1. Introduction
Self-healing concrete is used to prevent concrete deterioration and improve durability [
1,
2,
3]. Since there are insufficient human and material resources for damage detection and the timely repair of concrete components, scholars proposed a self-healing concrete with bionic characteristics. Microcapsule self-healing composites, a research hot spot in the field of self-healing, have received increasing attention for use in cement-based materials [
4,
5,
6,
7].
Since White et al. [
8] first developed concrete microcapsules with a self-healing ability using injection techniques and polymerization, scholars have conducted numerous studies on microcapsule self-healing concrete using different methods [
9,
10,
11,
12,
13]. In recent years, researchers focused on the performance and technology of microencapsulated self-healing concrete. Jose [
14] introduced calcium nitrate as a self-healing material to improve the microencapsulation process and the mechanical properties of the microencapsulated concrete. The mix proportion of the concrete was determined by experiments, and the self-healing efficiency of the self-healing concrete was evaluated. Perez [
15] innovatively used nano-silica and amine-based materials with good cement compatibility as wall and core materials of microcapsules, respectively, to form a relatively stable concrete self-healing system. Wang et al. [
16] used bentonite and an expansive agent as core materials and swelling resin as a wall material. The permeability was evaluated to determine the optimal process and the optimal components of the microcapsules. In addition, the effects of the crack width and microcapsule dosage on the repair performance were investigated. Zhu et al. [
17] used basalt fiber/cement as the self-healing material and determined the optimum mix proportion of the composite material using the ultrasonic time, amplitude, and frequency as indices. Giannaros et al. [
18] studied the repair performance of self-healing mortar specimens with different contents of the microcapsules and curing agent. Zhang et al. [
19] used the mercury intrusion and nitrogen adsorption methods combined with micro-computed tomography (μ-CT) to characterize the pore structure of the microencapsulated cement-based materials containing epoxy resin. It was found that the pore structure was significantly improved after healing. The above studies demonstrated the effectiveness of the performance recovery of self-healing concrete with microcapsules and focused on the appropriate dosage of the microcapsules, laying a foundation for subsequent large-scale experimental applications.
Other studies focused on the diversity of healing conditions and mechanisms of self-healing concrete with microcapsules. Sun et al. [
20] prepared melamine urea formaldehyde (MUF) microcapsules by in situ polymerization and studied the self-healing performance of asphalt concrete pavement. Kosarli et al. [
21] synthesized cement-based self-healing microcapsules with epoxy resin as the core material, analyzed the self-healing process of the microcapsules in the concrete using the capillary dynamics principle, and established a new self-healing evaluation method using the seepage structure parameters, pore structure parameters, and adsorption–desorption curve as indices. Lv et al. [
22] focused on the healing performance of self-healing concrete with epoxy resin microcapsules under a chloride and strong acid attack. Wang et al. [
23] combined microcapsule self-healing and microbial self-healing. The microcapsules protected the bacteria producing calcium carbonate, thus filling the cracks. Leeys et al. [
24] used polyvinyl alcohol (PVA) fibers and precipitation crystallization for self-healing. The PVA self-healing fibers were wrapped around the precipitation crystallization material, resulting in a good self-healing effect. Hong et al. [
25] established a new test system for self-healing concrete to evaluate damage and cracking. X-ray μ-CT was used to analyze the healing mechanism of two types of microcapsule self-healing systems. Both systems provided a good crack healing performance in concrete. The reviewed studies combined different principles to explore the healing mechanism of microencapsulated self-healing concrete in different environments. Thus, different working conditions and various evaluation indicators should be used to evaluate the self-healing performance comprehensively and objectively.
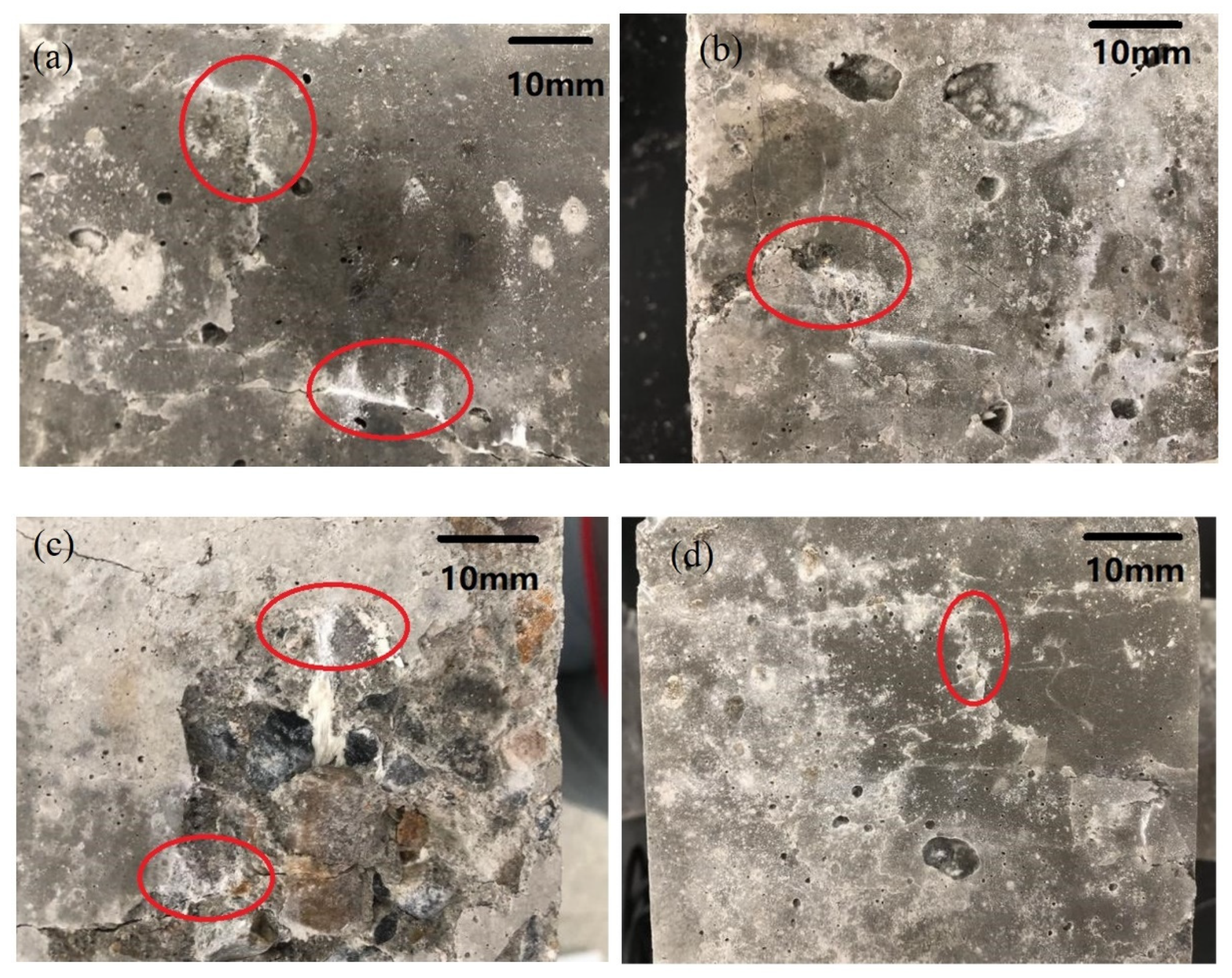
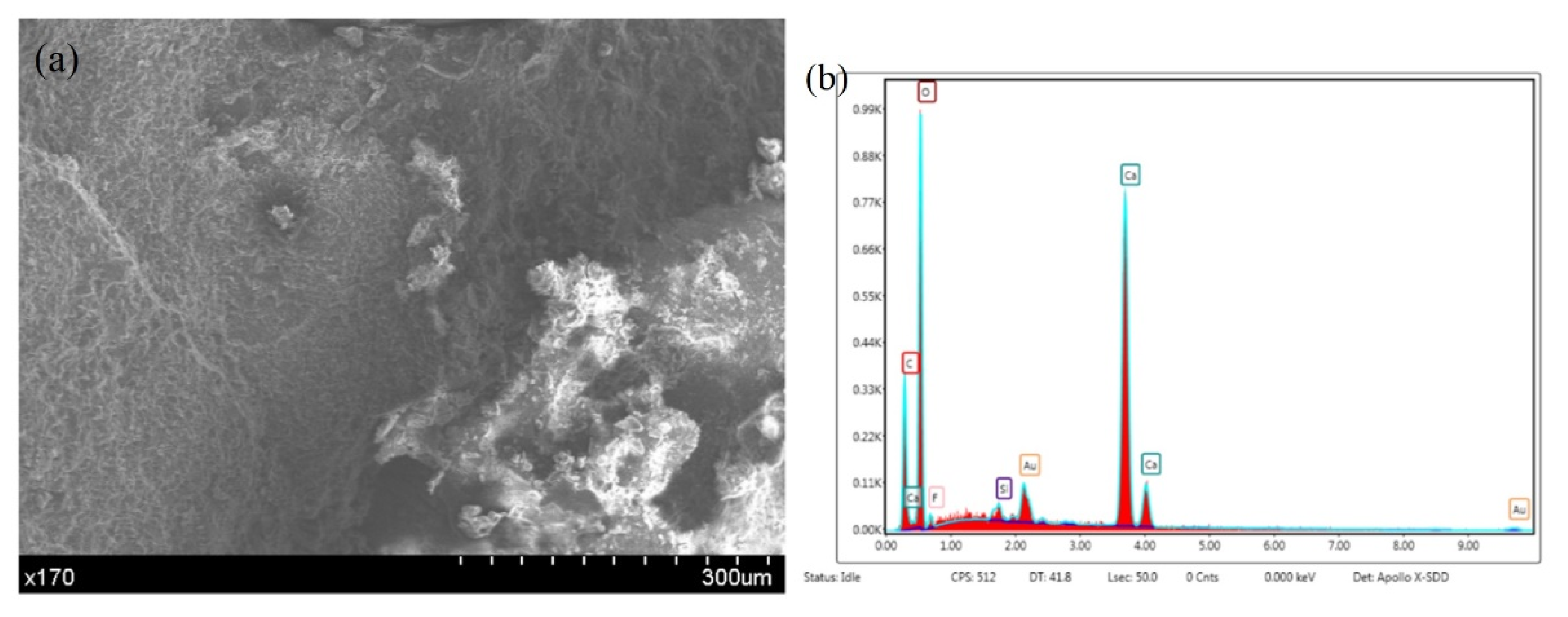
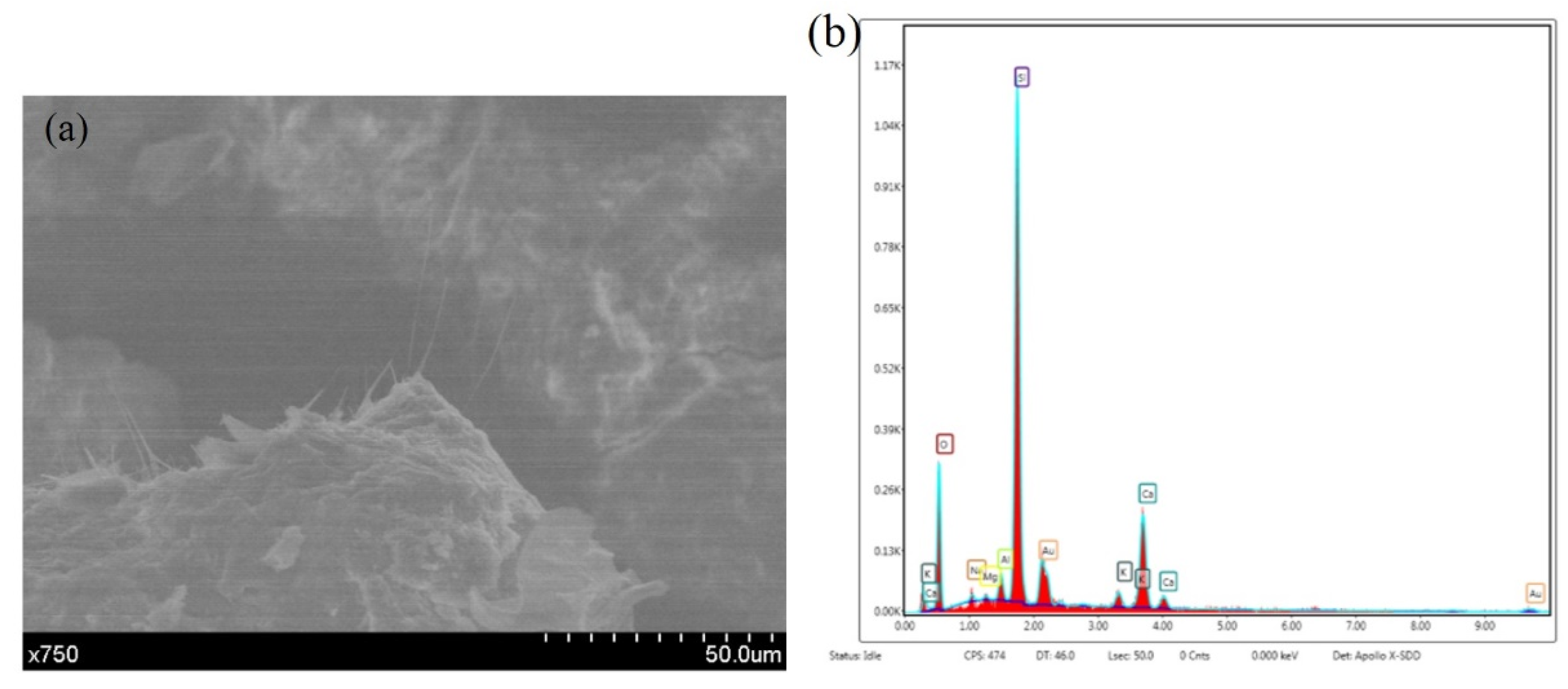
However, the amounts of the components in the microcapsule self-healing system and the components’ influences on the basic properties and self-healing properties of concrete remain unclear. In this paper, a microcapsule system is used in cement-based composites, and an orthogonal test is used to analyze the healing performance for different pre-damage loads. The strength recovery performance and sound speed recovery performance under extensive damage are analyzed using an orthogonal test. The optimum factor combination of the microcapsule self-healing cementitious composite system is obtained. Scanning electron microscopy (SEM) and energy dispersive spectroscopy (EDS) are conducted on the concrete samples before and after healing to determine the healing mechanism of the microcapsule self-healing concrete.
2. Specimen Preparation
A Wj-3 extrusion spheronizer (Panfeng Drying Equipment Co., Ltd, Changzhou, China) was used to prepare the microcapsules. The main steps included preparation of the wet material, extruding the strips, rolling the balls, spray coating, and hot-air drying. The first three steps focused on forming the pellets, and spray coating was used to combine the core and the wall. An appropriate coating solution was used. Due to the relatively high viscosity of the ethyl cellulose solution used in the capsule wall, the dissolving agent has volatile components. Thus, that material is prone to thermosetting, and hot-air drying was needed to prevent mutual adhesion. The preparation of the wet material was the first step and determined the composition of the repair material in the core material. Portland cement and sodium silicate, which react with calcium hydroxide, were added to the self-healing microcapsules, representing the core materials. This composition facilitates the comparison with subsequent experiments.
Concrete specimens (100 mm × 100 mm × 100 mm cubes) were prepared. The fixed water binder ratio was 0.54, the fineness modulus of the sand was 3.0–2.3, and the particle size of the gravel was about 3–5 mm. The cement properties are listed in
Table 1 and
Table 2. The microcapsules and other concrete materials were mixed in a concrete mixer. The finished cube specimen is shown in
Figure 1.
4. Influencing Factors on Compressive Strength
The ultimate compressive strength of the orthogonal test and ordinary concrete specimens is listed in
Table 4.
Table 5 and
Table 6 list the analysis of variance results of the ultimate compressive strength of the cube specimens. The results in
Table 5 and
Table 6 show that the compressive strength of the test specimens is optimal at 5% microcapsule content, 50% sodium silicate concentration, and 10% sodium fluosilicate content, and the combination level is A3B2C1. The
F-value of the compressive strength shows that the order of influence of the factors in the test is C > B > A. The most important factor affecting the compressive strength of the specimens is the percentage of sodium fluosilicate, followed by the proportion of microcapsules and the microcapsule content. The three factors can have a significant impact on the compressive strength of the concrete. The confidence level of the lowest influencing factor (microcapsule dosage) on the compressive strength of concrete is 60%. The
F-value of the proportion of sodium fluorosilicate is significantly higher than that of the other two factors, and the confidence level exceeds 95%.
The order of influence of the factors on the compressive strength at 28 d is B > C > A, and the influence of factor B is similar to that of factor C. Compared with the concrete aged for 7 d, factor A has a lower F-value and B has a higher F-value for the concrete cured for 28 d, indicating that the strength of the microcapsules may have a larger influence on the concrete aged for 28 d. In addition, the significant decrease in the F-value of factor C is due to the retarding effect of sodium fluosilicate. An increase in its dosage results in a more pronounced retarding effect for the concrete cured for 7 d and a decrease in the retarding effect for the concrete cured for 28 d.
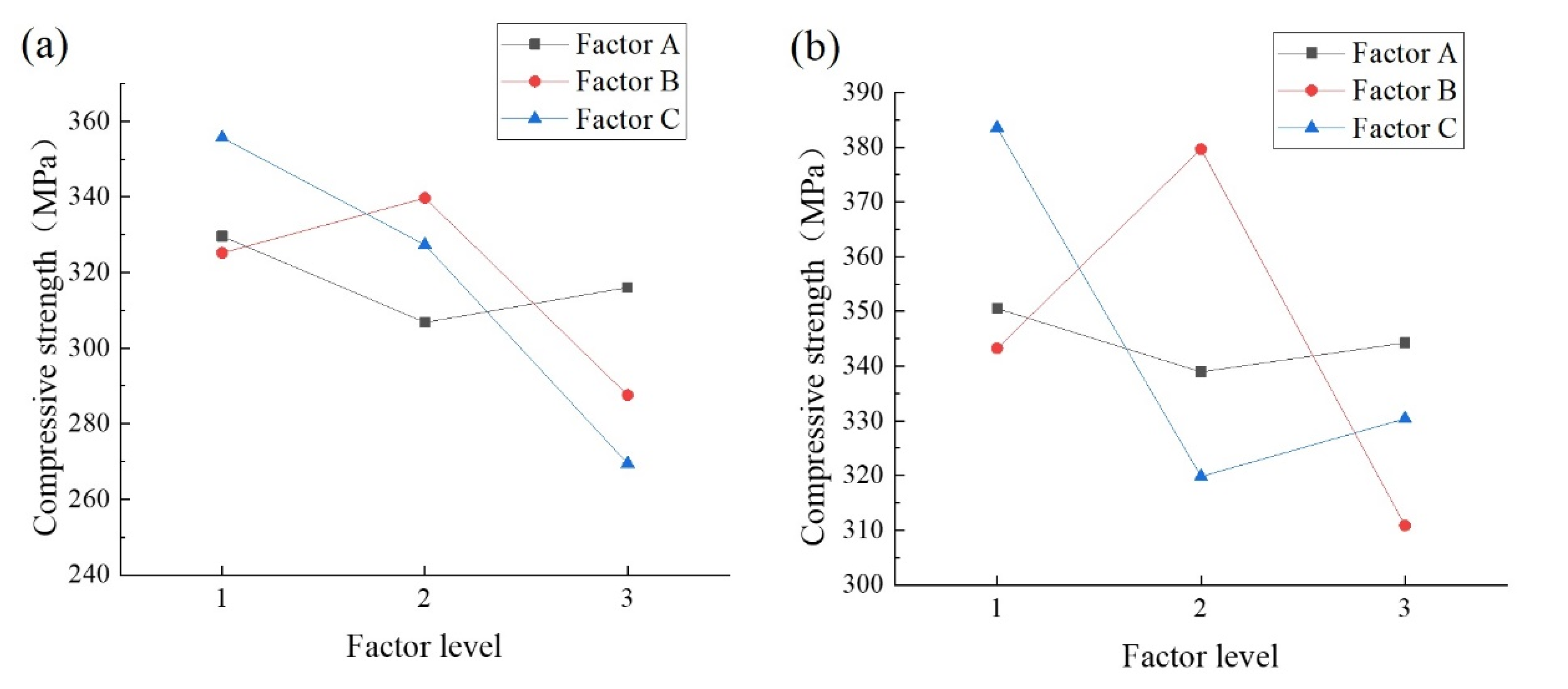
A comparison of the
K-values in
Figure 2 indicates that for factor A, the strength is the highest at a microcapsule content of 1%, indicating that an increase in the microcapsule content reduces the concrete strength, but the strength reduction is not significant at contents of 3% and 5%. For factor B, the concrete strength is the highest at 50% sodium silicate. For factor C, the compressive strength of concrete decreases with the sodium fluosilicate content, which is consistent with the conclusion that a high content of sodium fluosilicate reduces the compressive strength of concrete.
5. Influencing Factors on the Recovery Rate of the Compressive Strength
5.1. Variance Analysis of Influencing Factors on Strength Recovery
The recovery rate of the compressive strength according to the ultimate compressive strength of the cube specimens before and after healing is listed in
Table 7 and
Table 8. The strength recovery rates of the nine experimental groups are higher than that of the control group, demonstrating the effectiveness of the microcapsule self-healing concrete system.
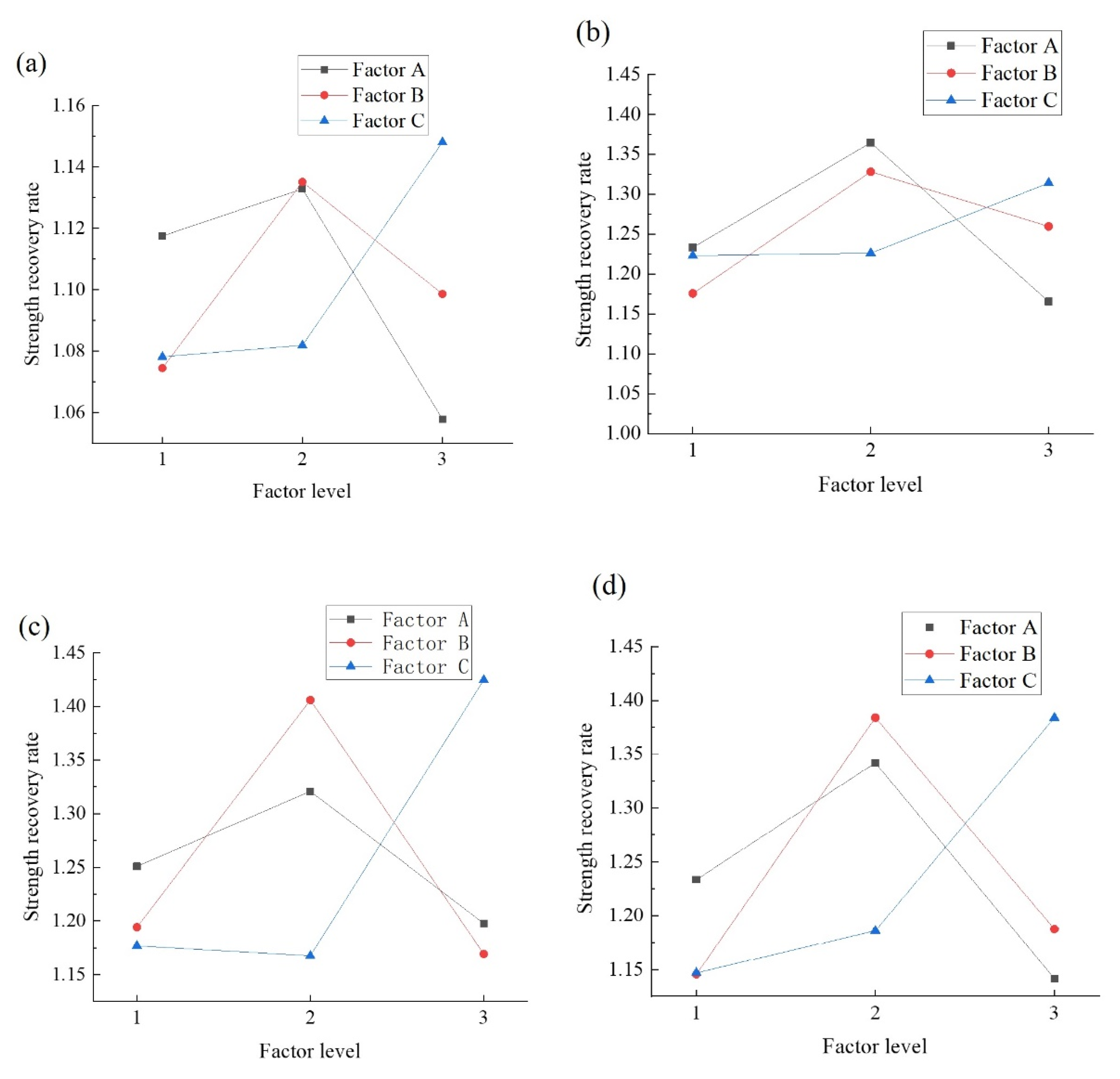
The
K-values (
Figure 3) indicate that the maximum recovery rate is obtained after 7 d of curing, and the maximum healing rate of the specimens with 100% and 90% damage loads at 28 d is obtained at 3% dosage. In the 80% and 70% damage conditions, the recovery rate decreases with an increase in the dosage. The healing ability of the microcapsules is poor due to the insufficient microcapsule content at 1% dosage. However, at 5% dosage, the damage to the concrete is greater, indicating that the self-healing performance is impaired in pre-damaged specimens. The self-healing performance is lower at a microcapsule content of 5% than 3% at 80% and 70% damage loads at 28 d of curing. The reason may be that there are fewer cracks under a low damage load, especially for concrete aged for 28 d. Therefore, there are fewer microcapsules with crack damage. As a result, the healing rate is reduced. Besides, factor A has a negligible influence on the compressive strength, whereas the 100% and 90% damage loads are the primary factors influencing the healing rate for the two curing conditions. Therefore, the optimal factor level of factor A in the system is 3%.
The K-value indicates that a 50% sodium silicate content is the optimum factor level for the microcapsule self-healing concrete. Although Portland cement provides strength recovery, it is insufficient, leading to a decrease in the self-healing performance. The strength of the microcapsules with a 70% sodium silicate content is relatively low; thus, there are more cracks. In this case, sodium silicate acts as a binder but cannot fill the cracks. Therefore, the strength recovery performance of the self-healing microcapsules consisting entirely of sodium silicate was relatively low. In addition, the concentration of the core had a substantial influence on the compressive strength and recovery rate at 7 d but a negligible effect at 28 d (the F-value was about 1) and was low at a concentration of 70%. Therefore, the optimum factor level of the sodium silicate content is 50%.
The influence of factor C (sodium fluosilicate content) on the recovery rate depends on the curing time. At 7 d of curing, the recovery rate increases with an increase in the sodium fluosilicate content due to its retarding, resulting in a substantial reduction in the concrete strength aged for 7 d and an increase in the recovery rate in the later period. At aging for 28 d, the optimum factor level of C2 is 15%. The reason is the same as for factor B, i.e., the healing effect at a low dosage cannot compensate for the cracks, but the damage is similar at a high dosage.
5.2. Influence of Damage Loads on the Significance of Various Factors
The
F-values of the compressive strength recovery rate after healing at aging for 7 d and 28 d are listed in
Table 9 and
Table 10. Unlike at pre-damage loads of 70% and 80%, at 100%, the most influential factor is the microcapsule content at 7 d and 28 d. The reasons are as follows. Under complete or almost complete failure, there are more cracks in the concrete and the microcapsules, and the self-healing efficiency largely depends on the number of damaged microcapsules. Therefore, the microcapsule content determines the number of broken microcapsules, i.e., the self-healing rate. Therefore, under a high damage load, a high
F-value is obtained and vice versa. This finding demonstrates the effectiveness of the self-healing performance of the microcapsule self-healing concrete system.
5.3. The Optimum Factor Combination to Optimize the Recovery Rate
The variance analysis shows that in most cases, the F-values of the factors are greater than 1, and the confidence level is greater than 50%, indicating that all three factors affect the self-healing efficiency of concrete. The influence of the sodium fluorosilicate content is higher under a lower damage load because there are fewer broken microcapsules, and the sodium silicate may dissolve in water. The more sodium fluorosilicate is added, the higher the reaction rate is, and the greater the strength recovery is.
The variance analysis and K-values of the compressive strength and compressive strength recovery rate indicate that the optimum factor combination in the microcapsule self-healing concrete system is A2B2C2, (a microcapsule content of 3%, a sodium silicate content of 30%, and a sodium fluorosilicate content of 15%). This combination provides the optimum self-healing effect of the concrete without reducing the concrete strength under different damage loads.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}