Pathophysiological Impact of Cigarette Smoke Exposure on the Cerebrovascular System with a Focus on the Blood-brain Barrier: Expanding the Awareness of Smoking Toxicity in an Underappreciated Area

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
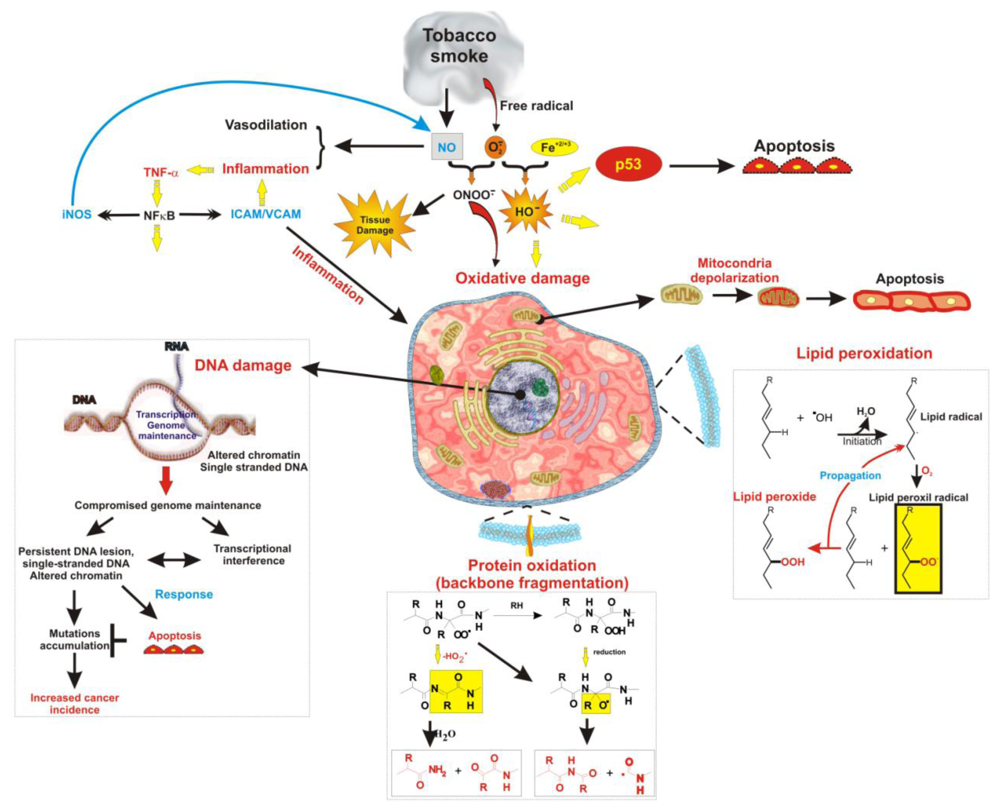
2. Tobacco Smoke Induces Oxidative Injury to the Cerebrovascular System
3. Tobacco Smoke Induces Inflammatory and Thrombotic Injury
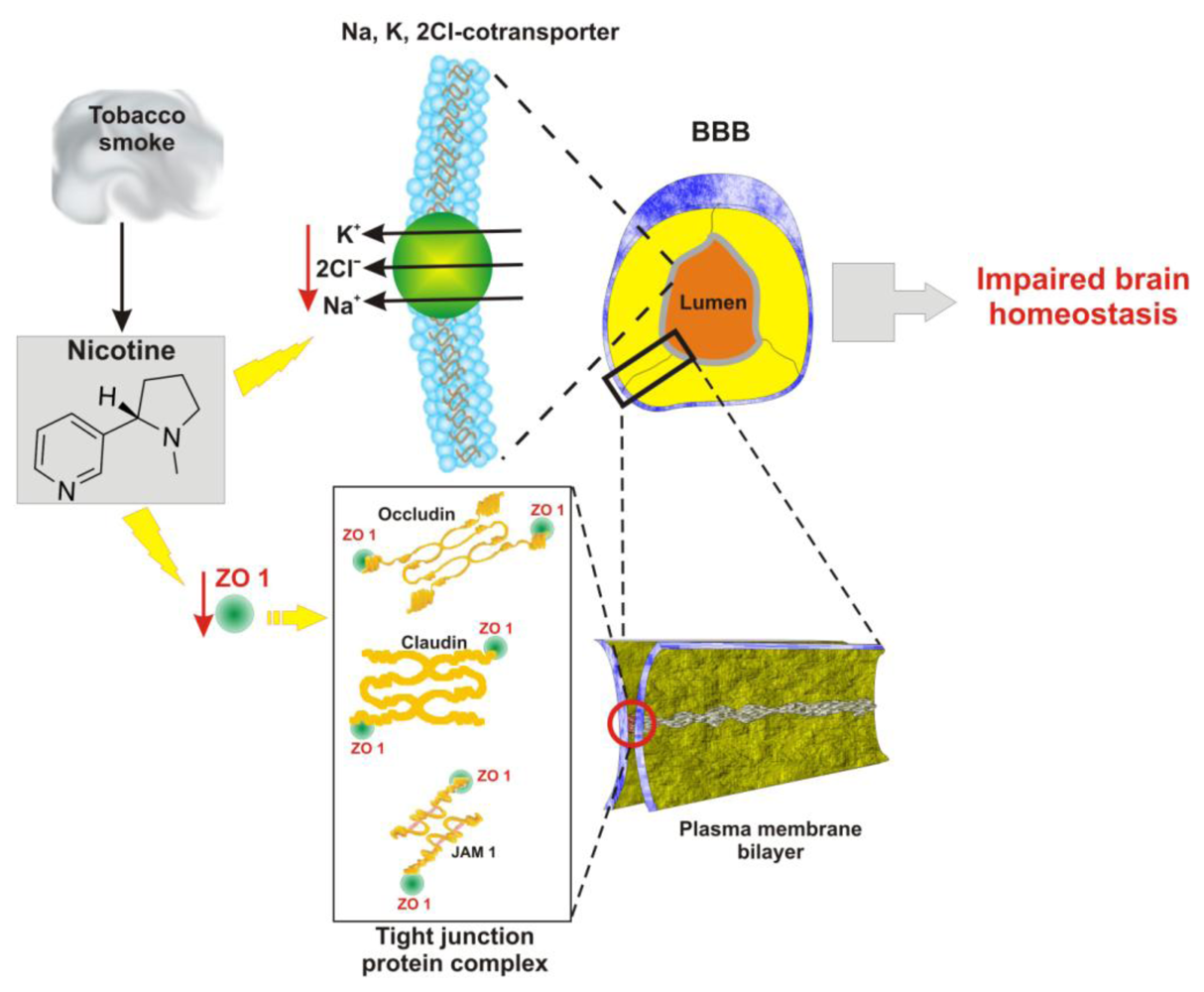
4. Pathophysiology of BBB Endothelial Cells
5. Vascular and Inflammatory Effects of Tobacco Smoke on the BBB
6. Consequences of TS Induced Damage
Small vessel ischemic disease
Cerebrovascular injuries
Behavioral impairment and increased risk for sudden infant death syndrome
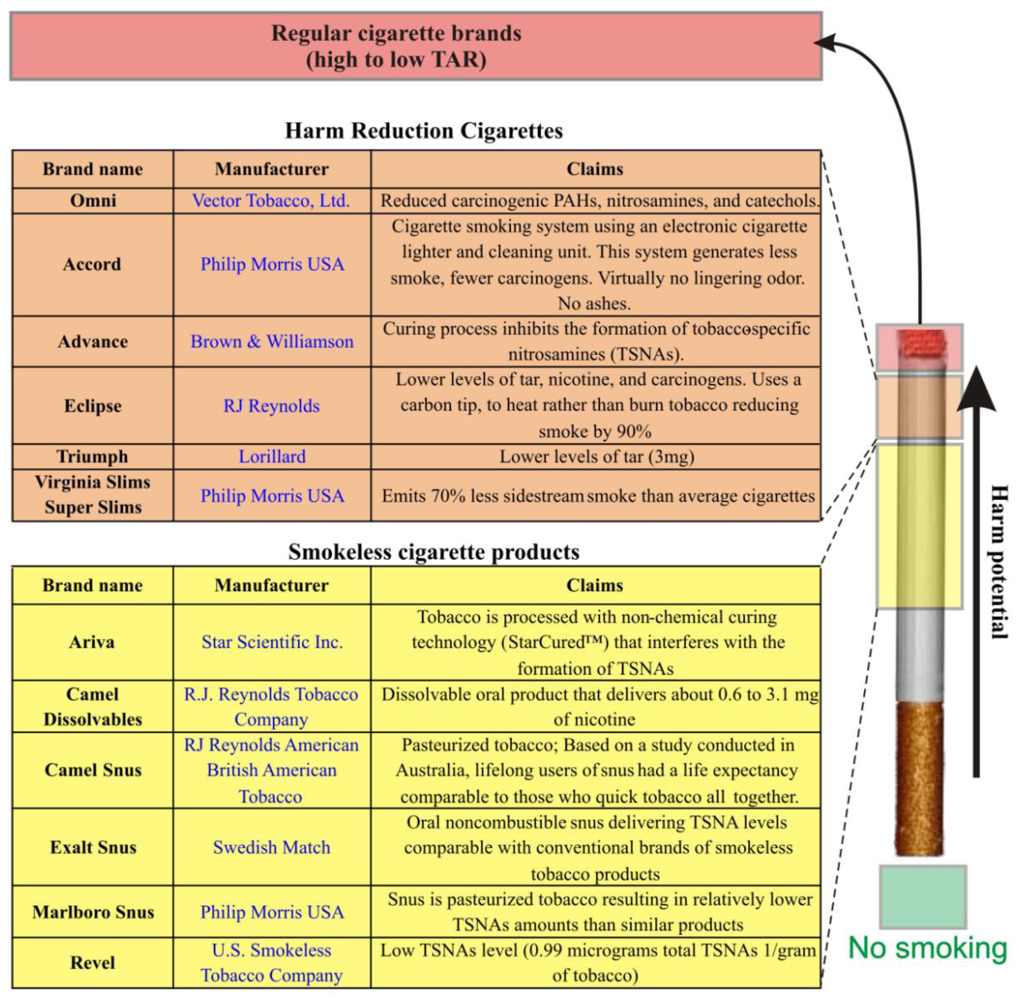
7. New Tobacco Products: Lower Risks or More of the Same?
8. Conclusions
Acknowledgements
References and Notes
- Chiu, HJ; Fischman, DA; Hammerling, U. Vitamin A depletion causes oxidative stress, mitochondrial dysfunction, and PARP-1-dependent energy deprivation. FASEB J 2008, 22, 3878–3887. [Google Scholar]
- Tsuneki, H; Sekizaki, N; Suzuki, T; Kobayashi, S; Wada, T; Okamoto, T; Kimura, I; Sasaoka, T. Coenzyme Q10 prevents high glucose-induced oxidative stress in human umbilical vein endothelial cells. Eur. J. Pharmacol 2007, 566, 1–10. [Google Scholar]
- Gallo, C; Renzi, P; Loizzo, S; Loizzo, A; Piacente, S; Festa, M; Caputo, M; Tecce, MF; Capasso, A. Potential therapeutic effects of vitamin E and C on placental oxidative stress induced by nicotine: An in vitro evidence. Open Biochem. J 2010, 4, 77–82. [Google Scholar]
- Davitashvili, DT; Museridze, DP; Svanidze, IK; Pavliashvili, NS; Sanikidze, TV. Correction of oxidative stress in the rat brain cortical cellular culture with vitamines E and C. Georgian Med. News 2010, 180, 56–60. [Google Scholar]
- Hayes, JD; Strange, RC. Potential contribution of the glutathione S-transferase supergene family to resistance to oxidative stress. Free Radical Res 1995, 22, 193–207. [Google Scholar]
- Raij, L; Demaster, EG; Jaimes, EA. Cigarette smoke-induced endothelium dysfunction: Role of superoxide anion. J. Hypertens 2001, 19, 891–897. [Google Scholar]
- Peluffo, G; Calcerrada, P; Piacenza, L; Pizzano, N; Radi, R. Superoxide-mediated inactivation of nitric oxide and peroxynitrite formation by tobacco smoke in vascular endothelium: Studies in cultured cells and smokers. Am. J. Physiol. Heart Circ. Physiol 2009, 296, H1781–H1792. [Google Scholar]
- Chow, SE; Lee, RS; Shih, SH; Chen, JK. Oxidized LDL promotes vascular endothelial cell pinocytosis via a prooxidation mechanism. FASEB J 1998, 12, 823–830. [Google Scholar]
- Colles, SM; Maxson, JM; Carlson, SG; Chisolm, GM. Oxidized LDL-induced injury and apoptosis in atherosclerosis. Potential roles for oxysterols. Trend. Cardiovasc. Med 2001, 11, 131–138. [Google Scholar]
- Banzet, N; Francois, D; Polla, BS. Tobacco smoke induces mitochondrial depolarization along with cell death: Effects of antioxidants. Redox Rep 1999, 4, 229–236. [Google Scholar]
- Tsuchiya, M; Asada, A; Kasahara, E; Sato, EF; Shindo, M; Inoue, M. Smoking a single cigarette rapidly reduces combined concentrations of nitrate and nitrite and concentrations of antioxidants in plasma. Circulation 2002, 105, 1155–1157. [Google Scholar]
- Circu, ML; Aw, TY. Reactive oxygen species, cellular redox systems, and apoptosis. Free Radic. Biol. Med 2010, 48, 749–762. [Google Scholar]
- Chen, HW; Chien, ML; Chaung, YH; Lii, CK; Wang, TS. Extracts from cigarette smoke induce DNA damage and cell adhesion molecule expression through different pathways. Chem. Biol. Interact 2004, 150, 233–241. [Google Scholar]
- Pryor, WA; Stone, K; Zang, LY; Bermudez, E. Fractionation of aqueous cigarette tar extracts: Fractions that contain the tar radical cause DNA damage. Chem. Res. Toxicol 1998, 11, 441–448. [Google Scholar]
- Stone, K; Bermudez, E; Zang, LY; Carter, KM; Queenan, KE; Pryor, WA. The ESR properties, DNA nicking, and DNA association of aged solutions of catechol versus aqueous extracts of tar from cigarette smoke. Arch. Biochem. Biophys 1995, 319, 196–203. [Google Scholar]
- DeMarini, DM. Genotoxicity of tobacco smoke and tobacco smoke condensate: A review. Mutat. Res 2004, 567, 447–474. [Google Scholar]
- Kong, Q; Lin, CL. Oxidative damage to RNA: Mechanisms, consequences, and diseases. Cell Mol. Life Sci 2010, 67, 1817–1829. [Google Scholar]
- Pfeifer, GP; Denissenko, MF; Olivier, M; Tretyakova, N; Hecht, SS; Hainaut, P. Tobacco smoke carcinogens, DNA damage and p53 mutations in smoking-associated cancers. Oncogene 2002, 21, 7435–7451. [Google Scholar]
- Rodin, SN; Rodin, AS. Origins and selection of p53 mutations in lung carcinogenesis. Semin. Cancer Biol 2005, 15, 103–112. [Google Scholar]
- Izzotti, A; Cartiglia, C; Longobardi, M; Bagnasco, M; Merello, A; You, M; Lubet, RA; De Flora, S. Gene expression in the lung of p53 mutant mice exposed to cigarette smoke. Cancer Res 2004, 64, 8566–8572. [Google Scholar]
- Koul, A; Singh, A; Sandhir, R. Effect of alpha-tocopherol on the cardiac antioxidant defense system and atherogenic lipids in cigarette smoke-inhaling mice. Inhal. Toxicol 2003, 15, 513–522. [Google Scholar]
- Kelly, G. The interaction of cigarette smoking and antioxidants. Part III: Ascorbic acid. Altern. Med. Rev 2003, 8, 43–54. [Google Scholar]
- Kelly, GS. The interaction of cigarette smoking and antioxidants. Part 2: alpha-tocopherol. Altern. Med. Rev 2002, 7, 500–511. [Google Scholar]
- Baldeiras, I; Santana, I; Proenca, MT; Garrucho, MH; Pascoal, R; Rodrigues, A; Duro, D; Oliveira, CR. Oxidative damage and progression to alzheimer’s disease in patients with mild cognitive impairment. J. Alzheim. Dis 2010, 21, 1165–1177. [Google Scholar]
- Seet, RC; Lee, CY; Lim, EC; Tan, JJ; Quek, AM; Chong, WL; Looi, WF; Huang, SH; Wang, H; Chan, YH; Halliwell, B. Oxidative damage in Parkinson disease: Measurement using accurate biomarkers. Free Radic. Biol. Med 2010, 48, 560–566. [Google Scholar]
- Reuter, S; Gupta, SC; Chaturvedi, MM; Aggarwal, BB. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med 2010, 49, 1603–1616. [Google Scholar]
- Dasgupta, J; Kar, S; Liu, R; Joseph, J; Kalyanaraman, B; Remington, SJ; Chen, C; Melendez, JA. Reactive oxygen species control senescence-associated matrix metalloproteinase-1 through c-Jun-N-terminal kinase. J. Cell. Physiol 2010, 225, 52–62. [Google Scholar]
- Kaplanski, G; Marin, V; Fabrigoule, M; Boulay, V; Benoliel, AM; Bongrand, P; Kaplanski, S; Farnarier, C. Thrombin-activated human endothelial cells support monocyte adhesion in vitro following expression of intercellular adhesion molecule-1 (ICAM-1; CD54) and vascular cell adhesion molecule-1 (VCAM-1; CD106). Blood 1998, 92, 1259–1267. [Google Scholar]
- Nordskog, BK; Blixt, AD; Morgan, WT; Fields, WR; Hellmann, GM. Matrix-degrading and pro-inflammatory changes in human vascular endothelial cells exposed to cigarette smoke condensate. Cardiovasc. Toxicol 2003, 3, 101–117. [Google Scholar]
- McMullen, CB; Fleming, E; Clarke, G; Armstrong, MA. The role of reactive oxygen intermediates in the regulation of cytokine-induced ICAM-1 surface expression on endothelial cells. Mol. Cell Biol. Res. Commun 2000, 3, 231–237. [Google Scholar]
- Masubuchi, T; Koyama, S; Sato, E; Takamizawa, A; Kubo, K; Sekiguchi, M; Nagai, S; Izumi, T. Smoke extract stimulates lung epithelial cells to release neutrophil and monocyte chemotactic activity. Amer. J. Pathol 1998, 153, 1903–1912. [Google Scholar]
- Palmblad, J. The role of granulocytes in inflammation. Scand. J. Rheumatol 1984, 13, 163–172. [Google Scholar]
- Hansen, LK; Grimm, RH, Jr; Neaton, JD. The relationship of white blood cell count to other cardiovascular risk factors. Int. J. Epidemiol 1990, 19, 881–888. [Google Scholar]
- Stampfli, MR; Anderson, GP. How cigarette smoke skews immune responses to promote infection, lung disease and cancer. Nat. Rev. Immunol 2009, 9, 377–384. [Google Scholar]
- Blackwell, CC; Tzanakaki, G; Kremastinou, J; Weir, DM; Vakalis, N; Elton, RA; Mentis, A; Fatouros, N. Factors affecting carriage of Neisseria meningitidis among Greek military recruits. Epidemiol. Infect 1992, 108, 441–448. [Google Scholar]
- Robbins, CS; Bauer, CM; Vujicic, N; Gaschler, GJ; Lichty, BD; Brown, EG; Stampfli, MR. Cigarette smoke impacts immune inflammatory responses to influenza in mice. Am. J. Respir. Crit. Care Med 2006, 174, 1342–1351. [Google Scholar]
- Chen, YH; Chen, SH; Jong, A; Zhou, ZY; Li, W; Suzuki, K; Huang, SH. Enhanced Escherichia coli invasion of human brain microvascular endothelial cells is associated with alternations in cytoskeleton induced by nicotine. Cell. Microbiol 2002, 4, 503–514. [Google Scholar]
- Iles, K; Poplawski, NK; Couper, RT. Passive exposure to tobacco smoke and bacterial meningitis in children. J. Paediatr. Child Health 2001, 37, 388–391. [Google Scholar]
- Togna, AR; Latina, V; Orlando, R; Togna, GI. Cigarette smoke inhibits adenine nucleotide hydrolysis by human platelets. Platelets 2008, 19, 537–542. [Google Scholar]
- Girdhar, G; Xu, S; Jesty, J; Bluestein, D. In vitro model of platelet-endothelial activation due to cigarette smoke under cardiovascular circulation conditions. Ann. Biomed. Eng 2008, 36, 1142–1151. [Google Scholar]
- Verma, S; Wang, CH; Li, SH; Dumont, AS; Fedak, PW; Badiwala, MV; Dhillon, B; Weisel, RD; Li, RK; Mickle, DA; Stewart, DJ. A self-fulfilling prophecy: C-reactive protein attenuates nitric oxide production and inhibits angiogenesis. Circulation 2002, 106, 913–919. [Google Scholar]
- Bernacki, J; Dobrowolska, A; Nierwinska, K; Malecki, A. Physiology and pharmacological role of the blood-brain barrier. Pharmacol. Rep 2008, 60, 600–622. [Google Scholar]
- Hagenbuch, B; Gao, B; Meier, PJ. Transport of xenobiotics across the blood-brain barrier. News Physiol. Sci 2002, 17, 231–234. [Google Scholar]
- De Boer, AB; De Lange, EL; van der Sandt, I; Breimer, DD. Transporters and the blood-brain barrier (BBB). Int. J. Clin. Pharmacol. Ther 1998, 36, 14–15. [Google Scholar]
- Weiss, N; Miller, F; Cazaubon, S; Couraud, PO. The blood-brain barrier in brain homeostasis and neurological diseases. Biochim. Biophys. Acta 2009, 1788, 842–857. [Google Scholar]
- Abbott, NJ; Revest, PA; Romero, IA. Astrocyte-endothelial interaction: Physiology and pathology. Neuropathol. Appl. Neurobiol 1992, 18, 424–433. [Google Scholar]
- Furchgott, RF. Introduction to EDRF research. J Cardiovasc Pharmacol 1993, 22(Suppl 7), S1–2. [Google Scholar]
- Furchgott, RF; Vanhoutte, PM. Endothelium-derived relaxing and contracting factors. FASEB J 1989, 3, 2007–2018. [Google Scholar]
- Bulnes, S; Argandona, EG; Bengoetxea, H; Leis, O; Ortuzar, N; Lafuente, JV. The role of eNOS in vascular permeability in ENU-induced gliomas. Acta Neurochir. Suppl 2010, 106, 277–282. [Google Scholar]
- McCarron, RM; Chen, Y; Tomori, T; Strasser, A; Mechoulam, R; Shohami, E; Spatz, M. Endothelial-mediated regulation of cerebral microcirculation. J Physiol Pharmacol 2006, 57(Suppl 11), 133–144. [Google Scholar]
- Kaur, C; Ling, EA. Blood brain barrier in hypoxic-ischemic conditions. Curr. Neurovasc. Res 2008, 5, 71–81. [Google Scholar]
- Miclescu, A; Sharma, HS; Martijn, C; Wiklund, L. Methylene blue protects the cortical blood-brain barrier against ischemia/reperfusion-induced disruptions. Crit. Care Med 2010, 38, 2109–2206. [Google Scholar]
- Greenwood, J; Howes, R; Lightman, S. The blood-retinal barrier in experimental autoimmune uveoretinitis. Leukocyte interactions and functional damage. Lab. Invest 1994, 70, 39–52. [Google Scholar]
- Holman, DW; Klein, RS; Ransohoff, RM. The blood-brain barrier, chemokines and multiple sclerosis. Biochim Biophys Acta 2010, in press. [Google Scholar]
- Cavender, DE; Edelbaum, D; Ziff, M. Endothelial cell activation induced by tumor necrosis factor and lymphotoxin. Amer. J. Pathol 1989, 134, 551–560. [Google Scholar]
- Abbruscato, TJ; Lopez, SP; Mark, KS; Hawkins, BT; Davis, TP. Nicotine and cotinine modulate cerebral microvascular permeability and protein expression of ZO-1 through nicotinic acetylcholine receptors expressed on brain endothelial cells. J. Pharm. Sci 2002, 91, 2525–2538. [Google Scholar]
- Abbruscato, TJ; Lopez, SP; Roder, K; Paulson, JR. Regulation of blood-brain barrier Na,K,2Cl-cotransporter through phosphorylation during in vitro stroke conditions and nicotine exposure. J. Pharmacol. Exp. Ther 2004, 310, 459–468. [Google Scholar]
- Hossain, M; Sathe, T; Fazio, V; Mazzone, P; Weksler, B; Janigro, D; Rapp, E; Cucullo, L. Tobacco smoke: A critical etiological factor for vascular impairment at the blood-brain barrier. Brain Res 2009, 1287, 192–205. [Google Scholar]
- Hawkins, BT; Brown, RC; Davis, TP. Smoking and ischemic stroke: a role for nicotine? Trends Pharmacol. Sci 2002, 23, 78–82. [Google Scholar]
- Hawkins, BT; Abbruscato, TJ; Egleton, RD; Brown, RC; Huber, JD; Campos, CR; Davis, TP. Nicotine increases in vivo blood-brain barrier permeability and alters cerebral microvascular tight junction protein distribution. Brain Res 2004, 1027, 48–58. [Google Scholar]
- Paulson, JR; Yang, T; Selvaraj, PK; Mdzinarishvili, A; Van der Schyf, CJ; Klein, J; Bickel, U; Abbruscato, TJ. Nicotine exacerbates brain edema during in vitro and in vivo focal ischemic conditions. J. Pharmacol. Exp. Ther 2010, 332, 371–379. [Google Scholar]
- Howard, G; Wagenknecht, LE; Burke, GL; Diez-Roux, A; Evans, GW; McGovern, P; Nieto, FJ; Tell, GS. Cigarette smoking and progression of atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA 1998, 279, 119–124. [Google Scholar]
- Pun, PB; Lu, J; Moochhala, S. Involvement of ROS in BBB dysfunction. Free Radical Res 2009, 43, 348–364. [Google Scholar]
- Yin, W; Ghebrehiwet, B; Weksler, B; Peerschke, EI. Regulated complement deposition on the surface of human endothelial cells: Effect of tobacco smoke and shear stress. Thromb. Res 2008, 122, 221–228. [Google Scholar]
- Wang, M; Zhang, W; Crisostomo, P; Markel, T; Meldrum, KK; Fu, XY; Meldrum, DR. Endothelial STAT3 plays a critical role in generalized myocardial proinflammatory and proapoptotic signaling. Am. J. Physiol. Heart Circ. Physiol 2007, 293, H2101–H2108. [Google Scholar]
- Kano, A; Wolfgang, MJ; Gao, Q; Jacoby, J; Chai, GX; Hansen, W; Iwamoto, Y; Pober, JS; Flavell, RA; Fu, XY. Endothelial cells require STAT3 for protection against endotoxin-induced inflammation. J. Exp. Med 2003, 198, 1517–1525. [Google Scholar]
- Borland, C; Higenbottam, T. Nitric oxide yields of contemporary UK, US and French cigarettes. Int. J. Epidemiol 1987, 16, 31–34. [Google Scholar]
- Wong, D; Dorovini-Zis, K; Vincent, SR. Cytokines, nitric oxide, and cGMP modulate the permeability of an in vitro model of the human blood-brain barrier. Exp. Neurol 2004, 190, 446–455. [Google Scholar]
- Yamauchi, A; Dohgu, S; Nishioku, T; Shuto, H; Naito, M; Tsuruo, T; Sawada, Y; Kataoka, Y. An inhibitory role of nitric oxide in the dynamic regulation of the blood-brain barrier function. Cell Mol. Neurobiol 2007, 27, 263–270. [Google Scholar]
- Huang, Z; Huang, PL; Ma, J; Meng, W; Ayata, C; Fishman, MC; Moskowitz, MA. Enlarged infarcts in endothelial nitric oxide synthase knockout mice are attenuated by nitro-L-arginine. J. Cereb. Blood Flow Metab 1996, 16, 981–987. [Google Scholar]
- Zhang, WZ; Venardos, K; Chin-Dusting, J; Kaye, DM. Adverse effects of cigarette smoke on NO bioavailability: Role of arginine metabolism and oxidative stress. Hypertension 2006, 48, 278–285. [Google Scholar]
- Marchi, N; Cavaglia, M; Fazio, V; Bhudia, S; Hallene, K; Janigro, D. Peripheral markers of blood-brain barrier damage. Clin. Chim. Acta 2004, 342, 1–12. [Google Scholar]
- Marchi, N; Rasmussen, P; Kapural, M; Fazio, V; Kight, K; Mayberg, MR; Kanner, A; Ayumar, B; Albensi, B; Cavaglia, M; Janigro, D. Peripheral markers of brain damage and blood-brain barrier dysfunction. Restor. Neurol. Neurosci 2003, 21, 109–121. [Google Scholar]
- Kanner, AA; Marchi, N; Fazio, V; Mayberg, MR; Koltz, MT; Siomin, V; Stevens, GH; Masaryk, T; Aumayr, B; Vogelbaum, MA; Barnett, GH; Janigro, D. Serum S100beta: A noninvasive marker of blood-brain barrier function and brain lesions. Cancer 2003, 97, 2806–2813. [Google Scholar]
- Shinton, R; Beevers, G. Meta-analysis of relation between cigarette smoking and stroke. BMJ 1989, 298, 789–794. [Google Scholar]
- Mannami, T; Iso, H; Baba, S; Sasaki, S; Okada, K; Konishi, M; Tsugane, S. Cigarette smoking and risk of stroke and its subtypes among middle-aged Japanese men and women: The JPHC Study Cohort I. Stroke 2004, 35, 1248–1253. [Google Scholar]
- Gill, JS; Shipley, MJ; Tsementzis, SA; Hornby, R; Gill, SK; Hitchcock, ER; Beevers, DG. Cigarette smoking. A risk factor for hemorrhagic and nonhemorrhagic stroke. Arch. Intern. Med 1989, 149, 2053–2057. [Google Scholar]
- He, Y; Lam, TH; Jiang, B; Wang, J; Sai, X; Fan, L; Li, X; Qin, Y; Hu, FB. Passive smoking and risk of peripheral arterial disease and ischemic stroke in Chinese women who never smoked. Circulation 2008, 118, 1535–1540. [Google Scholar]
- Miller, GJ; Bauer, KA; Cooper, JA; Rosenberg, RD. Activation of the coagulant pathway in cigarette smokers. Thromb. Haemost 1998, 79, 549–553. [Google Scholar]
- Mast, H; Thompson, JL; Lin, IF; Hofmeister, C; Hartmann, A; Marx, P; Mohr, JP; Sacco, RL. Cigarette smoking as a determinant of high-grade carotid artery stenosis in Hispanic, black, and white patients with stroke or transient ischemic attack. Stroke 1998, 29, 908–912. [Google Scholar]
- Vayssier-Taussat, M; Camilli, T; Aron, Y; Meplan, C; Hainaut, P; Polla, BS; Weksler, B. Effects of tobacco smoke and benzo[a]pyrene on human endothelial cell and monocyte stress responses. Am. J. Physiol Heart Circ. Physiol 2001, 280, H1293–H1300. [Google Scholar]
- Howard, G; Wagenknecht, LE; Cai, J; Cooper, L; Kraut, MA; Toole, JF. Cigarette smoking and other risk factors for silent cerebral infarction in the general population. Stroke 1998, 29, 913–917. [Google Scholar]
- Zhang, J; Liu, Y; Shi, J; Larson, DF; Watson, RR. Side-stream cigarette smoke induces dose-response in systemic inflammatory cytokine production and oxidative stress. Exp. Biol. Med. (Maywood) 2002, 227, 823–829. [Google Scholar]
- McQuaid, S; Cunnea, P; McMahon, J; Fitzgerald, U. The effects of blood-brain barrier disruption on glial cell function in multiple sclerosis. Biochem. Soc. Trans 2009, 37, 329–331. [Google Scholar]
- Deane, R; Zlokovic, BV. Role of the blood-brain barrier in the pathogenesis of Alzheimer’s disease. Curr. Alzheimer Res 2007, 4, 191–197. [Google Scholar]
- Slotkin, TA; Pinkerton, KE; Tate, CA; Seidler, FJ. Alterations of serotonin synaptic proteins in brain regions of neonatal Rhesus monkeys exposed to perinatal environmental tobacco smoke. Brain Res 2006, 1111, 30–35. [Google Scholar]
- Falcone, T; Fazio, V; Lee, C; Simon, B; Franco, K; Marchi, N; Janigro, D. Serum S100B: A potential biomarker for suicidality in adolescents? PLoS One 2010, 5, e11089. [Google Scholar]
- Touiki, K; Rat, P; Molimard, R; Chait, A; de Beaurepaire, R. Effects of tobacco and cigarette smoke extracts on serotonergic raphe neurons in the rat. Neuroreport 2007, 18, 925–929. [Google Scholar]
- Teaktong, T; Graham, AJ; Johnson, M; Court, JA; Perry, EK. Selective changes in nicotinic acetylcholine receptor subtypes related to tobacco smoking: An immunohistochemical study. Neuropathol. Appl. Neurobiol 2004, 30, 243–254. [Google Scholar]
- Sekizawa, S; Joad, JP; Pinkerton, KE; Bonham, AC. Secondhand tobacco smoke exposure differentially alters nucleus tractus solitarius neurons at two different ages in developing non-human primates. Toxicol. Appl. Pharmacol 2010, 242, 199–208. [Google Scholar]
- Machaalani, R; Waters, KA. Neuronal cell death in the Sudden Infant Death Syndrome brainstem and associations with risk factors. Brain 2008, 131, 218–228. [Google Scholar]
- The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Department of Health and Human Services, Office of the Surgeon General: Rockville, MD, USA, 2006.
- Blank, MD; Eissenberg, T. Evaluating oral noncombustible potential-reduced exposure products for smokers. Nicotine Tob. Res 2010, 12, 336–343. [Google Scholar]
- Stepanov, I; Carmella, SG; Briggs, A; Hertsgaard, L; Lindgren, B; Hatsukami, D; Hecht, SS. Presence of the carcinogen N’-nitrosonornicotine in the urine of some users of oral nicotine replacement therapy products. Cancer Res 2009, 69, 8236–8240. [Google Scholar]
- Boffetta, P; Hecht, S; Gray, N; Gupta, P; Straif, K. Smokeless tobacco and cancer. Lancet Oncol 2008, 9, 667–675. [Google Scholar]
- Shea, AK; Steiner, M. Cigarette smoking during pregnancy. Nicotine Tob. Res 2008, 10, 267–278. [Google Scholar]
- Almeida, OP; Garrido, GJ; Lautenschlager, NT; Hulse, GK; Jamrozik, K; Flicker, L. Smoking is associated with reduced cortical regional gray matter density in brain regions associated with incipient Alzheimer disease. Am. J. Geriatr. Psychiatr 2008, 16, 92–98. [Google Scholar]
- Sundstrom, P; Nystrom, L; Hallmans, G. Smoke exposure increases the risk for multiple sclerosis. Eur. J. Neurol 2008, 15, 579–583. [Google Scholar]



© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Mazzone, P.; Tierney, W.; Hossain, M.; Puvenna, V.; Janigro, D.; Cucullo, L. Pathophysiological Impact of Cigarette Smoke Exposure on the Cerebrovascular System with a Focus on the Blood-brain Barrier: Expanding the Awareness of Smoking Toxicity in an Underappreciated Area. Int. J. Environ. Res. Public Health 2010, 7, 4111-4126. https://doi.org/10.3390/ijerph7124111
Mazzone P, Tierney W, Hossain M, Puvenna V, Janigro D, Cucullo L. Pathophysiological Impact of Cigarette Smoke Exposure on the Cerebrovascular System with a Focus on the Blood-brain Barrier: Expanding the Awareness of Smoking Toxicity in an Underappreciated Area. International Journal of Environmental Research and Public Health. 2010; 7(12):4111-4126. https://doi.org/10.3390/ijerph7124111
Chicago/Turabian StyleMazzone, Peter, William Tierney, Mohammed Hossain, Vikram Puvenna, Damir Janigro, and Luca Cucullo. 2010. "Pathophysiological Impact of Cigarette Smoke Exposure on the Cerebrovascular System with a Focus on the Blood-brain Barrier: Expanding the Awareness of Smoking Toxicity in an Underappreciated Area" International Journal of Environmental Research and Public Health 7, no. 12: 4111-4126. https://doi.org/10.3390/ijerph7124111