

Early and Long-Term Results of Simultaneous and Staged Revascularization of Coronary and Carotid Arteries

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. 30-Day Outcomes of Simultaneous and Staged CABG and CEA
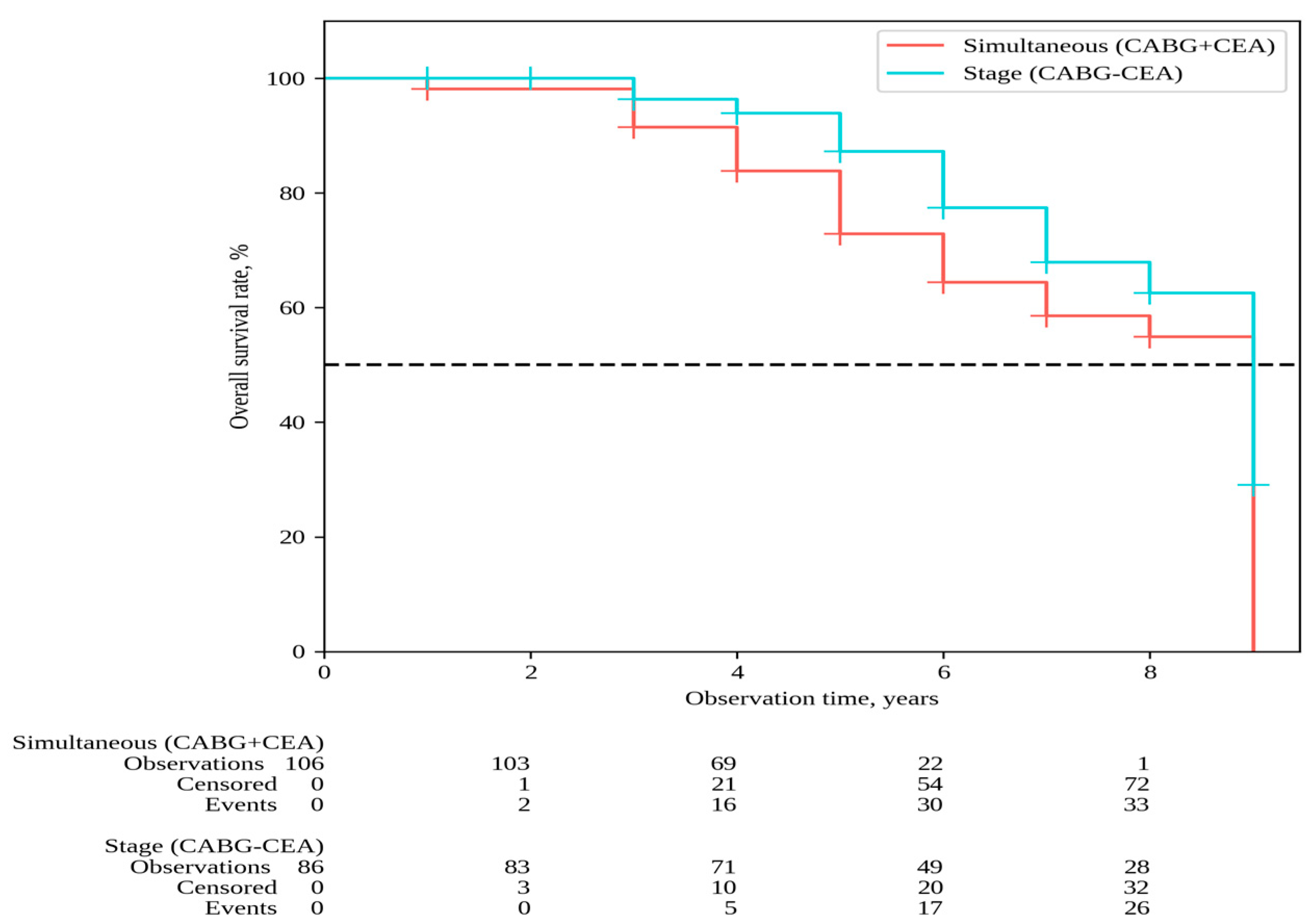
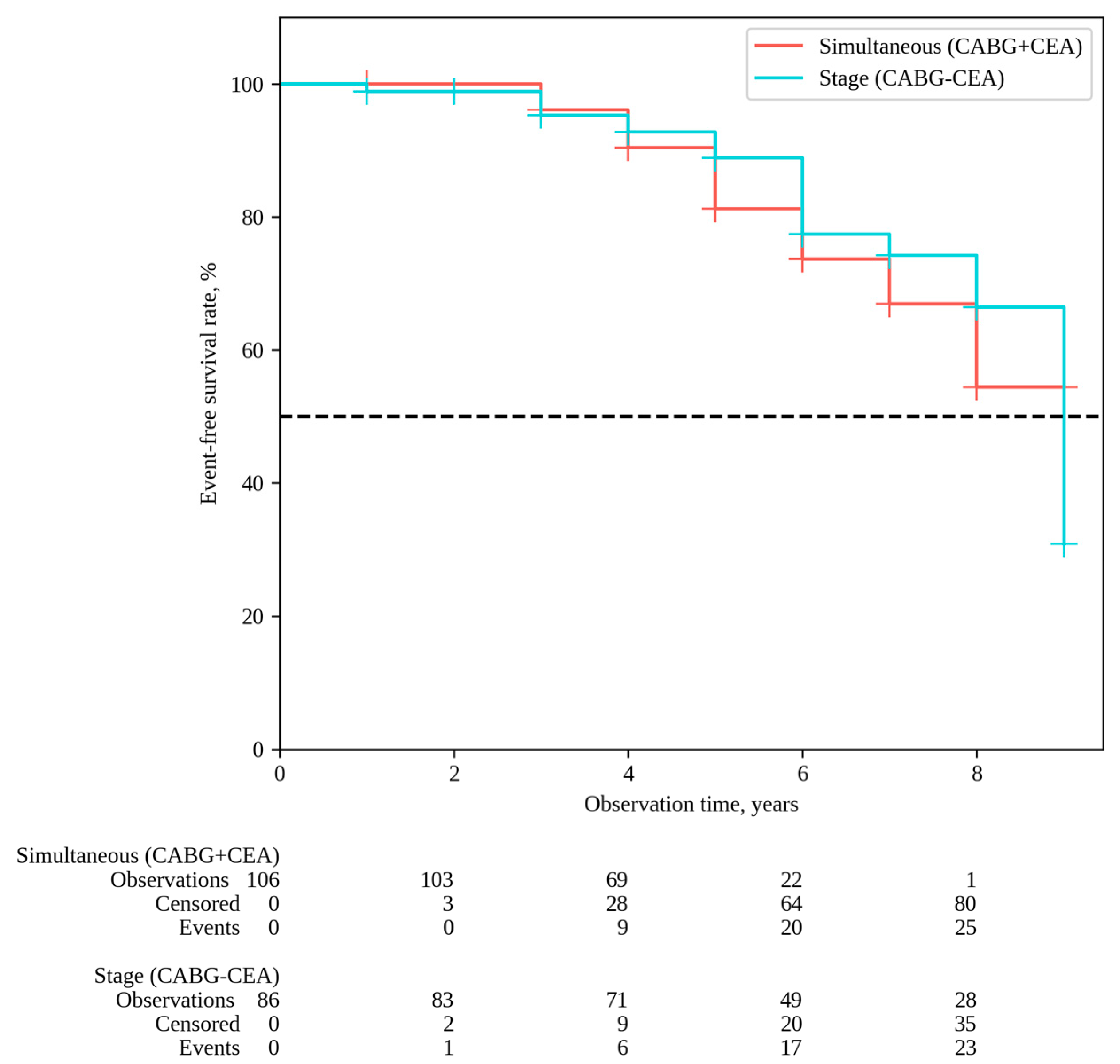
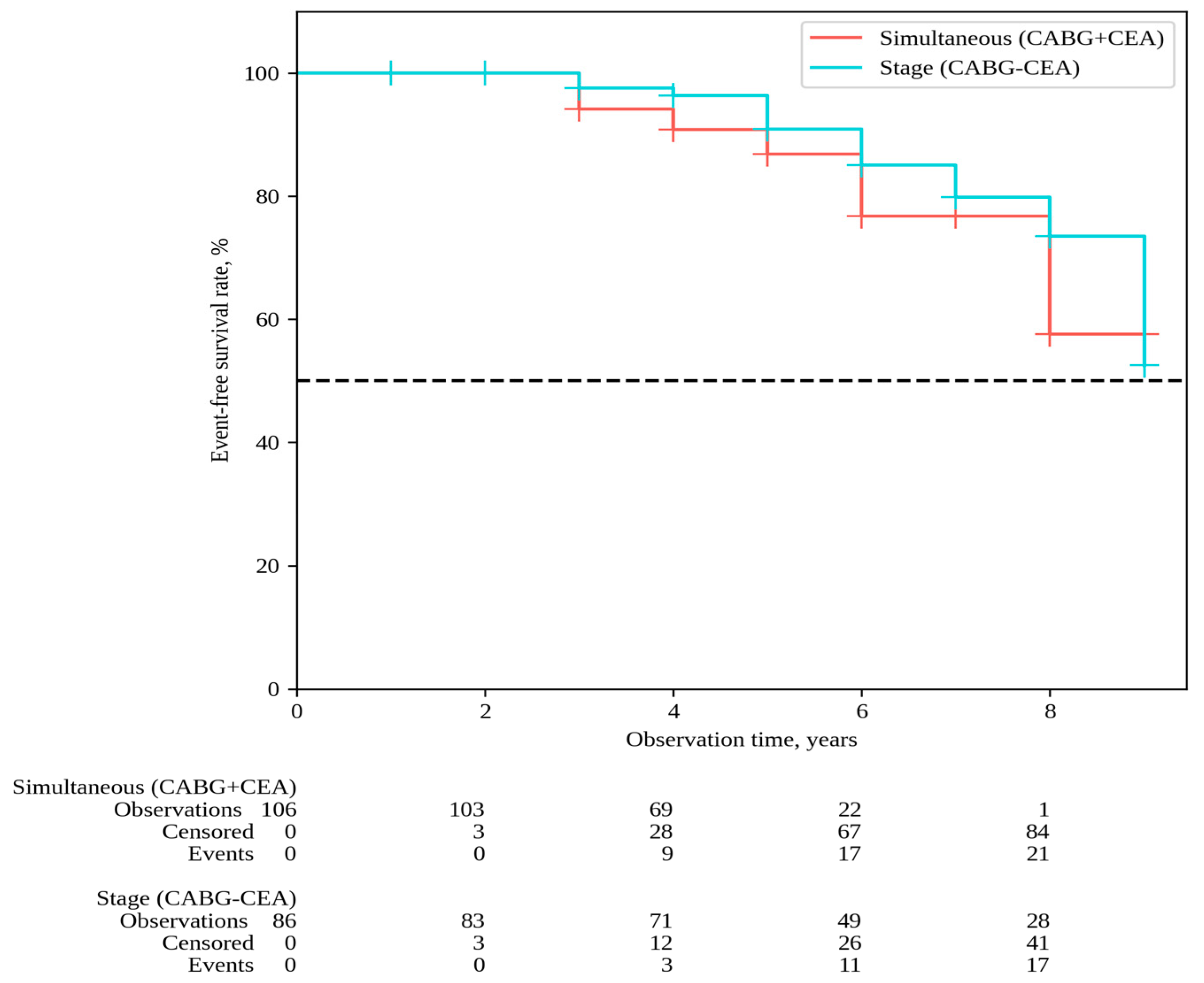
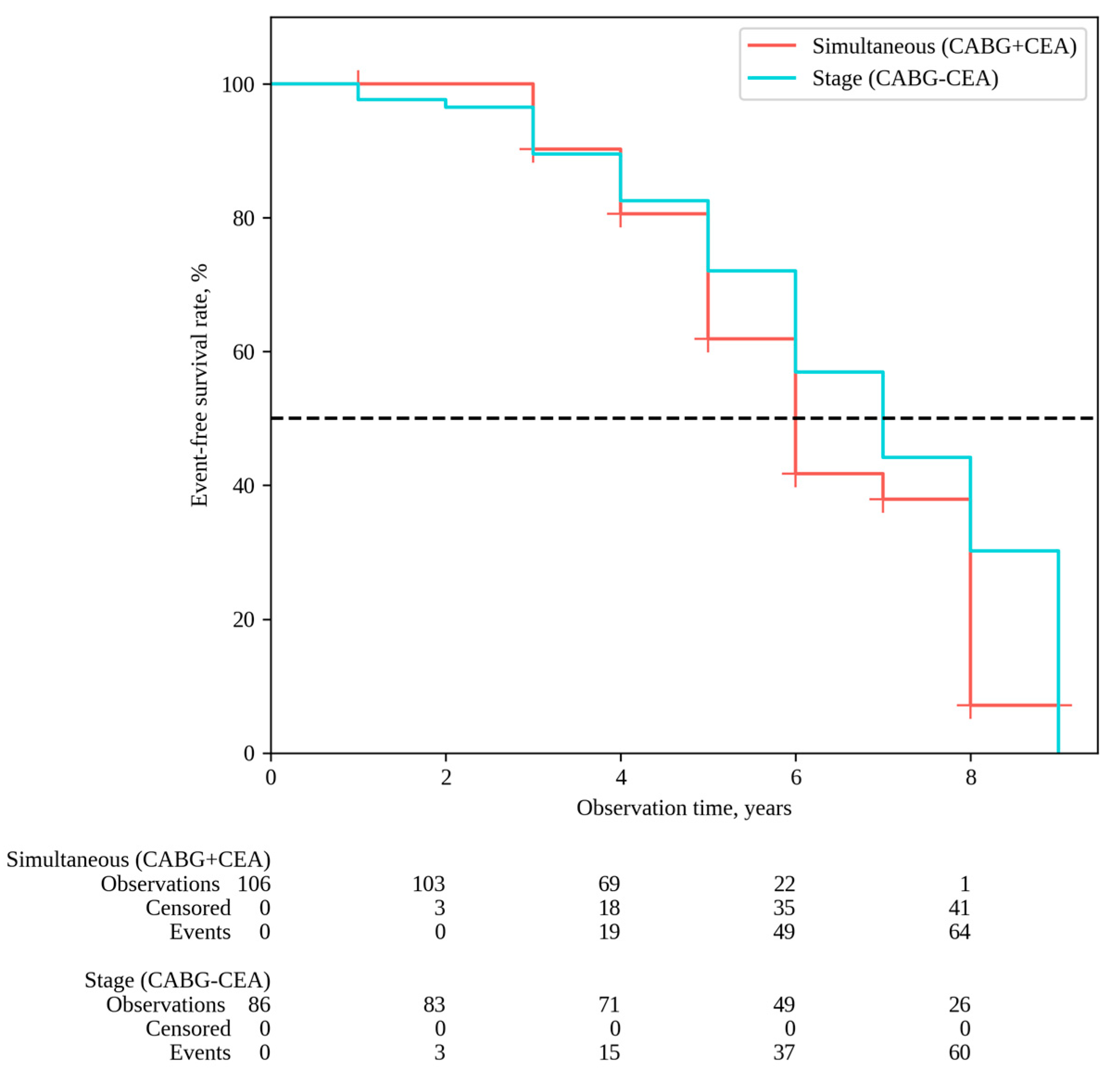
4.2. Long-Term Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Naylor, A.R.; Mehta, Z.; Rothwell, P.M.; Bell, P.R. Carotid artery disease and stroke during coronary artery bypass: A critical review of the literature. Eur. J. Vasc. Endovasc. Surg. 2002, 23, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Haywood, N.S.; Ratcliffe, S.J.; Zheng, X.; Mao, J.; Farivar, B.S.; Tracci, M.C.; Malas, M.B.; Goodney, P.P.; Clouse, W.D. Operative and long-term outcomes of combined and staged carotid endarterectomy and coronary bypass. J. Vasc. Surg. 2023, 77, 1424–1433.e1. [Google Scholar] [CrossRef] [PubMed]
- Gopaldas, R.R.; Chu, D.; Dao, T.K.; Huh, J.; LeMaire, S.A.; Lin, P.; Coselli, J.S.; Bakaeen, F.G. Staged versus synchronous carotid endarterectomy and coronary artery bypass grafting: Analysis of 10-year nationwide outcomes. Ann. Thorac. Surg. 2011, 91, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Tzoumas, A.; Giannopoulos, S.; Texakalidis, P.; Charisis, N.; Machinis, T.; Koullias, G.J. Synchronous versus Staged Carotid Endarterectomy and Coronary Artery Bypass Graft for Patients with Concomitant Severe Coronary and Carotid Artery Stenosis: A Systematic Review and Meta-analysis. Ann. Vasc. Surg. 2020, 63, 427–438.e1. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.K.; Shafi, A.M.A.; Grafton-Clarke, C.; Singh, S.; Harky, A. Concomitant severe carotid and coronary artery diseases: A separate management or concomitant approach. J. Card. Surg. 2019, 34, 803–813. [Google Scholar] [CrossRef]
- Naylor, R.; Rantner, B.; Ancetti, S.; de Borst, G.J.; De Carlo, M.; Halliday, A.; Kakkos, S.K.; Markus, H.S.; McCabe, D.J.; Sillesen, H.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 7–111. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Nedkoff, L.; Briffa, T.; Zemedikun, D.; Herrington, S.; Wright, F.L. Global Trends in Atherosclerotic Cardiovascular Disease. Clin. Ther. 2023, 45, 1087–1091. [Google Scholar] [CrossRef]
- Zivkovic, I.; Vukovic, P.; Milacic, P.; Milicic, M.; Sagic, D.; Ilijevski, N.; Krasic, S.; Peric, M.; Micovic, S. Midterm Results After Simultaneous Carotid Artery Stenting and Cardiac Surgery. Ann. Thorac. Surg. 2020, 110, 1557–1563. [Google Scholar] [CrossRef]
- Doenst, T.; Sigusch, H. Surgical collateralization: The hidden mechanism for improving prognosis in chronic coronary syndromes. J. Thorac. Cardiovasc. Surg. 2022, 163, 703–708.e2. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.F.; Mathew, J.P.; Grocott, H.P.; Mackensen, G.B.; Monk, T.; A Welsh-Bohmer, K.; A Blumenthal, J.; Laskowitz, D.T.; Mark, D.B. Central nervous system injury associated with cardiac surgery. Lancet 2006, 368, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Hood, R.; Budd, A.; Sorond, F.A.; Hogue, C.W. Peri-operative neurological complications. Anaesthesia 2018, 73 (Suppl. S1), 67–75. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; De Simone, G.; Ford, E.S.; et al. Heart disease and stroke statistics—2011 update: A report from the American Heart Association. Circulation 2011, 123, e18–e209, Erratum in Circulation 2011, 124, e426. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Ergul, E.A.; Mohebali, J.; Goodney, P.P.; Patel, V.I.; Conrad, M.F.; Eagleton, M.J.; Clouse, W.D. The effect of combining coronary bypass with carotid endarterectomy in patients with unrevascularized severe coronary disease. J. Vasc. Surg. 2019, 70, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Illuminati, G.; Ricco, J.-B.; Caliò, F.; Pacilè, M.A.; Miraldi, F.; Frati, G.; Macrina, F.; Toscano, M. Short-term results of a randomized trial examining timing of carotid endarterectomy in patients with severe asymptomatic unilateral carotid stenosis undergoing coronary artery bypass grafting. J. Vasc. Surg. 2011, 54, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Fareed, K.R.; Rothwell, P.M.; Mehta, Z.; Naylor, A.R. Synchronous carotid endarterectomy and off-pump coronary bypass: An updated, systematic review of early outcomes. Eur. J. Vasc. Endovasc. Surg. 2009, 37, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Deo, S.V.; Park, S.J.; Joyce, L.D. Meta-analysis of staged versus combined carotid endarterectomy and coronary artery bypass grafting. Ann. Thorac. Surg. 2014, 97, 102–109. [Google Scholar] [CrossRef]
- Peng, C.; Yang, Y.F.; Zhao, Y.; Yang, X.Y. Staged Versus Synchronous Carotid Endarterectomy and Coronary Artery Bypass Grafting: A Meta-Analysis and Systematic Review. Ann. Vasc. Surg. 2022, 86, 428–439. [Google Scholar] [CrossRef]
- Naylor, A.R.; Cuffe, R.L.; Rothwell, P.M.; Bell, P.R. A systematic review of outcomes following staged and synchronous carotid endarterectomy and coronary artery bypass. Eur. J. Vasc. Endovasc. Surg. 2003, 25, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Blecha, M.; De Jong, M.; Carlson, K. Risk factors for mortality within 5 years of carotid endarterectomy for asymptomatic stenosis. J. Vasc. Surg. 2022, 75, 1945–1957. [Google Scholar] [CrossRef] [PubMed]
- Halliday, A.; Bulbulia, R.; Bonati, L.H.; Chester, J.; Cradduck-Bamford, A.; Peto, R.; Pan, H.; Potter, J.; Eckstein, H.H.; Farrell, B.; et al. Second asymptomatic carotid surgery trial (ACST-2): A randomised comparison of carotid artery stenting versus carotid endarterectomy. Lancet 2021, 398, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Brassington, K.; Selemidis, S.; Bozinovski, S.; Vlahos, R. Chronic obstructive pulmonary disease and atherosclerosis: Common mechanisms and novel therapeutics. Clin. Sci. 2022, 136, 405–423. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.; Bøtker, H.E.; De Hert, S.; Ford, I.; Juanatey, J.R.G.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: Cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur. J. Anaesthesiol. 2014, 31, 517–573. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bhatt, D.L.; Storey, R.F.; Steg, P.G.; Cohen, M.; Kuder, J.; Goodrich, E.; Nicolau, J.C.; Parkhomenko, A.; López-Sendón, J.; et al. Ticagrelor for Prevention of Ischemic Events After Myocardial Infarction in Patients With Peripheral Artery Disease. J. Am. Coll. Cardiol. 2016, 67, 2719–2728. [Google Scholar] [CrossRef]
- Elbaz-Greener, G.; Rozen, G.; Carasso, S.; Kusniec, F.; Yarkoni, M.; Marai, I.; Strauss, B.; Wijeysundera, H.C.; Smart, F.W.; Erez, E.; et al. The Relationship Between Body Mass Index and In-Hospital Mortality in Patients Following Coronary Artery Bypass Grafting Surgery. Front. Cardiovasc. Med. 2021, 8, 754934. [Google Scholar] [CrossRef]
- Oz, K.; Aydın, Ü.; Kyaruzi, M.; Göksel, O.S.; Yeniterzi, M.; Bakir, I. Staged or Combined Approach for Carotid Endarterectomy in Patients Undergoing Coronary Artery Bypass Grafting: A 5-Year-Long Experience. Heart Surg. Forum. 2016, 19, E276–E281. [Google Scholar] [CrossRef]
- Kawashima, H.; Serruys, P.W.; Ono, M.; Hara, H.; O’leary, N.; Mack, M.J.; Holmes, D.R.; Morice, M.-C.; Head, S.J.; Kappetein, A.P.; et al. Impact of Optimal Medical Therapy on 10-Year Mortality After Coronary Revascularization. J. Am. Coll. Cardiol. 2021, 78, 27–38. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group 1 | Group 2 | p-Value |
|---|---|---|---|
| CABG + CEA (n = 106) | CABG/CEA (n = 86) | ||
| Anthropometric data | |||
| Gender, n (%) | M—90 (84.9) F—16 (15.1) | M—66 (76.7) F—20 (23.3) | 0.150 |
| Age, years, Me [IQR] | 64 [60–69] | 66 [61–69] | 0.115 |
| BMI, kg/m2, Me [M ± SD] | 28.20 ± 3.68 | 29.35 ± 4.09 | 0.041 * |
| Clinical and anamnestic data, risk factors, comorbidity | |||
| III-IV angina (CCS), n (%) | 91 (85.8) 15 (14.2) | 78 (90.7) 8 (9.3) | 0.304 |
| Previous MI, n (%) | 44 (41.5) | 36 (41.9) | 0.961 |
| Previous Stroke, n (%) | 21 (19.8) | 17 (19.8) | 0.994 |
| Hypertension, n (%) | 106 (100) | 84 (97.7) | 0.199 |
| Smoking, n (%) | 46 (43.4) | 20 (23.3) | 0.003 * |
| CKD, n (%) | 24 (24.4) | 16 (18.6) | 0.493 |
| Diabetes, n (%) | 22 (20.8) | 28 (32.6) | 0.064 |
| COPD, n (%) | 10 (9.5) | 2 (2.3) | 0.069 |
| Diagnostic data | |||
| LV EF, %, Me [IQR] | 55 [52–55] | 55 [51–56] | 0.090 |
| One-vessel disease, n (%) | 5 (4.7) | 2 (2.3) | 0.463 |
| Two-vessel disease, n (%) | 24 (22.6) | 15 (17.4) | 0.373 |
| Three-vessel disease, n (%) | 77 (72.6) | 68 (79.1) | 0.303 |
| LCA trunk disease > 50%, n (%) | 40 (38.1) | 25 (29.4) | 0.207 |
| Target CA stenosis, %, Me [IQR] | 77 [70–90] | 77 [70–87] | 0.387 |
| Linear velocity of the blood flow in target CA, cm/s, Me [IQR] | 247 [187–279] | 246 [208–291] | 0.848 |
| Bilateral CA stenosis > 70%, n (%) | 10 (9.4) | 8 (9.3) | 1.0 |
| Stenosis of the renal arteries > 70%, n (%) | 2 (1.9) | 0 | 0.503 |
| Lower extremity artery stenosis > 70%, n (%) | 9 (8.5) | 6 (6.9) | 0.791 |
| Interventions data | |||
| CABG off-pump, n (%) | 32 (30.2) | 26 (30.2) | 0.995 |
| CABG CPB, n (%) | 74 (69.8) | 60 (69.8) | |
| LITA to the LAD, n (%) | 83 (78.3) | 76 (88.4) | 0.066 |
| CPB time, min, [M ± SD] | 70.3 ± 12.4 | 72.4 ± 11.9 | 0.788 |
| Eversion CEA, n (%) | 65 (61.3) | 49 (57.0) | 0.542 |
| CEA with a synthetic patch angioplasty, n (%) | 41 (38.7) | 37 (43.0) | |
| Complications | Group 1 | Group 2 | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| CABG + CEA (n = 106) | CABG/CEA (n = 86) | ||||
| Complications | |||||
| Death, n (%) | 3 (2.8) | 2 (2.3) | 1.233 | 0.133–5.006 | 1.0 |
| Non-fatal MI, n (%) | 0 | 2 (2.3) | 6.302 | 0.299–133.032 | 0.199 |
| Non-fatal stroke, n (%) | 3 (2.8) | 1 (1.2) | 2.476 | 0.041–3.954 | 0.629 |
| MACEs, n (%) | 6 (5.7) | 5 (5.8) | 1.029 | 0.303–3.493 | 1.0 |
| Brain swelling, n (%) | 2 (1.9) | 0 | 4.139 | 0.011–5.100 | 0.503 |
| GI bleed, n (%) | 1 (0.9) | 0 | 2.406 | 0.016–10.106 | 1.0 |
| Respiratory failure, n (%) | 2 (1.9) | 1 (1.2) | 1.635 | 0.055–6.863 | 1.0 |
| Heart rhythm disorders, n (%) | 8 (7.5) | 4 (4.7) | 1.673 | 0.174–2.056 | 0.553 |
| Acute heart failure, n (%) | 2 (1.9) | 2 (2.3) | 1.238 | 0.171–8.976 | 1.0 |
| Multiple organ failure, n (%) | 2 (1.9) | 2 (2.3) | 1.238 | 0.171–8.976 | 1.0 |
| Duration of mechanical ventilation, h, Me [IQR] | 15.5 [10.0–18.1] | 11.5 [8.0–16.2] | 0.004 * | ||
| Rethoracotomy for bleeding, n (%) | 7 (6.6) | 6 (7.0) | 1.061 | 0.343–3.282 | 1.0 |
| Infectious complications, n (%) | 7 (6.6) | 2 (2.3) | 2.970 | 0.068–1.665 | 0.191 |
| Risk of complications | |||||
| Number of patients with 1 or more any postoperative complication, n (%) | 28 (26.4) | 12 (14.0) | 2.214 | 1.048–4.674 | 0.035 * |
| Risk Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age per 1 y | 1.16 (0.05–1.28) | 0.004 * | 1.15 (1.03–1.27) | 0.01 * |
| Female | 1.68 (0.42–6.68) | 0.460 | - | - |
| BMI per 1 kg/m2 | 0.81 (0.66–0.97) | 0.023 * | 0.81 (0.66–1.01) | 0.057 |
| Smoking | 1.64 (0.48–5.58) | 0.429 | - | - |
| Previous stroke | 2.47 (0.68–8.92) | 0.167 | - | - |
| Previous MI | 2.59 (0.73–9.16) | 0.140 | ||
| Bilateral CA stenosis | 0.96 (0.12–8.00) | 0.973 | - | - |
| LV EF | 0.94 (0.71–1.64) | 0.647 | - | - |
| Three-vessel disease | 3.41 (0.42–27.35) | 0.249 | - | - |
| LCA trunk disease > 50% | 0.42 (0.09–1.99) | 0.272 | - | - |
| Lower extremity artery stenosis | 1.19 (0.14–10.00) | 0.871 | - | - |
| Diabetes | 1.07 (0.27–4.20) | 0.924 | - | - |
| CKD | 0.36 (0.04–2.93) | 0.342 | - | - |
| COPD | 3.80 (0.72–19.98) | 0.115 | - | - |
| CABG CPB | 1.16 (0.30–4.55) | 0.827 | - | - |
| Stage | 1.03 (0.31–3.49) | 0.964 | - | - |
| Risk Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age per 1 y | 1.01 (0.97–1.04) | 0.850 | - | - |
| BMI per increase 1 kg/m2 | 0.92 (0.86–0.99) | 0.035 * | 0.93 (0.85–0.99) | 0.036 * |
| Smoking | 1.87 (1.10–3.18) | 0.021 * | - | - |
| Female | 1.47 (0.82–2.64) | 0.198 | - | - |
| Previous stroke | 1.34 (0.72–2.49) | 0.348 | - | - |
| Previous MI | 1.01 (0.56–1.68) | 0.988 | - | - |
| Bilateral CA stenosis | 1.01 (0.43–2.35) | 0.979 | - | - |
| LV EF | 1.03 (0.91–1.17) | 0.621 | - | - |
| Three-vessel disease | 0.53 (0.31–0.98) | 0.063 | - | - |
| LCA trunk disease > 50% | 1.34 (0.79–2.28) | 0.282 | - | - |
| Lower extremity artery stenosis | 0.85 (0.31–2.35) | 0.758 | - | - |
| Diabetes | 0.84 (0.48–1.50) | 0.566 | - | - |
| CKD | 1.34 (0.73–2.44) | 0.341 | - | - |
| COPD | 1.56 (0.62–3.91) | 0.341 | - | - |
| CABG CPB | 1.47 (0.83–2.62) | 0.186 | - | - |
| Stage | 0.62 (0.37–1.04) | 0.069 | - | - |
| Risk Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age per 1 y | 1.01 (0.98–1.03) | 0.814 | - | - |
| Female | 1.14 (0.76–1.70) | 0.523 | - | - |
| BMI per 1 kg/m2 | 0.95 (0.91–0.99) | 0.042 * | 0.96 (0.92–1.01) | 0.080 |
| Smoking | 1.44 (1.01–2.04) | 0.043 * | 1.36 (0.95–1.94) | 0.09 |
| Previous Stroke | 1.12 (0.74–1.70) | 0.583 | - | - |
| Previous MI | 0.92 (0.66–1.29) | 0.629 | ||
| Bilateral CA stenosis | 0.96 (0.55–1.67) | 0.896 | - | - |
| LV EF | 0.94 (0.87–1.02) | 0.135 | - | - |
| Three-vessel disease | 0.76 (0.52–1.12) | 0.164 | - | - |
| LCA trunk disease > 50% | 1.19 (0.84–1.68) | 0.331 | - | - |
| Lower extremity artery stenosis | 1.08 (0.60–1.95) | 0.803 | - | - |
| Diabetes | 0.82 (0.57–1.19) | 0.820 | - | - |
| CKD | 1.35 (0.92–1.97) | 0.124 | - | - |
| COPD | 1.40 (0.76–2.59) | 0.283 | - | - |
| CABG CPB | 1.64 (1.12–2.28) | 0.082 | - | - |
| Stage | 0.715 (0.50–1.01) | 0.060 | - | - |
| Risk Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age per 1 y | 0.99 (0.95–1.04) | 0.899 | - | - |
| Female | 0.81 (0.34–1.94) | 0.638 | - | - |
| BMI per 1 kg/m2 | 1.03 (0.95–1.11) | 0.510 | - | - |
| Smoking | 1.71 (0.88–3.35) | 0.114 | - | - |
| Previos Stroke | 1.08 (0.47–2.46) | 0.851 | - | - |
| Previous MI | 0.99 (0.32–1.26) | 0.194 | - | - |
| Bilateral CA stenosis | 1.06 (0.38–0.99) | 0.913 | - | - |
| LV EF | 0.84 (0.73–0.98) | 0.022 * | 0.87 (0.74–1.01) | 0.061 |
| Three-vessel disease | 0.80 (0.38–1.70) | 0.568 | - | - |
| LCA trunk disease > 50% | 0.74 (0.35–1.58) | 0.442 | - | - |
| Lower extremity artery stenosis | 2.24 (0.94–5.37) | 0.069 | 2.45 (1.20–7.23) | 0.018 * |
| Diabetes | 0.94 (0.46–1.89) | 0.856 | - | - |
| CKD | 0.94 (0.42–2.15) | 0.892 | - | - |
| COPD | 3.19 (1.33–7.66) | 0.009 * | 2.89 (1.17–7.13) | 0.021 * |
| CABG CPB | 1.93 (0.48–1.81) | 0.839 | - | - |
| Stage | 0.64 (0.34–1.21) | 0.169 | - | - |
| Risk Factors | Univariate Analysis | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Age per 1 y | 1.01 (0.96–1.04) | 0.879 |
| Female | 0.88 (0.41–1.88) | 0.745 |
| BMI per 1 kg/m2 | 0.96 (0.89–1.04) | 0.365 |
| Smoking | 0.82 (0.42–1.63) | 0.577 |
| Previous stroke | 0.92 (0.43–1.97) | 0.829 |
| Previous MI | 1.08 (0.61–1.92) | 0.780 |
| Bilateral CA stenosis | 0.83 (0.30–2.30) | 0.715 |
| LV EF | 0.90 (0.79–1.03) | 0.121 |
| Three-vessel disease | 1.30 (0.61–2.78) | 0.500 |
| LCA trunk disease > 50% | 1.42 (0.79–2.56) | 0.236 |
| Lower extremity artery stenosis | 0.80 (0.95–2.58) | 0.710 |
| Diabetes | 0.87 (0.46–1.64) | 0.665 |
| CKD | 1.56 (0.83–2.96) | 0.169 |
| COPD | 0.05 (0.01–10.74) | 0.268 |
| CABG CPB | 2.02 (0.86–4.06) | 0.115 |
| Stage | 0.772 (0.443–1.347) | 0.364 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golukhova, E.; Sigaev, I.; Keren, M.; Slivneva, I.; Berdibekov, B.; Sheikina, N.; Kozlova, O.; Arakelyan, V.; Volkovskaya, I.; Zavalikhina, T.; et al. Early and Long-Term Results of Simultaneous and Staged Revascularization of Coronary and Carotid Arteries. Pathophysiology 2024, 31, 210-224. https://doi.org/10.3390/pathophysiology31020017
Golukhova E, Sigaev I, Keren M, Slivneva I, Berdibekov B, Sheikina N, Kozlova O, Arakelyan V, Volkovskaya I, Zavalikhina T, et al. Early and Long-Term Results of Simultaneous and Staged Revascularization of Coronary and Carotid Arteries. Pathophysiology. 2024; 31(2):210-224. https://doi.org/10.3390/pathophysiology31020017
Chicago/Turabian StyleGolukhova, Elena, Igor Sigaev, Milena Keren, Inessa Slivneva, Bektur Berdibekov, Nina Sheikina, Olga Kozlova, Valery Arakelyan, Irina Volkovskaya, Tatiana Zavalikhina, and et al. 2024. "Early and Long-Term Results of Simultaneous and Staged Revascularization of Coronary and Carotid Arteries" Pathophysiology 31, no. 2: 210-224. https://doi.org/10.3390/pathophysiology31020017