Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression





Abstract
:1. Introduction
2. Materials and Methods
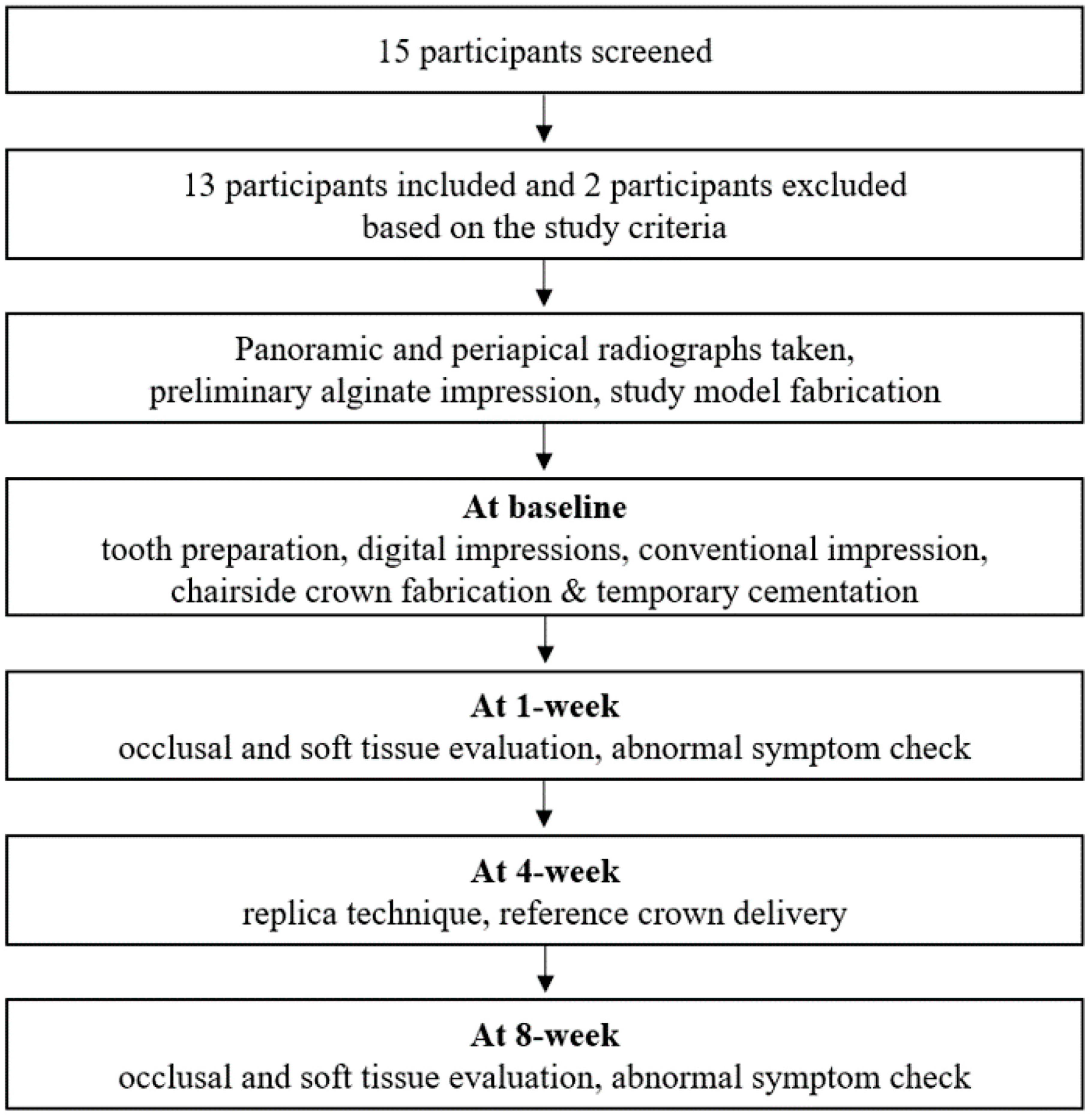
2.1. Clinical Study Design
- (1)
- Patients aged 19–70 years;
- (2)
- Patients in need of a tooth-supported crown in the posterior region (premolar or first molar);
- (3)
- Presence of healthy abutment and adjacent teeth without the need for additional treatment;
- (4)
- Normal occlusal plane of the opposite teeth;
- (5)
- Tooth with a finishing line that could be formed supragingivally;
- (6)
- Absence of temporomandibular or occlusal disorders;
- (7)
- Patients who participated voluntarily in this clinical trial and signed the informed consent.
- (1)
- Pregnancy;
- (2)
- Mental illness;
- (3)
- Allergy to the restorative material;
- (4)
- Symptomatic teeth requiring additional endodontic treatment;
- (5)
- Periodontally involved teeth;
- (6)
- Presence of parafunctional habits;
- (7)
- Inadequate crown height.
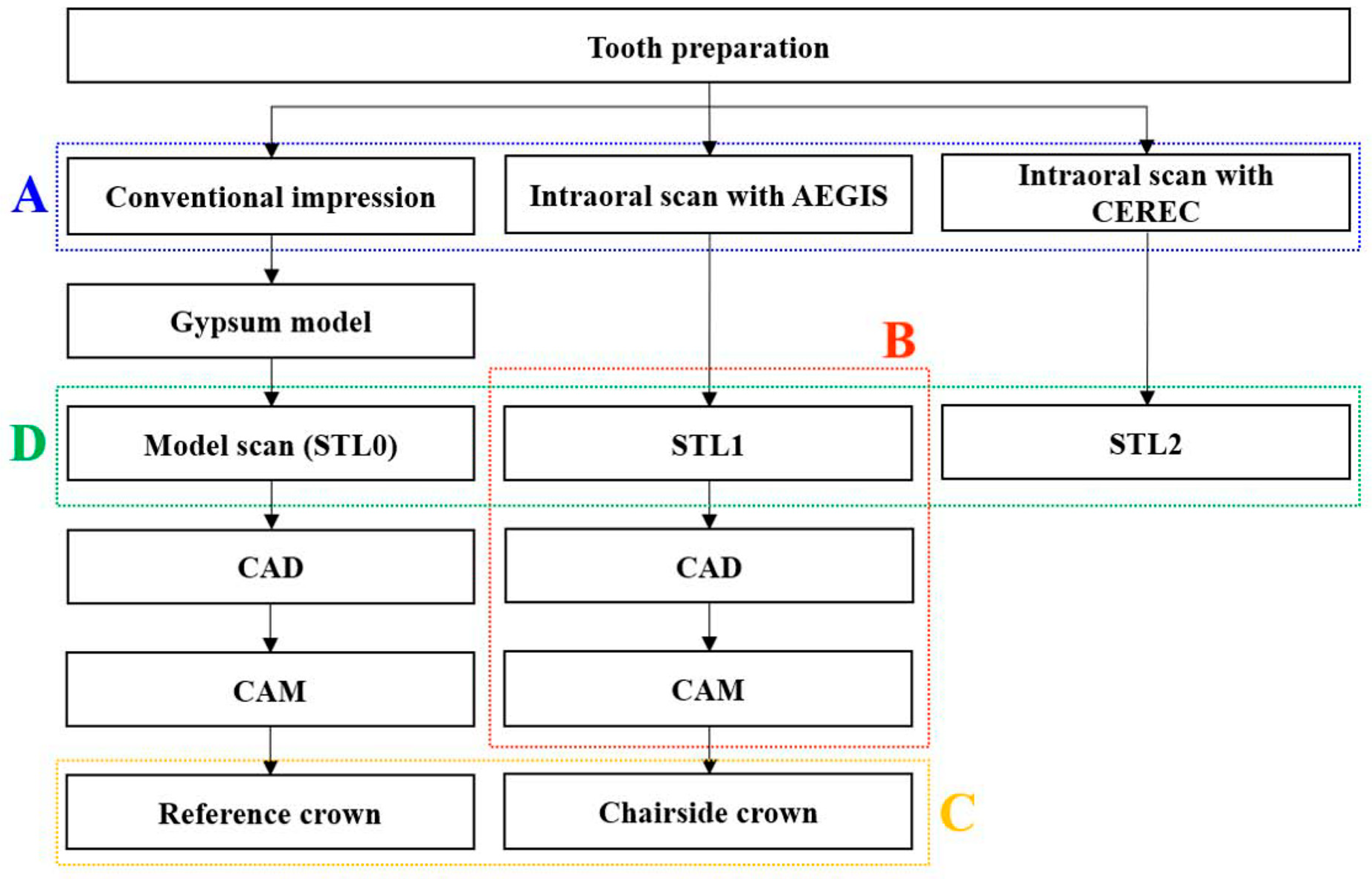
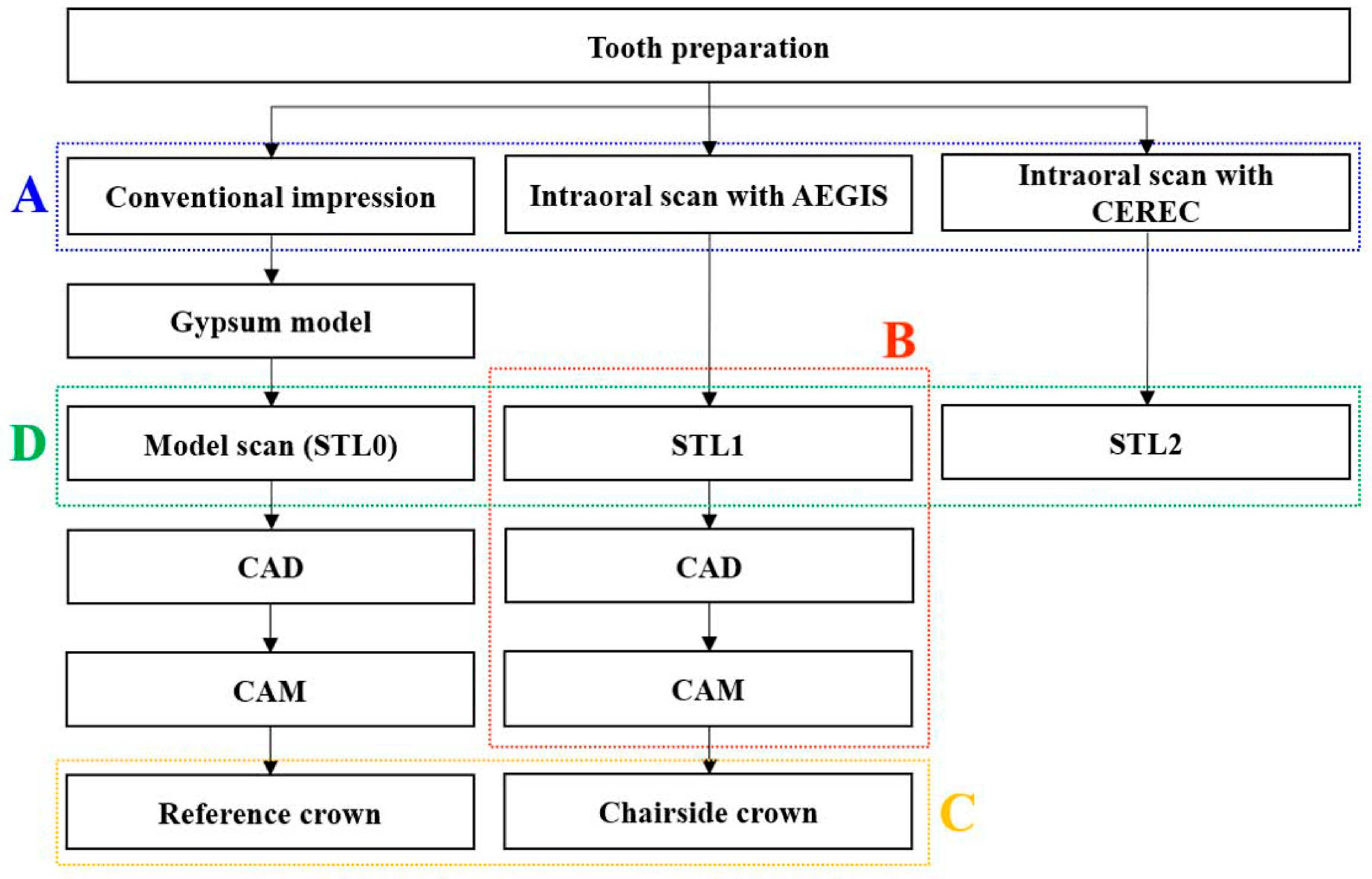
2.2. Clinical Procedures
2.2.1. Tooth Preparation
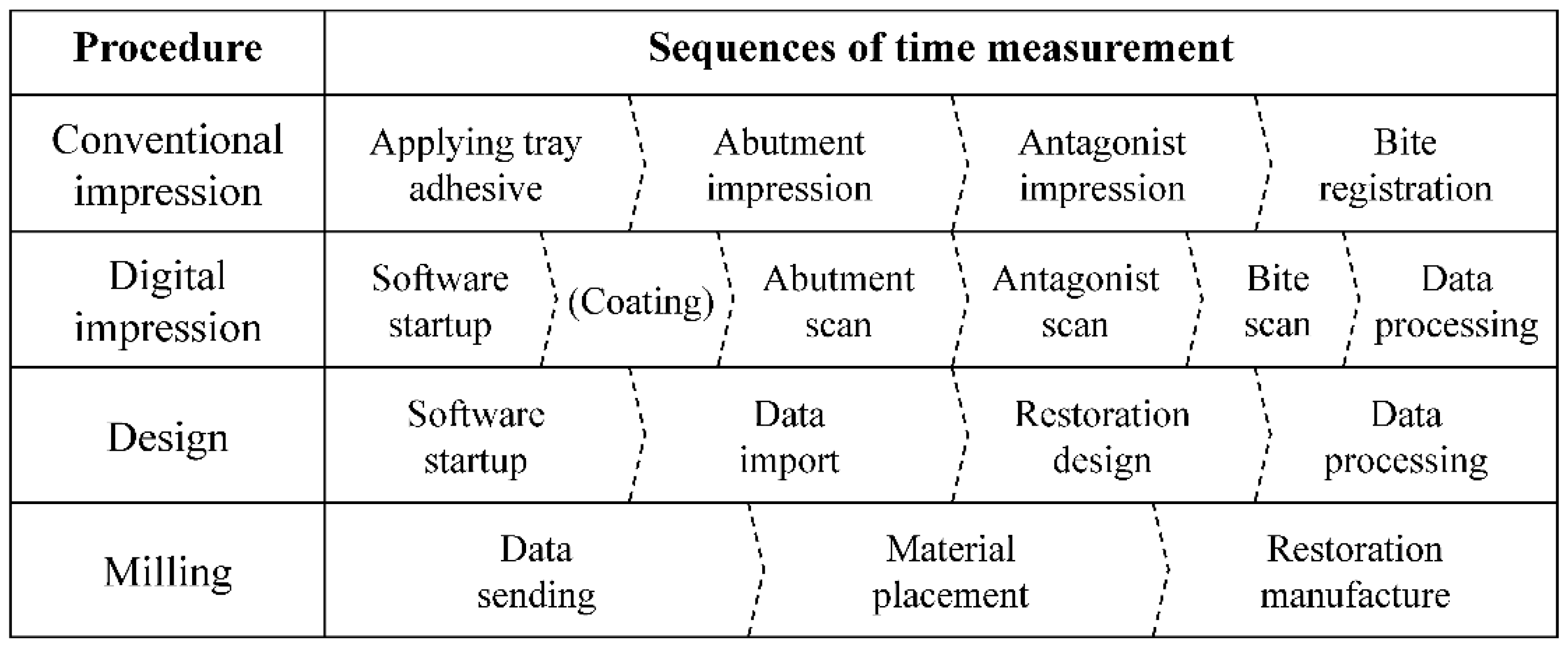
2.2.2. Conventional Impression
2.2.3. Digital Impressions
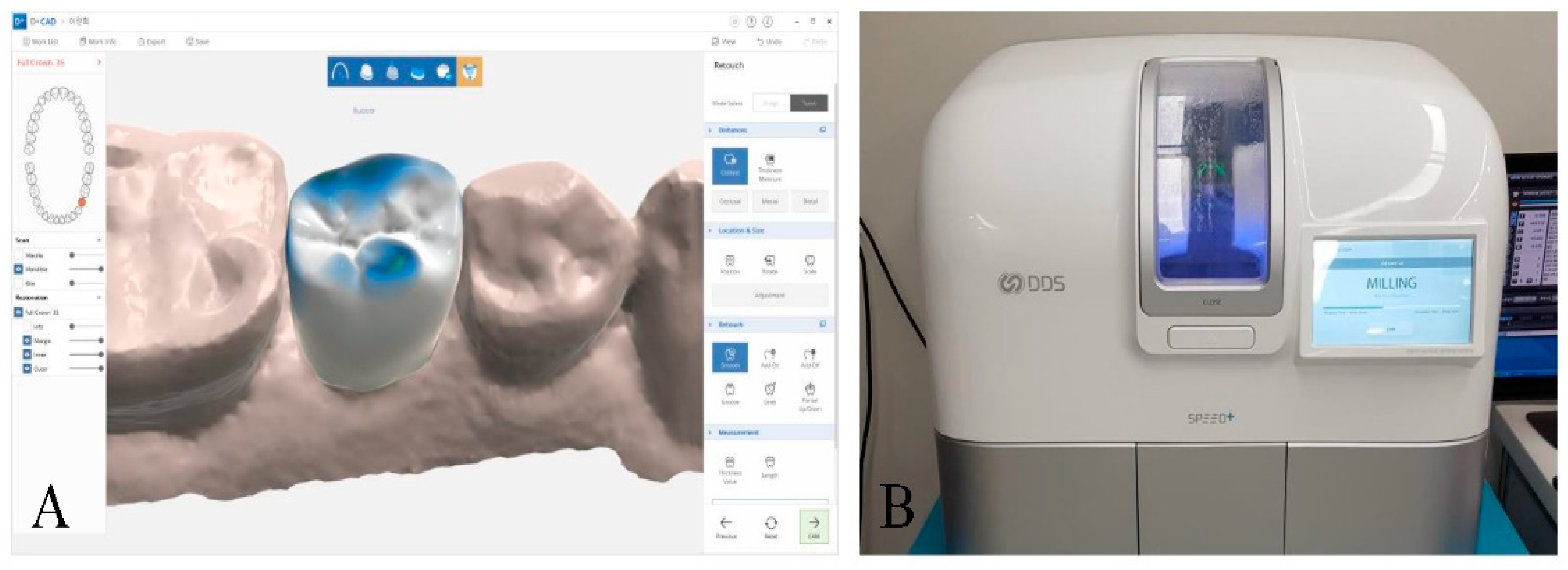
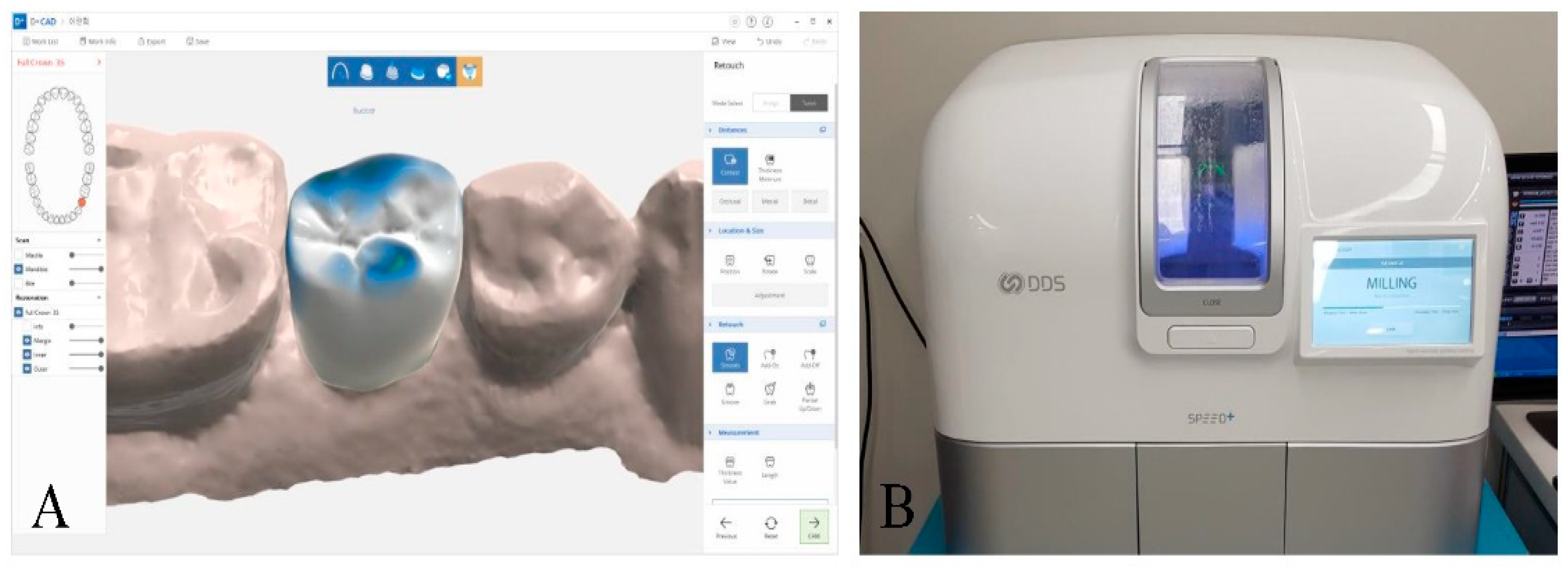
2.2.4. Chairside Crown Fabrication
2.2.5. Reference Crown Fabrication and Delivery
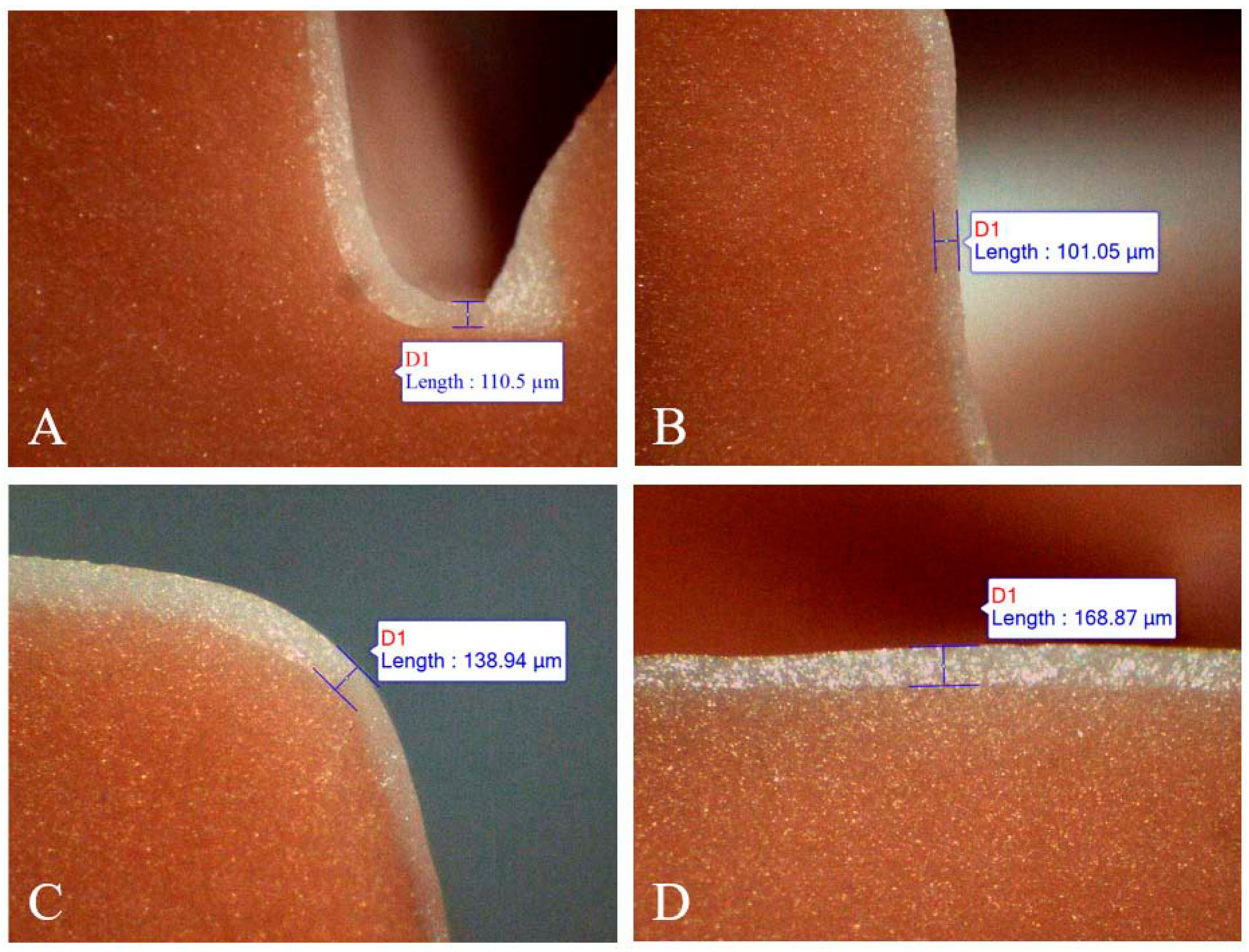
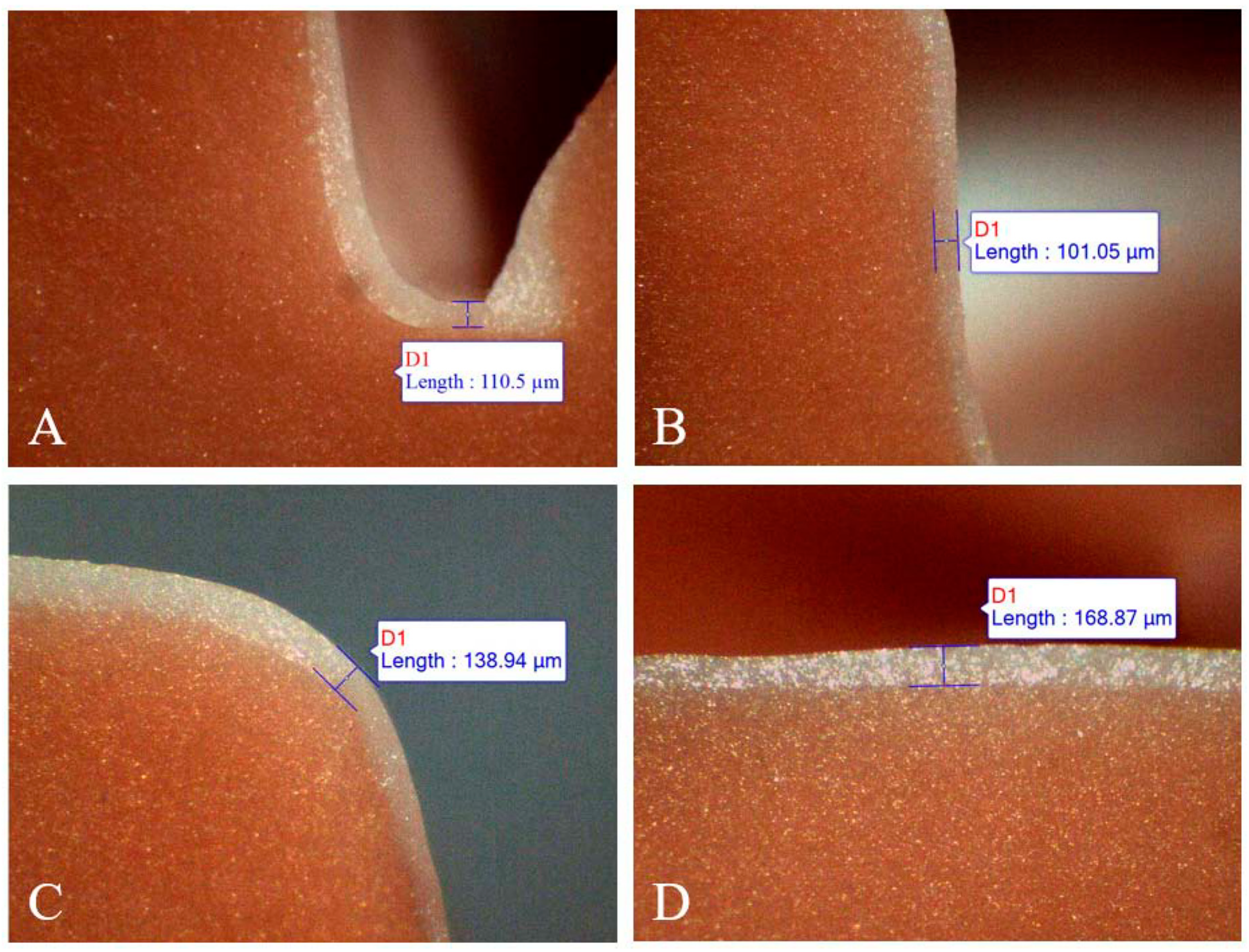
2.3. Replica Measurement
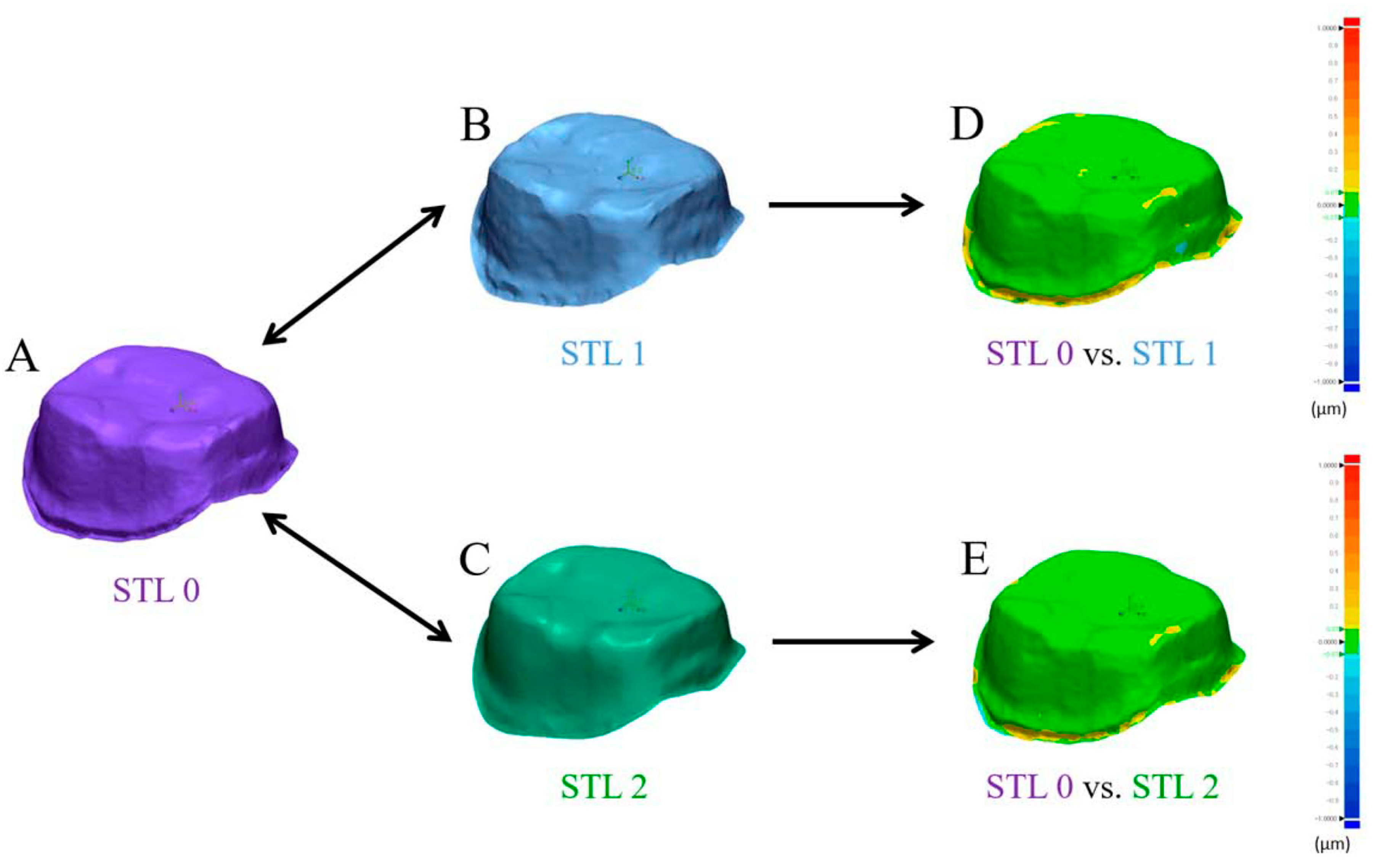
2.4. Best-Fit Alignment
2.5. Statistical Analysis
3. Results
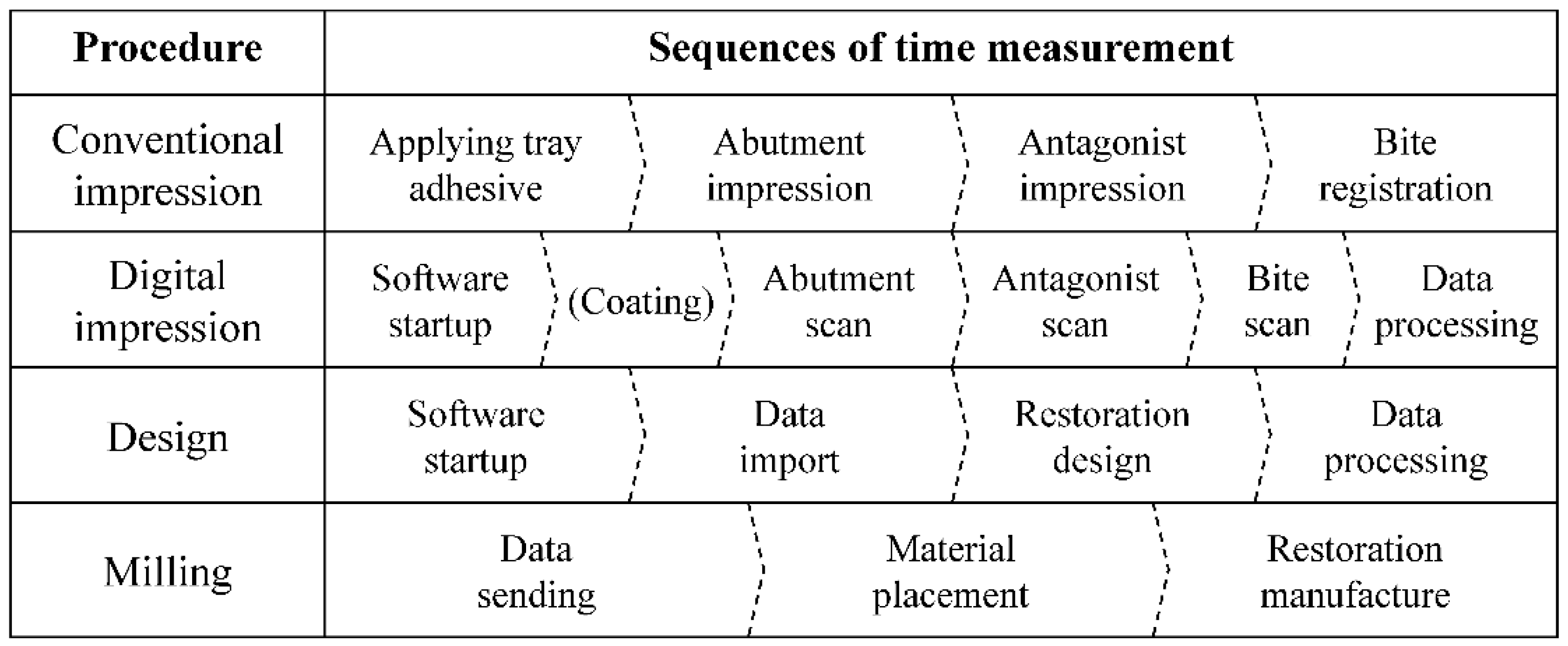
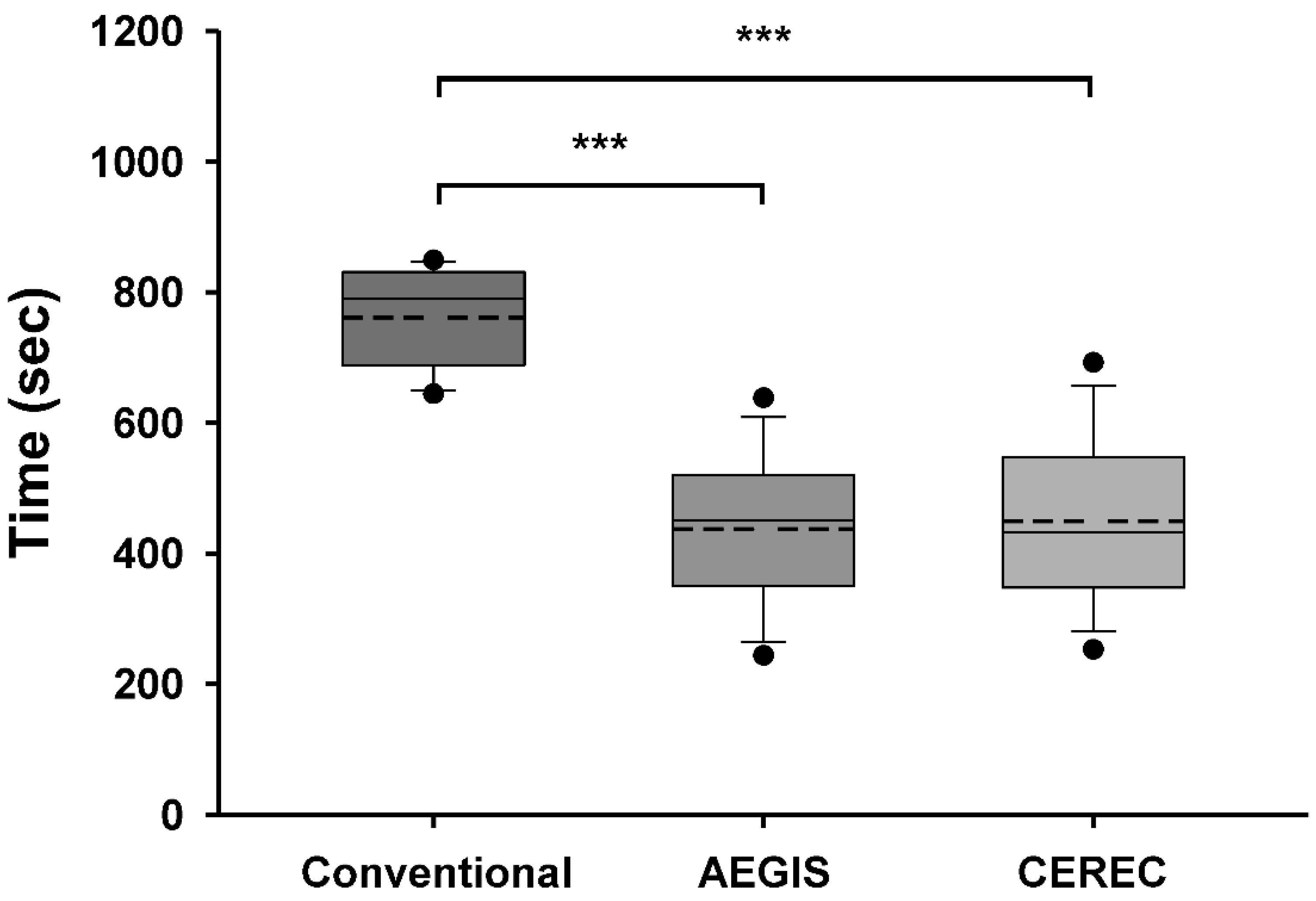
3.1. Comparison of Time Taken for Impression
3.2. Total Working Time for the Chairside Crown by the AEGIS Stystem
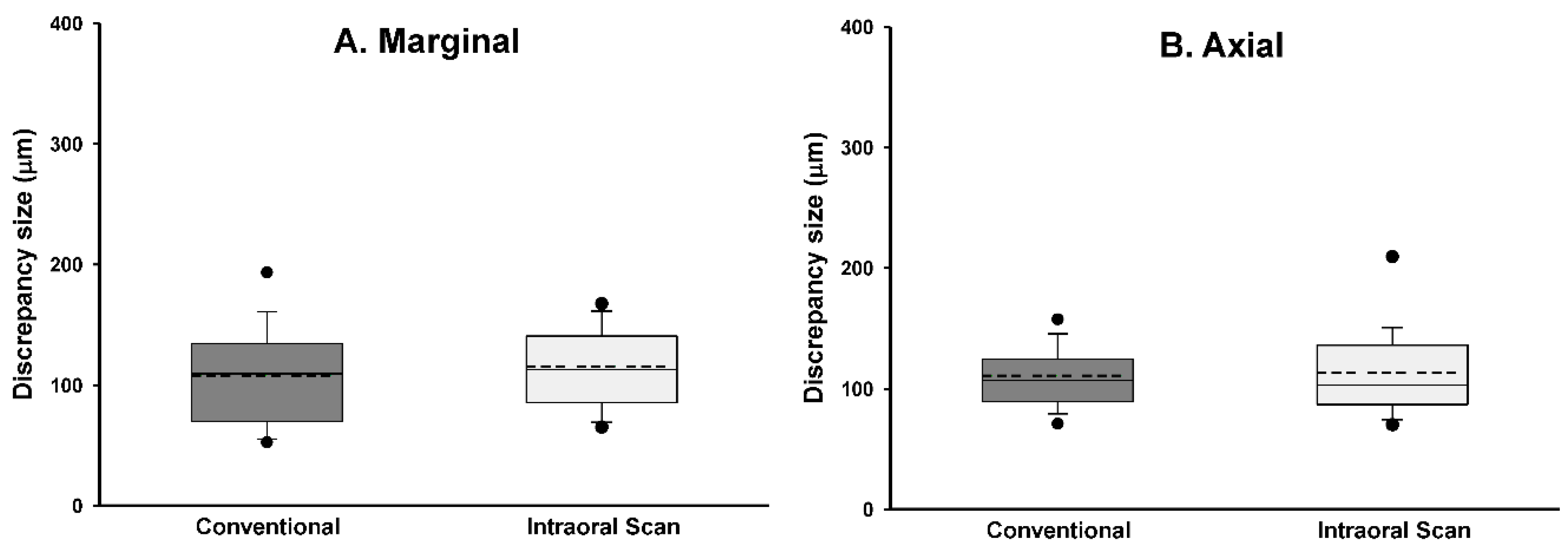
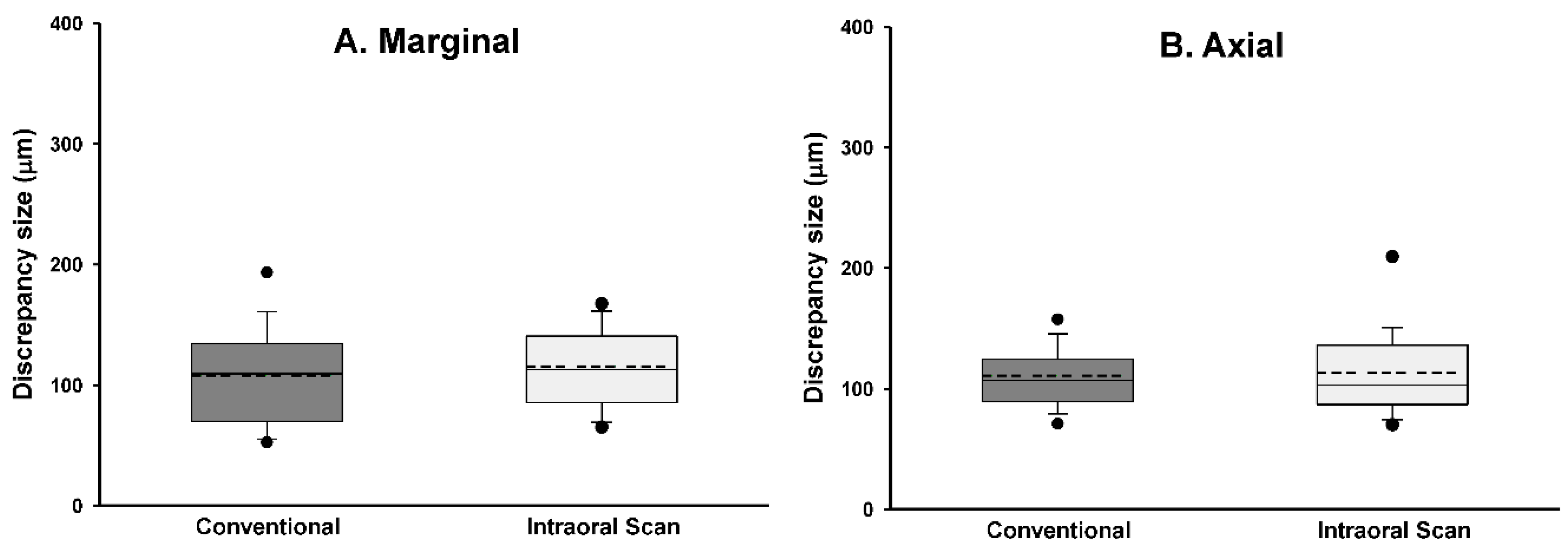
3.3. Marginal and Internal Fit
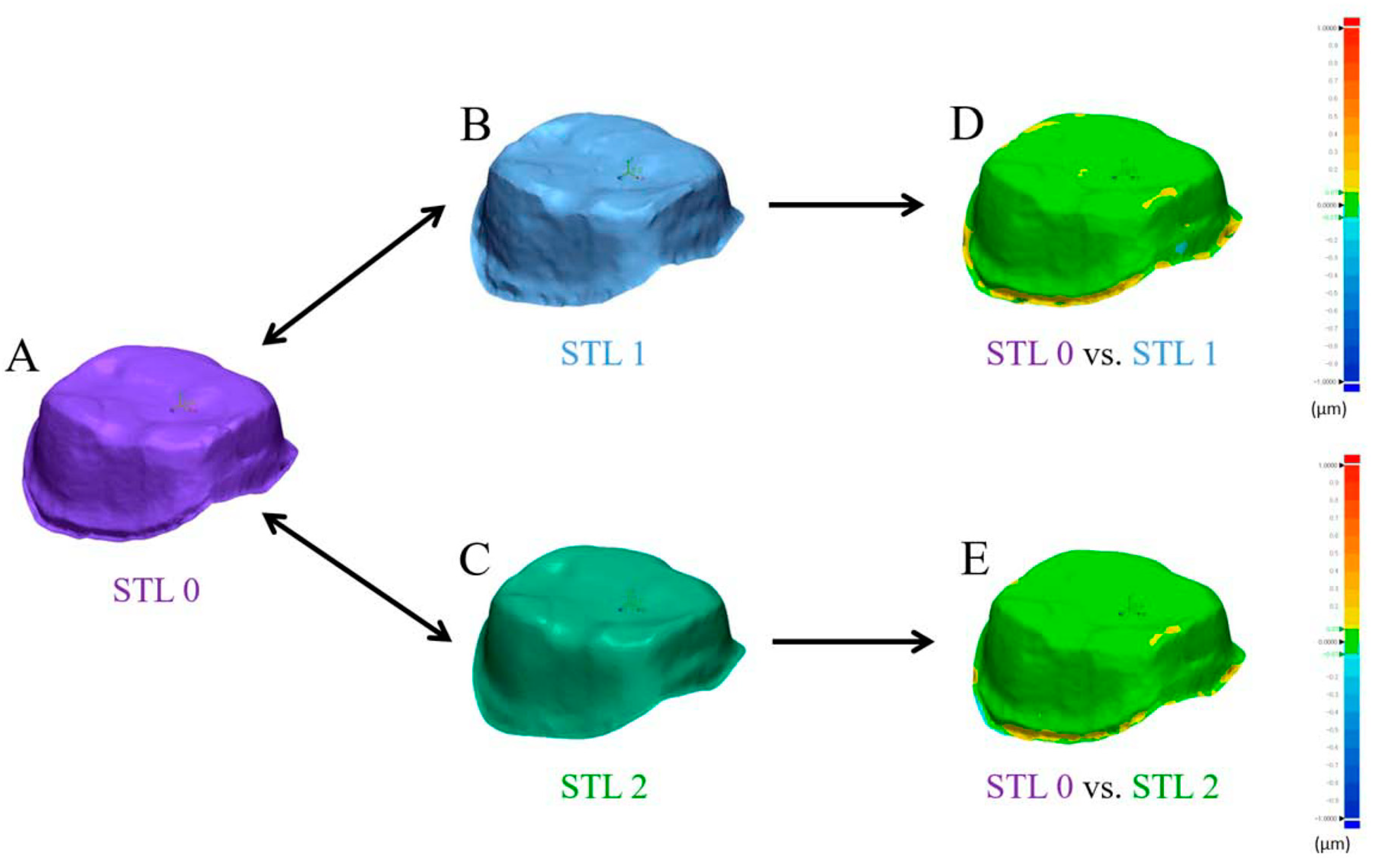
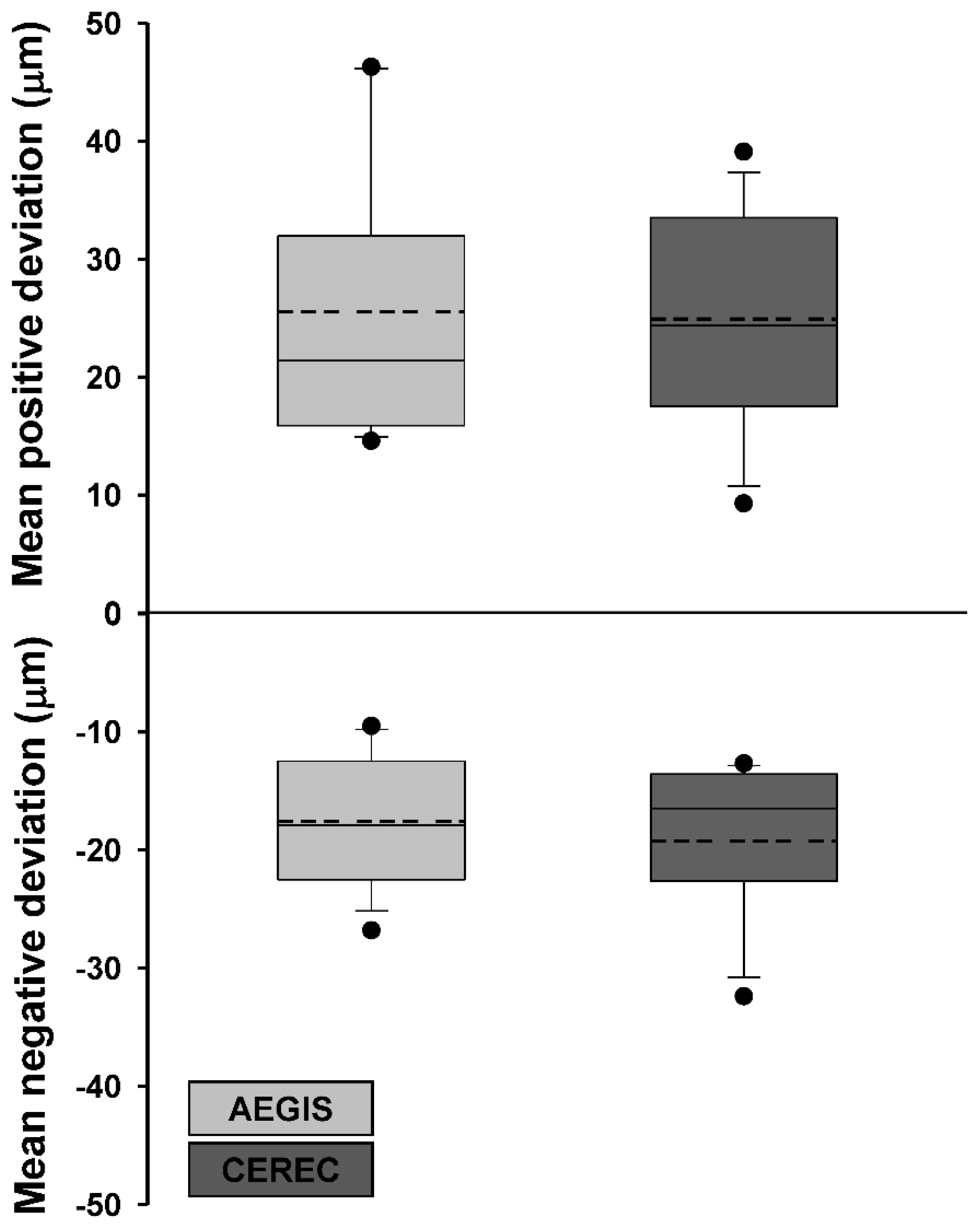
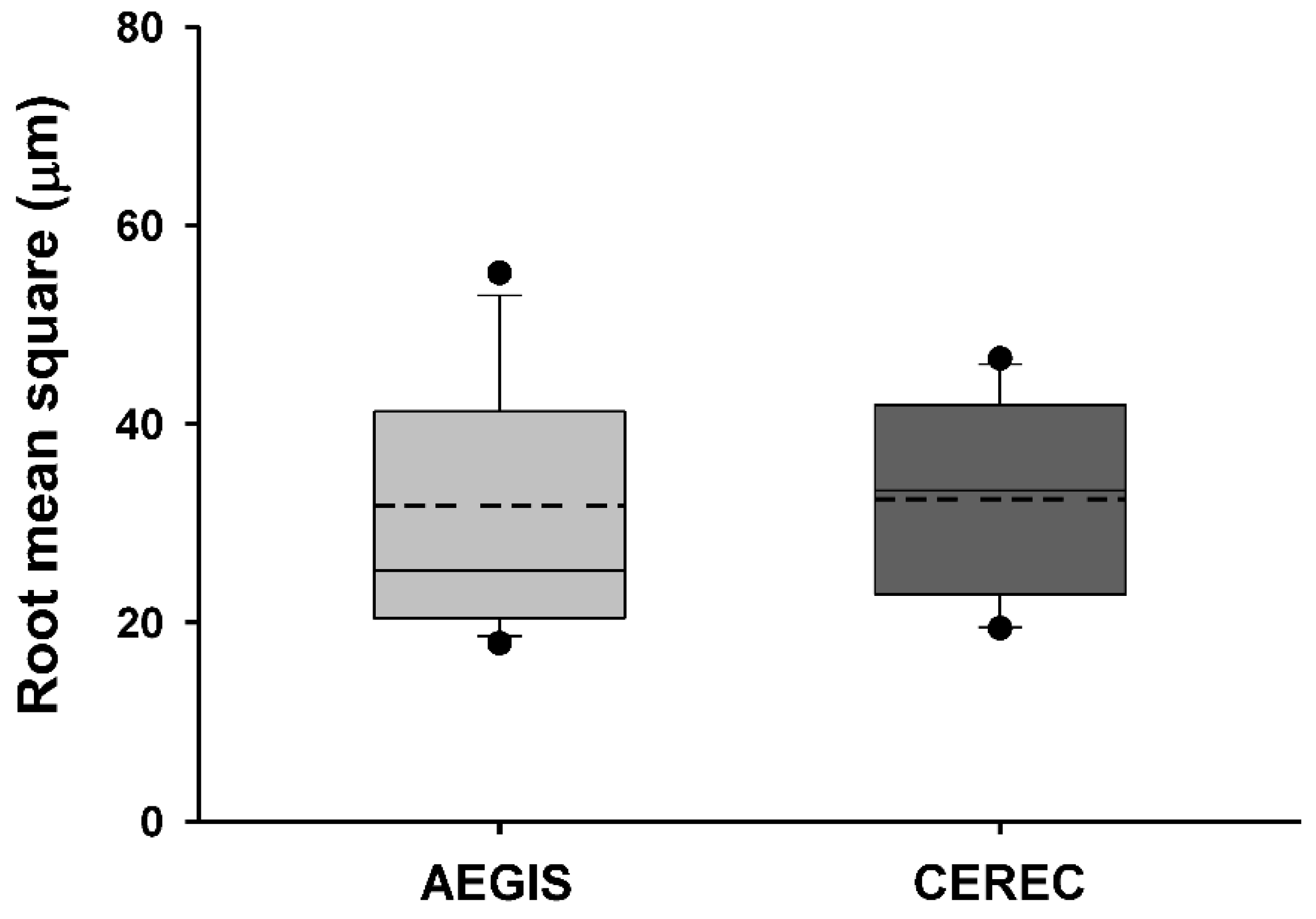
3.4. Accuracy of Intraoral Scanners
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schoenbaum, T.R. Dentistry in the digital age: An update. Dent. Today 2012, 31, 108–113. [Google Scholar]
- Joda, T.; Brägger, U. Time-Efficiency Analysis Comparing Digital and Conventional Workflows for Implant Crowns: A Prospective Clinical Crossover Trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Fasbinder, D.J. Digital dentistry: Innovation for restorative treatment. Compend. Contin. Educ. Dent. 2010, 31, 2–12. [Google Scholar]
- Fasbinder, D.J. Materials for chairside CAD/CAM restorations. Compend. Contin. Educ. Dent. 2010, 31, 702–709. [Google Scholar]
- Vichi, A.; Sedda, M.; Del Siena, F.; Louca, C.; Ferrari, M. Flexural resistance of Cerec CAD/CAM system ceramic blocks. Part 1: Chairside materials. Am. J. Dent. 2013, 26, 255–259. [Google Scholar]
- Vivadent, I. IPS e. Max Lithium Disilicate: The Future of All Ceramic Dentistry Material Science, Practical Applications, Keys to Success; Ivoclar Vivadent: Amherst, MA, USA; New York, NY, USA, 2009; pp. 1–15. [Google Scholar]
- van den Breemer, C.R.; Vinkenborg, C.; van Pelt, H.; Edelhoff, D.; Cune, M.S. The Clinical Performance of Monolithic Lithium Disilicate Posterior Restorations After 5, 10, and 15 Years: A Retrospective Case Series. Int. J. Prosthodont. 2017, 30, 62–65. [Google Scholar] [CrossRef] [Green Version]
- Rauch, A.; Reich, S.; Dalchau, L.; Schierz, O. Clinical survival of chair-side generated monolithic lithium disilicate crowns:10-year results. Clin. Oral Investig. 2018, 22, 1763–1769. [Google Scholar] [CrossRef]
- Fasbinder, D.J.; Dennison, J.B.; Heys, D.; Neiva, G. A clinical evaluation of chairside lithium disilicate CAD/CAM crowns: A two-year report. J. Am. Dent. Assoc. 2010, 141 (Suppl. 2), 10–14. [Google Scholar] [CrossRef]
- Baig, M.R.; Tan, K.B.; Nicholls, J.I. Evaluation of the marginal fit of a zirconia ceramic computer-aided machined (CAM) crown system. J. Prosthet. Dent. 2010, 104, 216–227. [Google Scholar] [CrossRef]
- Pak, H.S.; Han, J.S.; Lee, J.B.; Kim, S.H.; Yang, J.H. Influence of porcelain veneering on the marginal fit of Digident and Lava CAD/CAM zirconia ceramic crowns. J. Adv. Prosthodont. 2010, 2, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, M.S.; Windeler, A.S. An investigation of dental luting cement solubility as a function of the marginal gap. J. Prosthet. Dent. 1991, 65, 436–442. [Google Scholar] [CrossRef]
- Demir, N.; Ozturk, A.N.; Malkoc, M.A. Evaluation of the marginal fit of full ceramic crowns by the microcomputed tomography (micro-CT) technique. Eur. J. Dent. 2014, 8, 437–444. [Google Scholar] [CrossRef]
- Tan, P.L.; Gratton, D.G.; Diaz-Arnold, A.M.; Holmes, D.C. An in vitro comparison of vertical marginal gaps of CAD/CAM titanium and conventional cast restorations. J. Prosthodont. 2008, 17, 378–383. [Google Scholar] [CrossRef]
- Holmes, J.R.; Bayne, S.C.; Holland, G.A.; Sulik, W.D. Considerations in measurement of marginal fit. J. Prosthet. Dent. 1989, 62, 405–408. [Google Scholar] [CrossRef]
- Suárez, M.J.; González de Villaumbrosia, P.; Pradíes, G.; Lozano, J.F. Comparison of the marginal fit of Procera AllCeram crowns with two finish lines. Int. J. Prosthodont. 2003, 16, 229–232. [Google Scholar]
- Coli, P.; Karlsson, S. Fit of a new pressure-sintered zirconium dioxide coping. Int. J. Prosthodont. 2004, 17, 59–64. [Google Scholar]
- Neves, F.D.; Prado, C.J.; Prudente, M.S.; Carneiro, T.A.; Zancopé, K.; Davi, L.R.; Mendonca, G.; Cooper, L.F.; Soares, C.J. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. J. Prosthet. Dent. 2014, 112, 1134–1140. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Strub, J.R.; Rekow, E.D.; Witkowski, S. Computer-aided design and fabrication of dental restorations: Current systems and future possibilities. J. Am. Dent. Assoc. 2006, 137, 1289–1296. [Google Scholar] [CrossRef]
- Kapos, T.; Evans, C. CAD/CAM technology for implant abutments, crowns, and superstructures. Int. J. Oral Maxillofac. Implants. 2014, 29, 117–136. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, O.; Schmidt, M.; Goebel, R.; Kuepper, H. Qualitative and quantitative three-dimensional accuracy of a single tooth captured by elastomeric impression materials: An in vitro study. J. Prosthet. Dent. 2012, 108, 165–172. [Google Scholar] [CrossRef]
- Ragain, J.C.; Grosko, M.L.; Raj, M.; Ryan, T.N.; Johnston, W.M. Detail reproduction, contact angles, and die hardness of elastomeric impression and gypsum die material combinations. Int. J. Prosthodont. 2000, 13, 214–220. [Google Scholar]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Ender, A.; Mehl, A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpelä, A.; Mäkynen, A. Recent advances in dental optics–Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Güth, J.F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Eng, J. Sample size estimation: How many individuals should be studied? Radiology 2003, 227, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Suh, K.J.; Lee, K.M. Validity of Intraoral Scans Compared with Plaster Models: An In-Vivo Comparison of Dental Measurements and 3D Surface Analysis. PLoS ONE 2016, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Boening, K.W.; Wolf, B.H.; Schmidt, A.E.; Kästner, K.; Walter, M.H. Clinical fit of Procera AllCeram crowns. J. Prosthet. Dent. 2000, 84, 419–424. [Google Scholar] [CrossRef]
- Wettstein, F.; Sailer, I.; Roos, M.; Hämmerle, C.H. Clinical study of the internal gaps of zirconia and metal frameworks for fixed partial dentures. Eur. J. Oral Sci. 2008, 116, 272–279. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406. [Google Scholar] [CrossRef]
- Gjelvold, B.; Chrcanovic, B.R.; Korduner, E.K.; Collin-Bagewitz, I.; Kisch, J. Intraoral Digital Impression Technique Compared to Conventional Impression Technique. A Randomized Clinical Trial. J. Prosthodont. 2016, 25, 282–287. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Björn, A.L.; Björn, H.; Grkovic, B. Marginal fit of restorations and its relation to periodontal bone level. II. Crowns. Odontol. Revy 1970, 21, 337–346. [Google Scholar]
- Krejci, I.; Krejci, D.; Lutz, F. Clinical evaluation of a new pressed glass ceramic inlay material over 1.5 years. Quintessence Int. 1992, 23, 181–186. [Google Scholar]
- Fransson, B.; Oilo, G.; Gjeitanger, R. The fit of metal-ceramic crowns, a clinical study. Dent. Mater. 1985, 1, 197–199. [Google Scholar] [CrossRef]
- Laurent, M.; Scheer, P.; Dejou, J.; Laborde, G. Clinical evaluation of the marginal fit of cast crowns--validation of the silicone replica method. J. Oral. Rehabil. 2008, 35, 116–122. [Google Scholar] [CrossRef]
- Mounajjed, R.; Layton, D.M.; Azar, B. The marginal fit of E.max Press and E.max CAD lithium disilicate restorations: A critical review. Dent. Mater. J. 2016, 35, 835–844. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Azim, T.; Rogers, K.; Elathamna, E.; Zandinejad, A.; Metz, M.; Morton, D. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J. Prosthet. Dent. 2015, 114, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Dolev, E.; Bitterman, Y.; Meirowitz, A. Comparison of marginal fit between CAD-CAM and hot-press lithium disilicate crowns. J. Prosthet. Dent. 2019, 121, 124–128. [Google Scholar] [CrossRef]
- Kim, J.H.; Jeong, J.H.; Lee, J.H.; Cho, H.W. Fit of lithium disilicate crowns fabricated from conventional and digital impressions assessed with micro-CT. J. Prosthet. Dent. 2016, 116, 551–557. [Google Scholar] [CrossRef]
- Zeltner, M.; Sailer, I.; Mühlemann, S.; Özcan, M.; Hämmerle, C.H.; Benic, G.I. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part III: Marginal and internal fit. J. Prosthet. Dent. 2017, 117, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Alfaro, D.P.; Ruse, N.D.; Carvalho, R.M.; Wyatt, C.C. Assessment of the Internal Fit of Lithium Disilicate Crowns Using Micro-CT. J. Prosthodont. 2015, 24, 381–386. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Accuracy of crowns based on digital intraoral scanning compared to conventional impression-a split-mouth randomised clinical study. Clin. Oral Investig. 2019, 23, 4043–4050. [Google Scholar] [CrossRef]
- Berrendero, S.; Salido, M.P.; Valverde, A.; Ferreiroa, A.; Pradíes, G. Influence of conventional and digital intraoral impressions on the fit of CAD/CAM-fabricated all-ceramic crowns. Clin. Oral Investig. 2016, 20, 2403–2410. [Google Scholar] [CrossRef]
- Syrek, A.; Reich, G.; Ranftl, D.; Klein, C.; Cerny, B.; Brodesser, J. Clinical evaluation of all-ceramic crowns fabricated from intraoral digital impressions based on the principle of active wavefront sampling. J. Dent. 2010, 38, 553–559. [Google Scholar] [CrossRef]
- Luthardt, R.G.; Loos, R.; Quaas, S. Accuracy of intraoral data acquisition in comparison to the conventional impression. Int. J. Comput. Dent. 2005, 8, 283–294. [Google Scholar]
- Mehl, A.; Ender, A.; Mörmann, W.; Attin, T. Accuracy testing of a new intraoral 3D camera. Int. J. Comput. Dent. 2009, 12, 11–28. [Google Scholar]
- Steinhäuser-Andresen, S.; Detterbeck, A.; Funk, C.; Krumm, M.; Kasperl, S.; Holst, A.; Hirschfelder, U. Pilot study on accuracy and dimensional stability of impression materials using industrial CT technology. J. Orofac. Orthop. 2011, 72, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef]
- Menditto, A.; Patriarca, M.; Magnusson, B. Understanding the meaning of accuracy, trueness and precision. Accredit. Qual. Assur. 2007, 12, 45–47. [Google Scholar] [CrossRef]
- Kim, J.E.; Amelya, A.; Shin, Y.; Shim, J.S. Accuracy of intraoral digital impressions using an artificial landmark. J. Prosthet. Dent. 2017, 117, 755–761. [Google Scholar] [CrossRef]
- Park, H.N.; Lim, Y.J.; Yi, W.J.; Han, J.S.; Lee, S.P. A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. J. Adv. Prosthodont. 2018, 10, 58–64. [Google Scholar] [CrossRef]
- Boeddinghaus, M.; Breloer, E.S.; Rehmann, P.; Wöstmann, B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin. Oral Investig. 2015, 19, 2027–2034. [Google Scholar] [CrossRef]
- Uhm, S.H.; Kim, J.H.; Jiang, H.B.; Woo, C.W.; Chang, M.; Kim, K.N.; Bae, J.M.; Oh, S. Evaluation of the accuracy and precision of four intraoral scanners with 70% reduced inlay and four-unit bridge models of international standard. Dent. Mater. J. 2017, 36, 27–34. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scan (min:s) | Design (min:s) | Milling (min:s) | Total (min:s) | |
|---|---|---|---|---|
| Mean | 07:16 | 06:50 | 16:51 | 30:58 |
| Maximum | 10:38 | 12:20 | 22:00 | 39:16 |
| Minimum | 04:03 | 04:28 | 11:38 | 24:33 |
| SD | 01:50 | 02:15 | 03:30 | 04:40 |
| Region | Method | Mean ± SD (Median) | 95% Confidence Interval (Range) | Normality | p Value |
|---|---|---|---|---|---|
| Marginal | CI | 107.86 ± 42.45 (109.13) | 82.21–133.51 (49.87–219.90) | 0.544 | 0.381 |
| IOS | 115.52 ± 38.22 (112.64) | 92.42–138.62 (27.08–244.32) | |||
| Axial | CI | 110.84 ± 33.43 (107.14) | 90.64–131.05 (67.07–276.76) | 0.057 | 0.582 |
| IOS | 113.05 ± 35.67 (102.98) | 91.50–134.61 (57.90–219.34) | |||
| Cusp | CI | 151.04 ± 52.58 (143.32) | 119.27–182.81 (71.37–294.22) | 0.452 | 0.577 |
| IOS | 146.38 ± 46.78 (139.83) | 118.11–174.65 (58.77–246.93) | |||
| Occlusal | CI | 198.92 ± 77.04 (190.66) | 152.37–245.48 (96.81–386.78) | 0.053 | 0.442 |
| IOS | 207.54 ± 60.42 (198.84) | 171.03–244.05 (101.82–344.20) |
| Region | Marginal | Axial | Cusp | Occlusal |
|---|---|---|---|---|
| Marginal | CI IOS | p = 0.800 p = 0.278 | p < 0.001 p < 0.001 | p < 0.001 p < 0.001 |
| Axial | p = 0.800 p = 0.278 | CI IOS | p < 0.001 p < 0.001 | p < 0.001 p < 0.001 |
| Cusp | p < 0.001 p < 0.001 | p < 0.001 p < 0.001 | CI IOS | p < 0.001 p < 0.001 |
| Occlusal | p < 0.001 p < 0.001 | p < 0.001 p < 0.001 | p < 0.001 p < 0.001 | CI IOS |
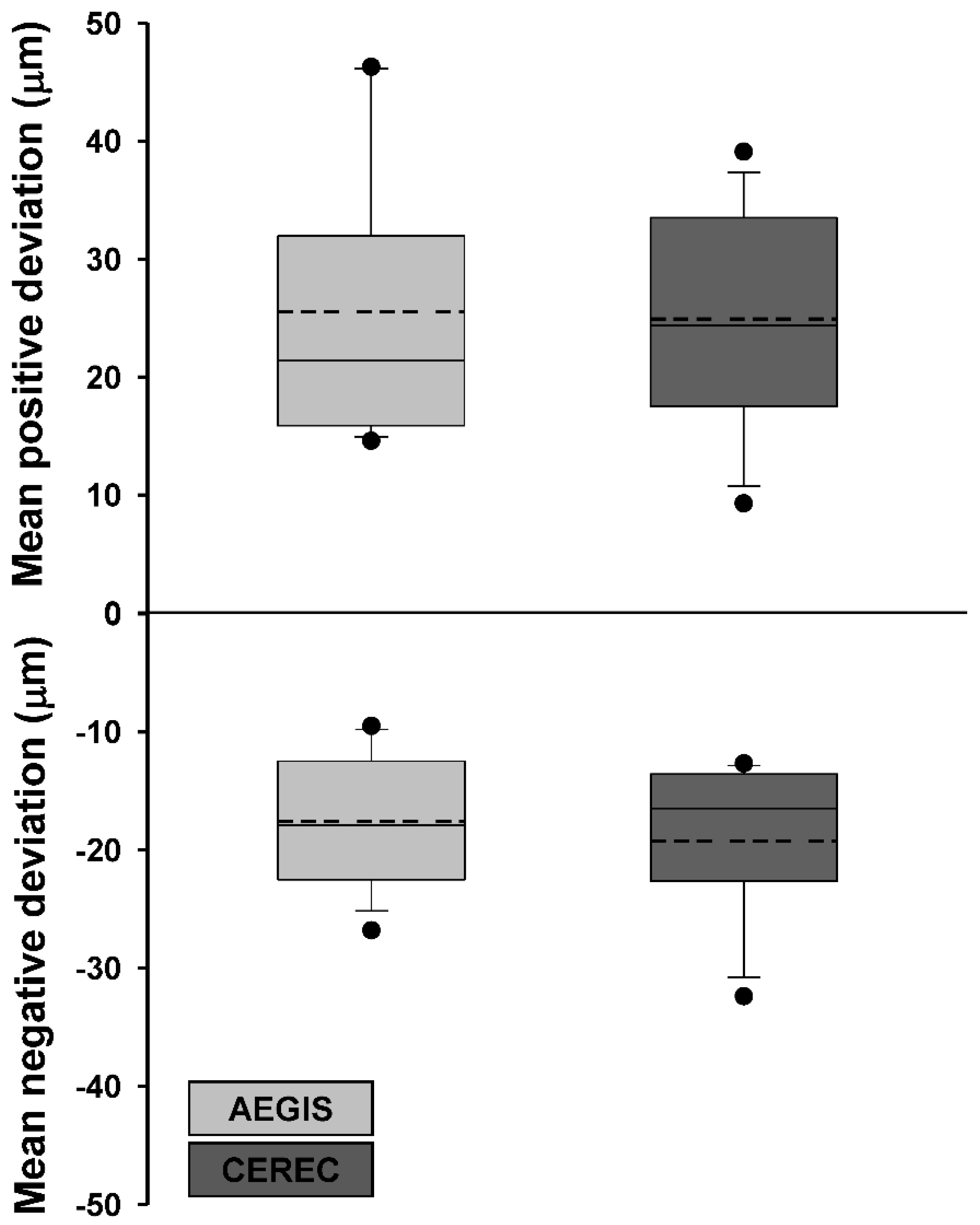
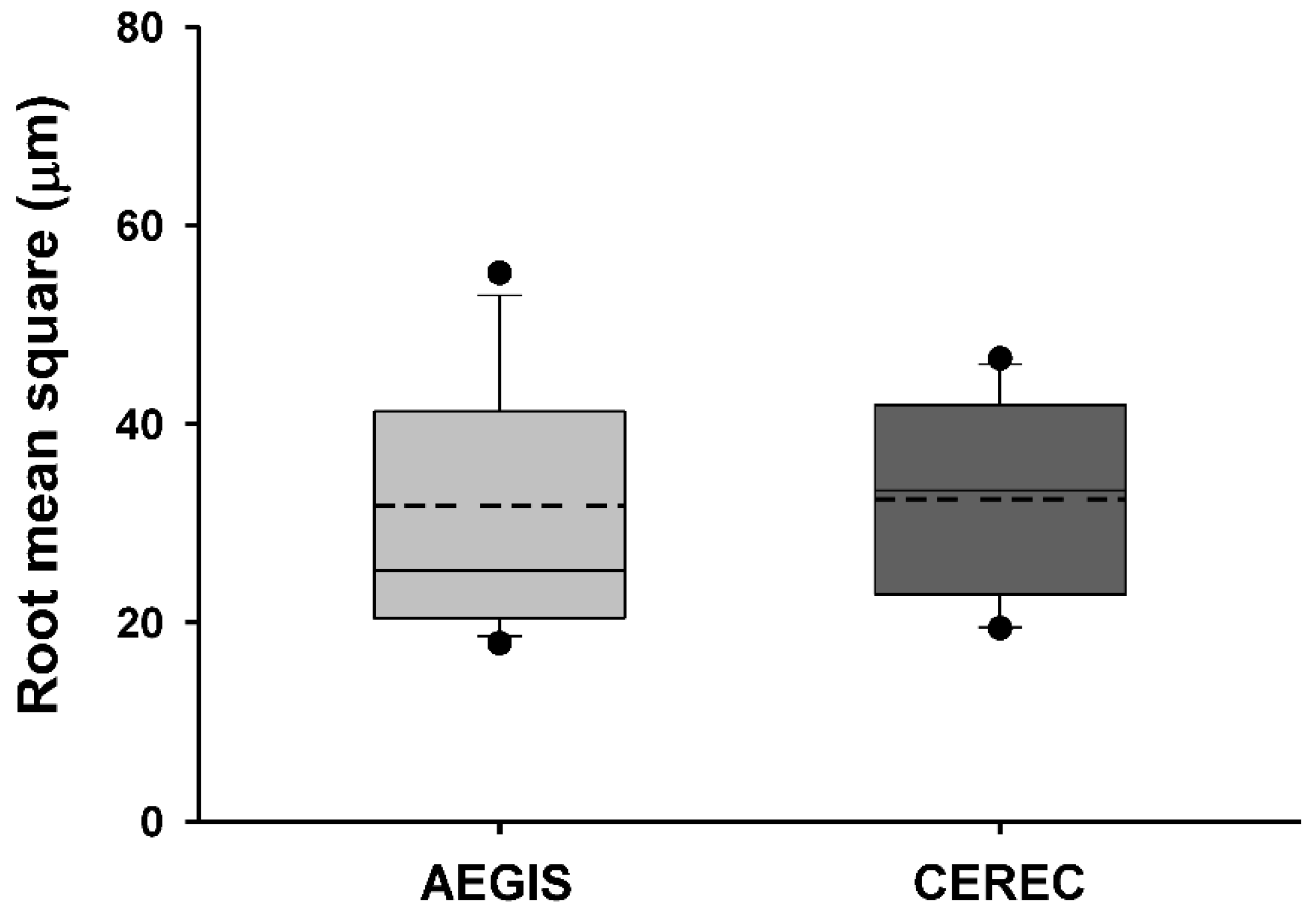
| Group | AEGIS | CEREC | Normality | p Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Mean positive deviation | 25.5 ± 11.0 | 24.9 ± 9.2 | 0.774 | 0.738 |
| Mean negative deviation | −17.6 ± 5.4 | −19.2 ± 6.2 | 0.262 | 0.409 |
| Root mean square | 31.7 ± 12.3 | 32.4 ± 9.7 | 0.894 | 0.760 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-S.; Lim, Y.-J.; Kim, B.; Kim, M.-J.; Kwon, H.-B. Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression. Materials 2020, 13, 5467. https://doi.org/10.3390/ma13235467
Park J-S, Lim Y-J, Kim B, Kim M-J, Kwon H-B. Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression. Materials. 2020; 13(23):5467. https://doi.org/10.3390/ma13235467
Chicago/Turabian StylePark, Ji-Su, Young-Jun Lim, Bongju Kim, Myung-Joo Kim, and Ho-Beom Kwon. 2020. "Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression" Materials 13, no. 23: 5467. https://doi.org/10.3390/ma13235467
APA StylePark, J.-S., Lim, Y.-J., Kim, B., Kim, M.-J., & Kwon, H.-B. (2020). Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression. Materials, 13(23), 5467. https://doi.org/10.3390/ma13235467