 2013, 2013, e591574. [Google Scholar] [CrossRef]
- Prabhakar, S.S. Inhibition of renin-angiotensin system: Implications for diabetes control and prevention. J. Investig. Med. 2013, 61, 551–557. [Google Scholar] [CrossRef]
- Velasquez, M.T.; Bhathena, S.J.; Striffler, J.S.; Thibault, N.; Scalbert, E. Role of angiotensin-converting enzyme inhibition in glucose metabolism and renal injury in diabetes. Metabolism 1998, 47, 7–11. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Chavez, A.O.; Gastaldelli, A.; Perego, L.; Tripathy, D.; Saad, M.J.; Velloso, L.; Folli, F. The crosstalk between insulin and renin-angiotensin-aldosterone signaling systems and its effect on glucose metabolism and diabetes prevention. Curr. Vasc. Pharmacol. 2008, 6, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.N.; Tomlinson, B. Prevention of macrovascular disease in type 2 diabetic patients: Blockade of the renin-angiotensin-aldosterone system. Curr. Diabetes Rev. 2008, 4, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Delevatti, R.S.; Bracht, C.G.; Lisboa, S.D.C.; Costa, R.R.; Marson, E.C.; Netto, N.; Kruel, L.F.M. The Role of Aerobic Training Variables Progression on Glycemic Control of Patients with Type 2 Diabetes: A Systematic Review with Meta-analysis. Sports Med.—Open 2019, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Leonel, L.d.S.; de Brum, G.; Alberton, C.L.; Delevatti, R.S. Aquatic training improves HbA1c, blood pressure and functional outcomes of patients with type 2 diabetes: A systematic review with meta-analysis. Diabetes Res. Clin. Pract. 2023, 11, 110575. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | ± sd/n |
|---|---|
| Age (years) | 53.2 ± 8.9 |
| Sex (F/M) | 6/6 |
| Body Mass (kg) | 95.5 ± 14.0 |
| Height (cm) | 167.7 ± 11.0 |
| BMI (kg/m2) | 34.0 ± 4.0 |
| Duration of diabetes (years) | 6.3 ± 6.3 |
| Medical treatment | n (%) |
| Metformin | 11 (91%) |
| Sulphonylurea | 6 (50%) |
| Insulin | 5 (41%) |
| ACE inhibitors | 5 (41%) |
| ARAs | 6 (50%) |
| Alpha-2 Adrenergic Receptor Agonists | 1 (8%) |
| Dihydropyridine calcium channel blockers | 1 (8%) |
| Diuretics | 7 (58%) |
| Beta blockers | 3 (25%) |
| Statins | 8 (66%) |
| Acetylsalicylic acid | 6 (50%) |
| Proton pump inhibitors | 1 (8%) |
| Antiepileptics | 1 (8%) |
| Benzodiazepines | 2 (16%) |
| Antidepressants | 2 (16%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delevatti, R.S.; Leonel, L.d.S.; Rodrigues, J.G.d.S.; Kanitz, A.C.; Alberton, C.L.; Lovatel, G.A.; Siqueira, I.R.; Kruel, L.F.M. Aerobic Exercise in the Aquatic Environment Suppresses the Plasma Renin Activity in Individuals with Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2024, 21, 938. https://doi.org/10.3390/ijerph21070938
Delevatti RS, Leonel LdS, Rodrigues JGdS, Kanitz AC, Alberton CL, Lovatel GA, Siqueira IR, Kruel LFM. Aerobic Exercise in the Aquatic Environment Suppresses the Plasma Renin Activity in Individuals with Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2024; 21(7):938. https://doi.org/10.3390/ijerph21070938
Chicago/Turabian StyleDelevatti, Rodrigo Sudatti, Larissa dos Santos Leonel, João Gabriel da Silveira Rodrigues, Ana Carolina Kanitz, Cristine Lima Alberton, Gisele Agustini Lovatel, Ionara Rodrigues Siqueira, and Luiz Fernando Martins Kruel. 2024. "Aerobic Exercise in the Aquatic Environment Suppresses the Plasma Renin Activity in Individuals with Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial" International Journal of Environmental Research and Public Health 21, no. 7: 938. https://doi.org/10.3390/ijerph21070938
APA StyleDelevatti, R. S., Leonel, L. d. S., Rodrigues, J. G. d. S., Kanitz, A. C., Alberton, C. L., Lovatel, G. A., Siqueira, I. R., & Kruel, L. F. M. (2024). Aerobic Exercise in the Aquatic Environment Suppresses the Plasma Renin Activity in Individuals with Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 21(7), 938. https://doi.org/10.3390/ijerph21070938