Safety and Feasibility of Combining On-Demand Selective Locoregional Treatment with First-Line Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Atezolizumab Plus Bevacizumab Treatment
2.3. RFA, TACE, and Radiotherapy Administration
2.4. HCC Treatment and Decision Regarding Combination Therapy
2.5. Assessment of Therapeutic Responses, Hepatic Reserve, and Complications
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
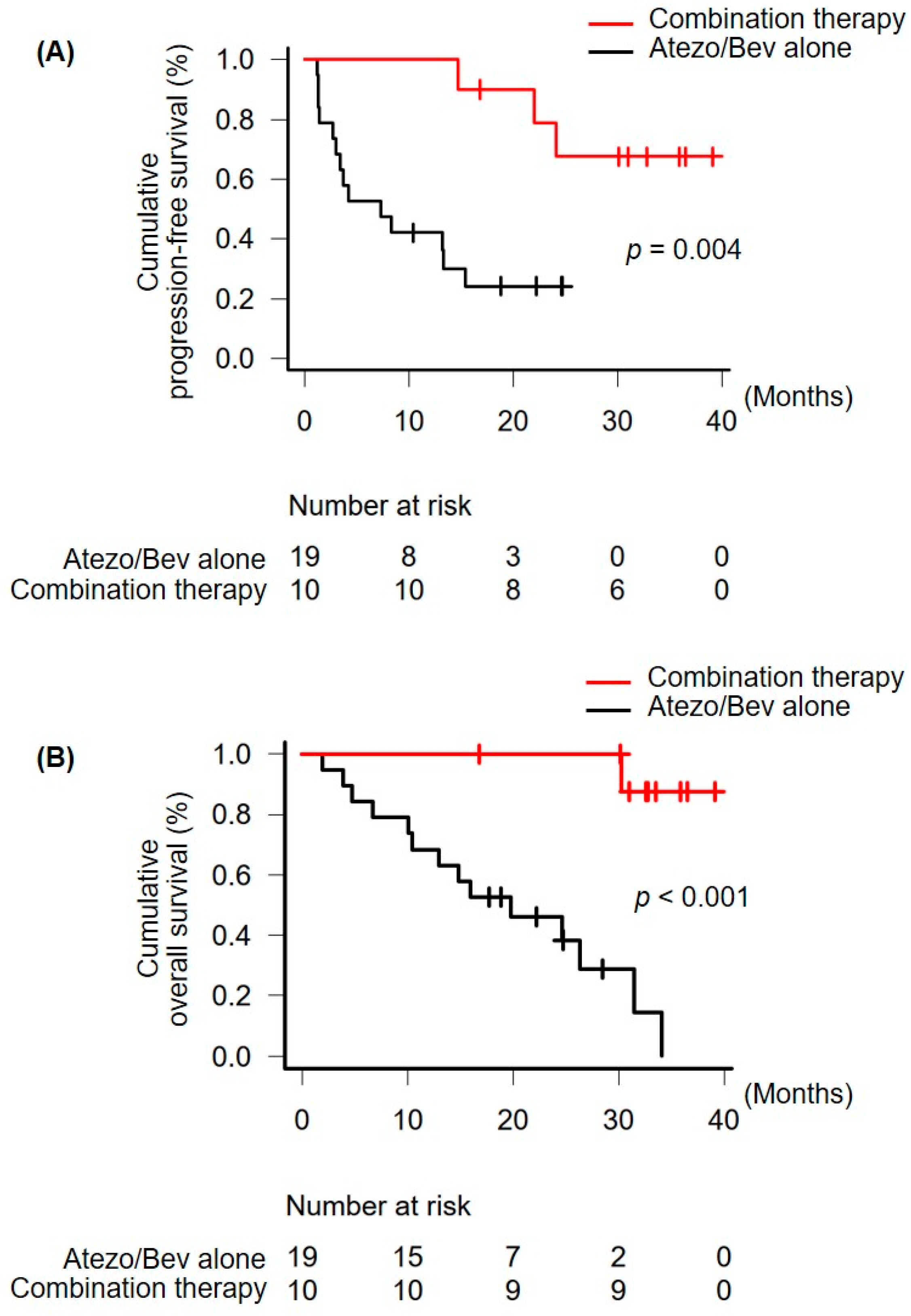
3.2. Therapeutic Responses, PFS, and OS
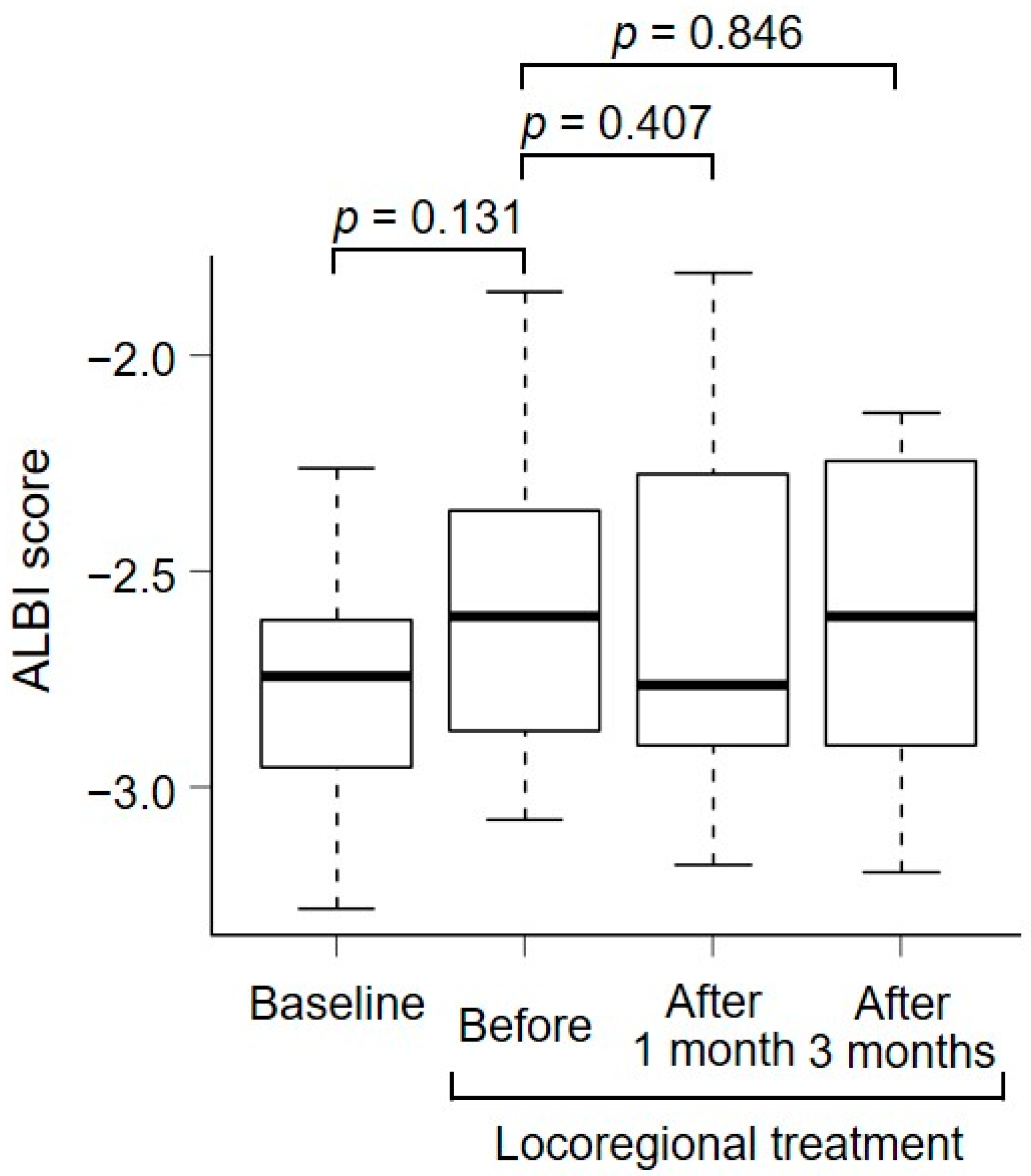
3.3. Adverse Events, Locoregional Treatment-Associated Complications, and Changes in the Hepatic Reserve after Locoregional Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Takayama, T.; Hasegawa, K.; Izumi, N.; Kudo, M.; Shimada, M.; Yamanaka, N.; Inomata, M.; Kaneko, S.; Nakayama, H.; Kawaguchi, Y.; et al. Surgery versus radiofrequency ablation for small hepatocellular carcinoma: A randomized controlled trial [SURF Trial]. Liver Cancer 2022, 11, 209–218. [Google Scholar] [CrossRef]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology 2021, 73, 158–191. [Google Scholar] [CrossRef]
- Llovet, J.M.; Castet, F.; Heikenwalder, M.; Maini, M.K.; Mazzaferro, V.; Pinato, D.J.; Pikarsky, E.; Zhu, A.X.; Finn, R.S. Immunotherapies for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2022, 19, 151–172. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Gordan, J.D.; Kennedy, E.B.; Abou-Alfa, G.K.; Beg, M.S.; Brower, S.T.; Gade, T.P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W.P.; et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO Guideline [ASCO guideline]. J. Clin. Oncol. 2020, 38, 4317–4345. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Chan, S.L.; Galle, P.R.; Rimassa, L.; Sangro, B. Systemic treatment of hepatocellular carcinoma: An EASL position paper. J. Hepatol. 2021, 75, 960–974. [Google Scholar] [CrossRef]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef]
- Iida, N.; Nakamoto, Y.; Baba, T.; Nakagawa, H.; Mizukoshi, E.; Naito, M.; Mukaida, N.; Kaneko, S. Antitumor effect after radiofrequency ablation of murine hepatoma is augmented by an active variant of CC Chemokine ligand 3/macrophage inflammatory protein-1alpha. Cancer Res. 2010, 15, 6556–6565. [Google Scholar] [CrossRef]
- Shi, L.; Chen, L.; Wu, C.; Zhu, Y.; Xu, B.; Zheng, X.; Sun, M.; Wen, W.; Dai, X.; Yang, M.; et al. PD-1 Blockade boosts radiofrequency ablation-elicited adaptive immune responses against tumor. Clin. Cancer Res. 2016, 22, 1173–1184. [Google Scholar] [CrossRef]
- Singh, P.; Toom, S.; Avula, A.; Kumar, V.; Rahma, O.E. The immune modulation effect of locoregional therapies and its potential synergy with immunotherapy in hepatocellular carcinoma. J. Hepatocell. Carcinoma 2020, 7, 11–17. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D.; Brandi, G. Trans-Arterial Chemoembolization Plus Systemic Treatments for Hepatocellular Carcinoma: An Update. J. Pers. Med. 2022, 12, 1788. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address: [email protected]; European Association for the Study of the Liver. EASL clinical practice guidelines. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Bolondi, L.; Burroughs, A.; Dufour, J.F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Ohkawa, K.; Miyazaki, M.; Sakakibara, M.; Imanaka, K.; Tamura, T.; Sueyoshi, H.; Takada, R.; Fukutake, N.; Uehara, H.; et al. Subclassification of patients with intermediate-stage (Barcelona Clinic Liver Cancer stage-B) hepatocellular carcinoma using the up-to-seven criteria and serum tumor markers. Hepatol. Int. 2017, 11, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Kishi, N.; Kanayama, N.; Hirata, T.; Ohira, S.; Wada, K.; Kawaguchi, Y.; Konishi, K.; Nagata, S.; Nakatsuka, S.I.; Marubashi, S.; et al. Preoperative stereotactic body radiotherapy to portal vein tumour thrombus in hepatocellular carcinoma: Clinical and pathological analysis. Sci. Rep. 2020, 10, 4105. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Numata, K.; Komiyama, S.; Miwa, H.; Sugimori, K.; Ogushi, K.; Moriya, S.; Nozaki, A.; Chuma, M.; Ruan, L.; et al. Combination therapy with lenvatinib and radiofrequency ablation for patients with intermediate-stage hepatocellular carcinoma beyond up-to-seven criteria and child-pugh class A liver function: A pilot study. Front. Oncol. 2022, 12, 843680. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 2020, 69, 1492–1501. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Validation of modified ALBI grade for more detailed assessment of hepatic function in hepatocellular carcinoma patients: A multicenter analysis. Liver Cancer 2019, 8, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Nakabori, T.; Abe, Y.; Higashi, S.; Hirao, T.; Kawamoto, Y.; Maeda, S.; Daiku, K.; Urabe, M.; Kai, Y.; Takada, R.; et al. Feasibility of immunotherapy in cancer patients with persistent or past hepatitis B or C virus infection. JGH Open 2022, 6, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Kawaoka, T.; Kosaka, M.; Shirane, Y.; Johira, Y.; Miura, R.; Murakami, S.; Yano, S.; Amioka, K.; Naruto, K.; et al. Early tumor response and safety of atezolizumab plus bevacizumab for patients with unresectable hepatocellular carcinoma in real-world practice. Cancers 2021, 13, 3958. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Atezolizumab plus bevacizumab treatment for unresectable hepatocellular carcinoma: Early clinical experience. Cancer Rep. 2022, 5, e1464. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Hiraoka, A.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Adverse events as potential predictive factors of therapeutic activity in patients with unresectable hepatocellular carcinoma treated with atezolizumab plus bevacizumab. Cancer Med. 2023, 12, 7772–7783. [Google Scholar] [CrossRef] [PubMed]
- Tomonari, T.; Tani, J.; Sato, Y.; Tanaka, H.; Tanaka, T.; Taniguchi, T.; Asahiro, M.; Okamoto, K.; Sogabe, M.; Miyamoto, H.; et al. Initial therapeutic results of atezolizumab plus bevacizumab for unresectable advanced hepatocellular carcinoma and the importance of hepatic functional reserve. Cancer Med. 2023, 12, 2646–2657. [Google Scholar] [CrossRef]
- Gettinger, S.; Horn, L.; Jackman, D.; Spigel, D.; Antonia, S.; Hellmann, M.; Powderly, J.; Heist, R.; Sequist, L.V.; Smith, D.C.; et al. Five-year follow-up of nivolumab in previously treated advanced non-small-cell lung cancer: Results from the CA209-003 study. J. Clin. Oncol. 2018, 36, 1675–1684. [Google Scholar] [CrossRef]
- Osa, A.; Uenami, T.; Koyama, S.; Fujimoto, K.; Okuzaki, D.; Takimoto, T.; Hirata, H.; Yano, Y.; Yokota, S.; Kinehara, Y.; et al. Clinical implications of monitoring nivolumab immunokinetics in non-small cell lung cancer patients. JCI Insight 2018, 3, e59125. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Does first-line treatment have prognostic impact for unresectable HCC?—Atezolizumab plus bevacizumab versus lenvatinib. Cancer Med. 2023, 12, 325–334. [Google Scholar] [CrossRef]
- Ueshima, K.; Nishida, N.; Hagiwara, S.; Aoki, T.; Minami, T.; Chishina, H.; Takita, M.; Minami, Y.; Ida, H.; Takenaka, M.; et al. Impact of baseline ALBI grade on the outcomes of hepatocellular carcinoma patients treated with lenvatinib: A multicenter study. Cancers 2019, 11, 952. [Google Scholar] [CrossRef]
- Lencioni, R.; Kudo, M.; Erinjeri, J.; Qin, S.; Ren, Z.; Chan, S.; Arai, Y.; Heo, J.; Mai, A.; Escobar, J.; et al. EMERALD-1: A phase 3, randomized, placebo-controlled study of transarterial chemoembolization combined with durvalumab with or without bevacizumab in participants with unresectable hepatocellular carcinoma eligible for embolization. J. Clin. Oncol. 2024, 42, LBA432. [Google Scholar] [CrossRef]
- Qin, S.; Chen, M.; Cheng, A.L.; Kaseb, A.O.; Kudo, M.; Lee, H.C.; Yopp, A.C.; Zhou, J.; Wang, L.; Wen, X.; et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): A randomised, open-label, multicentre, phase 3 trial. Lancet 2023, 402, 1835–1847. [Google Scholar] [CrossRef]
- Zhou, C.; Li, Y.; Li, J.; Song, B.; Li, H.; Liang, B.; Gu, S.; Li, H.; Chen, C.; Li, S.; et al. A phase 1/2 multicenter randomized trial of local ablation plus toripalimab versus toripalimab alone for previously treated unresectable hepatocellular carcinoma. Clin. Cancer Res. 2023, 29, 2816–2825. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Atezolizumab Plus Bevacizumab | ||||
|---|---|---|---|---|
| Variable | All Patients (n = 29) | Combination Therapy (n = 10) | Atezo/Bev Alone (n = 19) | p-Value |
| Age, years | 75 (46–85) | 73 (62–85) | 75 (46–82) | 0.927 |
| Sex, male/female | 27/2 | 9/1 | 18/1 | 1.000 |
| Etiology, HBV/HCV/NBNC | 8/5/16 | 2/4/4 | 6/1/12 | 0.080 |
| Child–Pugh score, 5/6/7 | 22/6/1 | 7/3/0 | 15/3/1 | 0.761 |
| ALBI score | −2.615 (−3.283−1.772) | −2.743 (−3.283−2.263) | −2.518 (−3.011−1.772) | 0.077 |
| Modified ALBI grade, 1/2a/2b | 16/8/5 | 8/1/1 | 8/7/4 | 0.185 |
| Platelet count, 104/μL | 18.4 (8.8–48.5) | 15.3 (12.3–36.4) | 18.7 (8.8–48.5) | 0.506 |
| Macrovascular invasion, +/− | 2/27 | 1/9 | 1/18 | 1.000 |
| Extrahepatic metastasis, +/− | 17/12 | 6/4 | 11/8 | 1.000 |
| BCLC Stage, B */C | 10/19 | 3/7 | 7/12 | 1.000 |
| NLR | 3.275 (1.364–12.88) | 4.812 (2.000–7.485) | 2.907 (1.364–12.88) | 0.085 |
| Serum AFP, ng/mL | 13 (2− > 10,000) | 8 (2–2039) | 57 (2− > 10,000) | 0.160 |
| Serum DCP, mAU/mL | 175 (<30–220,629) | 53 (<30 to 25,329) | 699 (<30–220,629) | 0.135 |
| Atezolizumab Plus Bevacizumab | |||
|---|---|---|---|
| Variable | Combination Therapy (n = 10) | Atezo/Bev Alone (n = 19) | p-Value |
| Prior to the first combination therapy | |||
| Best response, CR/PR/SD/PD | 0/4/6/0 | N.A. | |
| Objective response rate, % | 40.0 | N.A. | |
| Disease-control rate, % | 100.0 | N.A. | |
| Overall period | |||
| Best response, CR/PR/SD/PD | 5/3/2/0 | 2/2/10/5 | |
| Objective response rate, % | 80.0 | 21.1 | 0.005 |
| Disease-control rate, % | 100.0 | 73.7 | 0.134 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age, <75 vs. ≥75 years | 1.117 | 0.430–2.901 | 0.820 | |||
| Sex, male vs. female | 0.446 | 0.099–1.999 | 0.291 | |||
| Etiology, viral vs. nonviral | 0.939 | 0.360–2.446 | 0.898 | |||
| Child-Pugh score, 5 vs. 6 or 7 | 1.547 | 0.439–5.446 | 0.497 | |||
| ALBI grade, 1 vs. 2 | 2.965 | 0.752–11.69 | 0.120 | |||
| BCLC stage, B vs. C | 0.866 | 0.320–2.346 | 0.777 | |||
| NLR, <3 vs. ≥3 | 0.896 | 0.684–1.175 | 0.427 | |||
| Serum AFP, <200 vs. ≥200 ng/mL | 1.620 | 0.597–4.401 | 0.344 | |||
| Serum DCP, <1000 vs. ≥1000 mAU/mL | 2.273 | 0.870–5.937 | 0.093 | 2.320 | 0.864–6.231 | 0.095 |
| Locoregional treatment, yes vs. no | 0.183 | 0.051–0.658 | <0.001 | 0.177 | 0.048–0.652 | 0.004 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age, <75 vs. ≥75 years | 1.325 | 0.479–3.666 | 0.588 | |||
| Sex, male vs. female | 1.117 | 0.146–8.577 | 0.915 | |||
| Etiology, viral vs. nonviral | 0.763 | 0.271–2.151 | 0.609 | |||
| Child-Pugh score, 5 vs. 6 or 7 | 1.465 | 0.383–5.609 | 0.577 | |||
| ALBI grade, 1 vs. 2 | 4.989 | 1.020–24.40 | 0.047 | 5.547 | 0.877–35.09 | 0.069 |
| BCLC stage, B vs. C | 0.958 | 0.324–2.832 | 0.938 | |||
| NLR, <3 vs. ≥3 | 0.418 | 0.147–1.189 | 0.102 | |||
| Serum AFP, <200 vs. ≥200 ng/mL | 1.818 | 0.599–5.516 | 0.291 | |||
| Serum DCP, <1000 vs. ≥1000 mAU/mL | 2.880 | 1.015–8.173 | 0.047 | 4.275 | 1.231–14.84 | 0.022 |
| Locoregional treatment, yes vs. no | 0.053 | 0.006–0.417 | <0.001 | 0.027 | 0.003–0.285 | 0.003 |
| Atezolizumab Plus Bevacizumab | |||
|---|---|---|---|
| Variable | Combination Therapy (n = 10) | Atezo/Bev Alone (n = 19) | p-Value |
| Adverse events | |||
| Yes/no | 8/2 | 15/4 | 1.000 |
| Grade ≥ 3 | 4 | 7 | 1.000 |
| Liver injury | 8 | 8 | |
| Hypertension | 5 (3) | 5 (1) | |
| Proteinuria | 2 (2) | 5 (4) | |
| Adrenal cortical insufficiency | 1 | 5 | |
| Hypothyroidism | 1 | 4 | |
| Pneumonitis | 1 | 0 | |
| Tumor hemorrhage | 1 (1) | 2 (2) | |
| Subconjunctival hemorrhage | 0 | 2 | |
| Nosebleed | 0 | 1 | |
| Fever | 4 | 1 | |
| Skin rash | 2 | 2 | |
| Diarrhea | 1 | 1 | |
| Renal dysfunction | 0 | 1 (1) | |
| Hyperamylasemia | 0 | 1 (1) | |
| Fatigue | 1 | 1 | |
| Loss of appetite | 0 | 1 | |
| Stomatitis | 1 | 0 | |
| Thrombocytopenia | 1 | 0 | |
| Neutropenia | 1 | 0 | |
| Pneumothrax | 1 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakabori, T.; Higashi, S.; Abe, Y.; Mukai, K.; Ikawa, T.; Konishi, K.; Maeda, N.; Nakanishi, K.; Hasegawa, S.; Wada, H.; et al. Safety and Feasibility of Combining On-Demand Selective Locoregional Treatment with First-Line Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma. Curr. Oncol. 2024, 31, 1543-1555. https://doi.org/10.3390/curroncol31030117
Nakabori T, Higashi S, Abe Y, Mukai K, Ikawa T, Konishi K, Maeda N, Nakanishi K, Hasegawa S, Wada H, et al. Safety and Feasibility of Combining On-Demand Selective Locoregional Treatment with First-Line Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma. Current Oncology. 2024; 31(3):1543-1555. https://doi.org/10.3390/curroncol31030117
Chicago/Turabian StyleNakabori, Tasuku, Sena Higashi, Yutaro Abe, Kaori Mukai, Toshiki Ikawa, Koji Konishi, Noboru Maeda, Katsuyuki Nakanishi, Shinichiro Hasegawa, Hiroshi Wada, and et al. 2024. "Safety and Feasibility of Combining On-Demand Selective Locoregional Treatment with First-Line Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma" Current Oncology 31, no. 3: 1543-1555. https://doi.org/10.3390/curroncol31030117
APA StyleNakabori, T., Higashi, S., Abe, Y., Mukai, K., Ikawa, T., Konishi, K., Maeda, N., Nakanishi, K., Hasegawa, S., Wada, H., & Ohkawa, K. (2024). Safety and Feasibility of Combining On-Demand Selective Locoregional Treatment with First-Line Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma. Current Oncology, 31(3), 1543-1555. https://doi.org/10.3390/curroncol31030117