
Native Hawaiian and Pacific Islanders’ Identity and Housing Status: The Impact on Historical Trauma and Perceived Stress

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analytics Plan
3. Results
3.1. The Interaction between NHPI Identity and Houselessness on the Perceived Stress of Transition-Aged Youth
3.2. Houselessness, Historical Trauma, and Perceived Stress
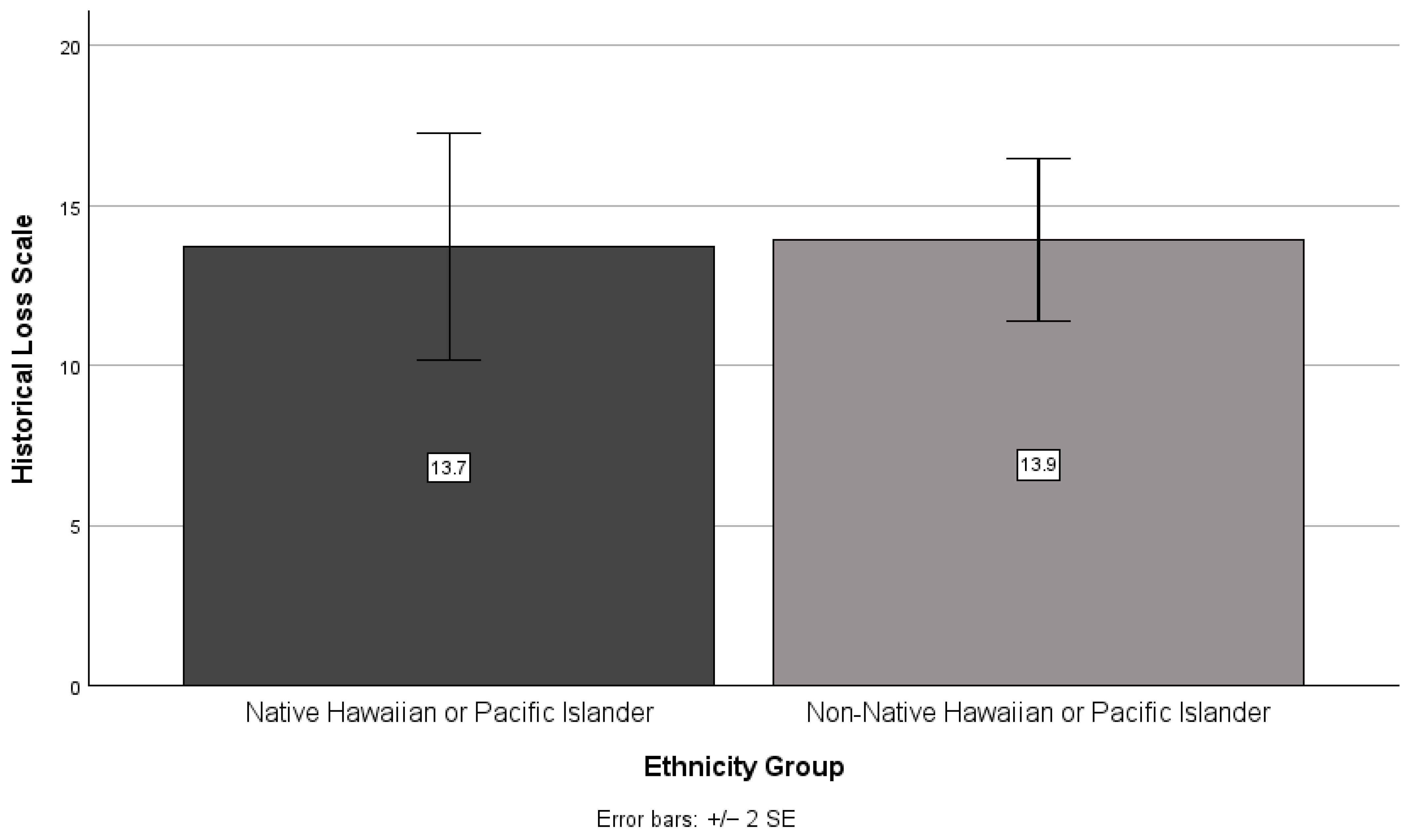
3.3. NHPI Identity, Historical Trauma, and Perceived Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- 2023 Point in Time Count. Partners in Care. Available online: https://www.partnersincareoahu.org/pitc (accessed on 5 May 2023).
- Jones, A.D. Food insecurity and mental health status: A global analysis of 149 countries. Am. J. Prev. Med. 2017, 53, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Riley, E.D.; Neilands, T.B.; Moore, K.; Cohen, J.; Bangsberg, D.R.; Havlir, D. Social, structural and behavioral determinants of overall health status in a cohort of homeless and unstably housed hiv-infected men. PLoS ONE 2012, 7, 35207. [Google Scholar] [CrossRef] [PubMed]
- Penaia, C.S.; Morey, B.N.; Thomas, K.B.; Chang, R.C.; Tran, V.D.; Pierson, N.; Greer, J.; Ponce, N.A. Disparities in Native Hawaiian and Pacific Islander covid-19 mortality: A community-driven data response. Am. J. Public Health 2021, 111, S49–S52. [Google Scholar] [CrossRef] [PubMed]
- Mental and Behavioral Health—Native Hawaiians/Pacific Islanders. Office of Minority Health; 2019. Available online: https://www.minorityhealth.hhs.gov/mental-and-behavioral-health-native-hawaiianspacific-islanders (accessed on 5 May 2023).
- Mounga, V.; Maughan, E. Breast cancer in Pacific Islander women. Nurs. Women’s Health 2012, 16, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Khago, A.; Gyawali, S. Racial/Ethnic Differences in Substance Use, Substance Use Disorders, And Substance Use Treatment Utilization Among People Aged 12 Or Older (2015–2019); Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021.
- Brave Heart, M.Y. The return to the sacred path: Healing the historical trauma and historical unresolved grief response among the Lakota through a psychoeducational group intervention. Smith Coll. Stud. Soc. Work. 1998, 68, 287–305. [Google Scholar] [CrossRef]
- Evans-Campbell, T. Historical trauma in American Indian/Native American communities: A multilevel framework for exploring impacts on individuals, families, and communities. J. Interpers. Violence 2008, 23, 316–338. [Google Scholar] [CrossRef]
- Riley, L.; Su‘esu‘e, A.; Hulama, K.; Neumann, S.K.; Chung-Do, J. Ke ala I Ka Mauliola: Native Hawaiian youth experiences with historical trauma. Int. J. Environ. Res. Public Health 2022, 19, 12564. [Google Scholar] [CrossRef]
- Pokhrel, P.; Herzog, T.A. Historical trauma and substance use among Native Hawaiian College students. Am. J. Health Behav. 2014, 38, 420–429. [Google Scholar] [CrossRef]
- Smith, K.E.; Pollak, S.D. Early life stress and development: Potential mechanisms for adverse outcomes. J. Neurodev. Disord. 2020, 12, 34. [Google Scholar] [CrossRef]
- Brietzke, E.; Sant’anna, M.K.; Jackowski, A.; Grassi-Oliveira, R.; Bucker, J.; Zugman, A.; Mansur, R.B.; Bressan, R.A. Impact of childhood stress on psychopathology. Rev. Bras. Psiquiatr. 2012, 34, 480–488. [Google Scholar] [CrossRef]
- Aparicio, E.M.; Birmingham, A.; Rodrigues, E.N.; Houser, C. Dual experiences of teenage parenting and homessless among Native Hawaiian youth: A critical interpretative phenomenological analysis. Child Fam. Soc. Work. 2019, 24, 330–339. [Google Scholar] [CrossRef]
- Julien-Chinn, F.J.; Park, M.L.N. Understanding the connection between the ‘Aina, strengths, and houselessness among previously houseless Native Hawaiian and Micronesian families. J. Hum. Behav. Soc. Environ. 2022, 32, 466–477. [Google Scholar] [CrossRef]
- McDermott, C.L.; Seidlitz, J.; Nadig, A.; Liu, S.; Clasen, L.S.; Blumenthal, J.D.; Reardon, P.K.; Lalonde, F.; Greenstein, D.; Patel, R.; et al. Longitudinally mapping childhood socioeconomic status associations with cortical and subcortical morphology. J. Neurosci. 2018, 39, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Taira, D.A.; Lim, E.; Chen, J. Modeling poverty and health for Native Hawaiian and Pacific Islander and Asian ethnic populations. Hawaii J. Health Soc. Welf. 2023, 82, 77–83. [Google Scholar]
- Liu, D.M.K.I.; Alameda, C.K. Social determinants of health for Native Hawaiian children and adolescents. Hawaii Med. J. 2011, 70, 11. [Google Scholar]
- Whitbeck, L.B.; Adams, G.W.; Hoyt, D.R.; Chen, X. Conceptualizing and measuring historical trauma among American Indian people. Am. J. Community Psychol. 2004, 33, 119–130. [Google Scholar] [CrossRef]
- Balsam, K.F.; Huang, B.; Fieland, K.C.; Simoni, J.M.; Walters, K.L. Culture, trauma, and wellness: A comparison of heterosexual and lesbian, gay, bisexual, and two-spirit Native Americans. Cult. Divers. Ethn. Minor. Psychol. 2004, 10, 287–301. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Bombay, A.; Matheson, K.; Anisman, H. The intergenerational effects of Indian residential schools: Implications for the concept of historical trauma. Transcult. Psychiatry 2014, 51, 320–338. [Google Scholar] [CrossRef]
- Spencer, S.D.; Pokhrel, P.; Helm, S.; Wilczek, K.; Galimov, A.; Sussman, S. Emerging adulthood attributes, discrimination, mental health, and substance use in a sample of Asian, Native Hawaiian/Pacific Islander, and White college students. Asian Am. J. Psychol. 2023, 14, 51–62. [Google Scholar] [CrossRef]
- Rew, L.; Kelley, M.; Preston, A. Psychological capital variables as protective factors in indigenous youth experiencing homelessness. Arch. Psychiatr. Nurs. 2024, 51, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.; Rawal, H. Interconnections among homelessness, family separation, and mental health: Implications for multi-sectoral social services. J. Soc. Serv. Res. 2018, 45, 543–557. [Google Scholar] [CrossRef]
- Stevens-Watkins, D.; Perry, B.; Pullen, E.; Jewell, J.; Oser, C.B. Examining the associations of racism, sexism, and stressful life events on psychological distress among African-American women. Cult. Divers. Ethn. Minor. Psychol. 2014, 20, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Walls, M.L.; Whitbeck, L.B. Distress among Indigenous North Americans. Soc. Ment. Health 2011, 1, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Wexler, L. Looking across three generations of Alaska Natives to explore how culture fosters indigenous resilience. Transcult. Psychiatry 2014, 51, 73–92. [Google Scholar] [CrossRef]
- Ramirez, L.C.; Hammack, P.L. Surviving colonization and the quest for healing: Narrative and resilience among California Indian tribal leaders. Transcult. Psychiatry 2014, 51, 112–133. [Google Scholar] [CrossRef]
- Jara, C.; Phan, N.T. An analysis of Hawaiian identity and life satisfaction through cultural reclamation: Implications for Hawaiian well-being. AlterNative Int. J. Indig. Peoples 2024, 20, 167–177. [Google Scholar] [CrossRef]
- Lee, H.-R.; Lee, H.E.; Cassel, K.; Hagiwara, M.I.; Somera, L.P. Protective effect of bilculturalism for health amongst minority youth: The case of Pacific Islander migrant youths in Hawaii. Br. J. Soc. Work. 2019, 49, 1003–1022. [Google Scholar] [CrossRef]
- Townsend, C.K.M.; Dillard, A.; Hosoda, K.K.; Maskarinec, G.G.; Maunakea, A.K.; Yoshimura, S.R.; Hughes, C.; Palakiko, D.-M.; Kehauoha, B.P.; Kaholokula, J.K. Community-based participatory research integrates behavioral and biological research to achieve health equity for Native Hawaiians. Int. J. Environ. Res. Public Health 2016, 13, 4. [Google Scholar] [CrossRef]
- Guillemin, M.; Gillam, L.; Barnard, E.; Stewart, P.; Walker, H.; Rosenthal, D. “We’re checking them out:” Indigenous and non-Indigenous research participants’ accounts of deciding to be involved in research. Int. J. Equity Health 2016, 15, 8. [Google Scholar] [CrossRef]
- Viswanathan, M.; Ammerman, A.; Eng, E.; Gartlehner, G.; Lohr, K.N.; Griffith, D.; Rhodes, S.; Samuel-Hodge, C.; Maty, S.; Lux, L.; et al. Community-Based Participatory Research: Assessing the Evidence. Summary, Evidence Report/Technology Assessment No. 99 (Prepared by RTI–University of North Carolina Evidence-based Practice Center under Contract No. 290-02-0016). AHRQ Publication 04-E022-1; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2004.
- McFarlane, S.J.; Occa, A.; Peng, W.; Awonuga, O.; Morgan, S.E. Community-based participatory research (CBPR) to enhance participation of racial/ethnic minorities in clinical trials: A 10-year systematic review. Health Commun. 2022, 37, 9. [Google Scholar] [CrossRef] [PubMed]
- McElfish, P.A.; Narcisse, M.-R.; Long, C.R.; Ayers, B.L.; Hawley, N.; Aitaoto, N.; Riklon, S.; Su, L.J.; Ima, S.Z.; Wilmoth, R.O.; et al. Leveraging community-based participatory research capacity to recruit Pacific Islanders into a genetics study. J. Community Genet. 2017, 8, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Antonio, M.C.K.; Keaulana, S.; Ing, C.T.; Williams, M.; Dillard, A.; Kekauoha, B.P.; Kenney, M.; Marshall, S.M.; Cassel, K.; Abrigo, S.; et al. A psychometric analysis of the adapted historical loss scale and historical loss associated symptoms scale among native Hawaiian adults. Front. Public Health 2024, 12, 1356627. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Response Options | n (%) |
|---|---|---|
| Age | Range | 18–24 |
| Mean | 21.37 | |
| Standard Deviation | 1.93 | |
| Race and Ethnicity a | American Indian or Alaskan Native | 2 (3.9%) |
| Asian | 30 (58.8%) | |
| Black or African American | 4 (7.8%) | |
| Latinx or Hispanic | 10 (19.6%) | |
| Native Hawaiian or Pacific Islander | 26 (51.0%) | |
| White or European American | 25 (49.0%) | |
| Other | 4 (7.8%) | |
| Housing Status | Emergency Shelter | 12 (23.5%) |
| Transitional Shelter | 5 (9.8%) | |
| Outdoor Public Area | 2 (3.9%) | |
| Living with family; Temporary | 8 (15.7) | |
| Permanent Housing | 24 (47.1%) | |
| Gender Identity b | Woman/female | 32 (62.7%) |
| Man/male | 15 (29.4%) | |
| Gender non-conforming | 2 (3.9%) | |
| Prefer not to answer | 1 (2.0%) | |
| Education b | Less than High School | 3 (5.9%) |
| Some High School | 4 (7.8%) | |
| High School Diploma or GED | 14 (27.5%) | |
| Some College | 9 (17.6%) | |
| Associate degree/Vocational | 7 (13.7%) | |
| 4-year College Degree | 7 (13.7%) | |
| Graduate Degree | 3 (5.9%) | |
| Income b | $0 to $15,000 | 21 (41.2%) |
| $15,001 to $20,000 | 5 (9.8%) | |
| $20,001 to $25,000 | 4 (7.8%) | |
| $25,001 to $30,000 | 1 (2.0%) | |
| $30,001 to $35,000 | 2 (3.9%) | |
| $40,001 to $45,000 | 1 (2.0%) | |
| $45,001 to $50,000 | 1 (2.0%) | |
| $55,001 to $60,000 | 1 (2.0%) | |
| $60,001 to $65,000 | 1 (2.0%) | |
| Experience of Food Insecurity b | Daily | 7 (13.7%) |
| More than once a week | 10 (19.6%) | |
| More than once a month | 9 (17.6%) | |
| Never | 20 (39.2%) | |
| Access to Mental Health Services b | Yes | 32 (62.7%) |
| No | 16 (31.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palafu, T.; Carreira Ching, D.L.; Acosta, V.M.; Okamoto, S.K.; Okamura, K.H. Native Hawaiian and Pacific Islanders’ Identity and Housing Status: The Impact on Historical Trauma and Perceived Stress. Int. J. Environ. Res. Public Health 2024, 21, 1249. https://doi.org/10.3390/ijerph21091249
Palafu T, Carreira Ching DL, Acosta VM, Okamoto SK, Okamura KH. Native Hawaiian and Pacific Islanders’ Identity and Housing Status: The Impact on Historical Trauma and Perceived Stress. International Journal of Environmental Research and Public Health. 2024; 21(9):1249. https://doi.org/10.3390/ijerph21091249
Chicago/Turabian StylePalafu, Tessa, Danielle L. Carreira Ching, Veronica M. Acosta, Scott K. Okamoto, and Kelsie H. Okamura. 2024. "Native Hawaiian and Pacific Islanders’ Identity and Housing Status: The Impact on Historical Trauma and Perceived Stress" International Journal of Environmental Research and Public Health 21, no. 9: 1249. https://doi.org/10.3390/ijerph21091249
APA StylePalafu, T., Carreira Ching, D. L., Acosta, V. M., Okamoto, S. K., & Okamura, K. H. (2024). Native Hawaiian and Pacific Islanders’ Identity and Housing Status: The Impact on Historical Trauma and Perceived Stress. International Journal of Environmental Research and Public Health, 21(9), 1249. https://doi.org/10.3390/ijerph21091249