
Effect of Conventional Adhesive Application or Co-Curing Technique on Dentin Bond Strength


Abstract
:
1. Introduction
2. Materials and Methods
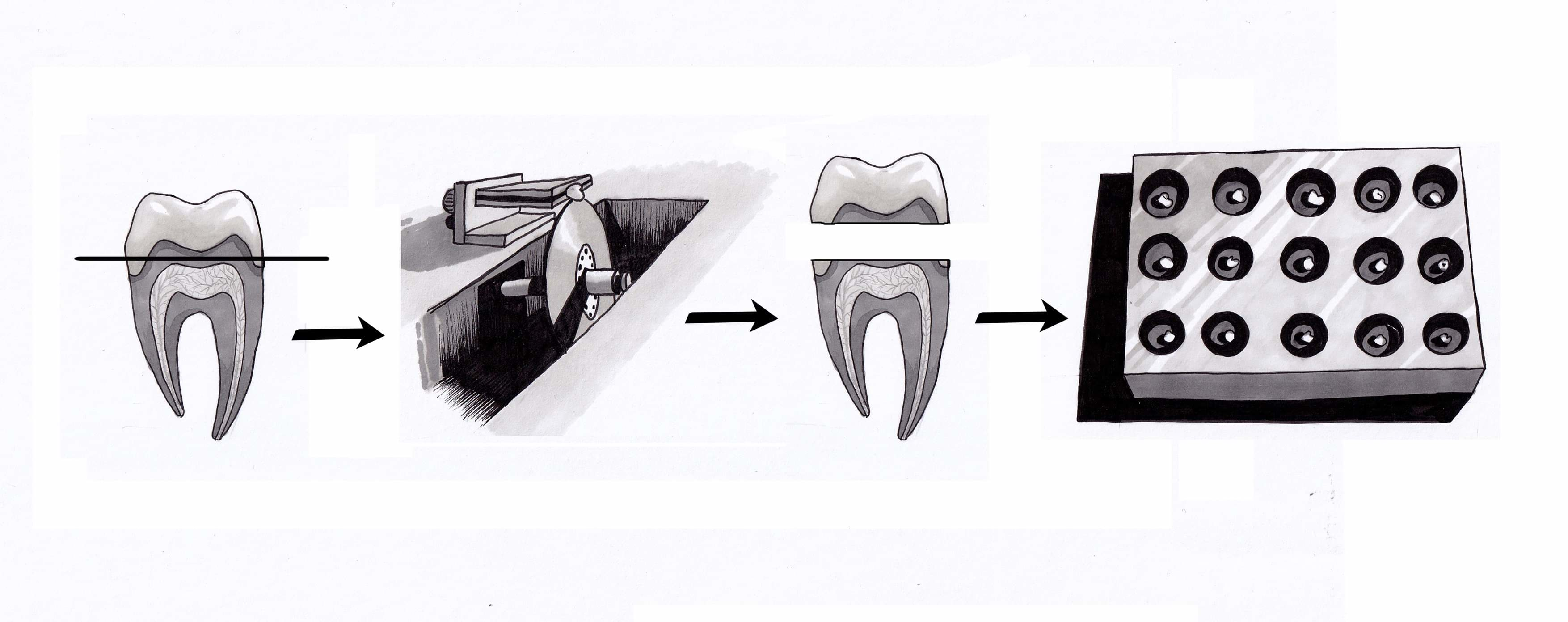
2.1. Dentin Substrate Preparation
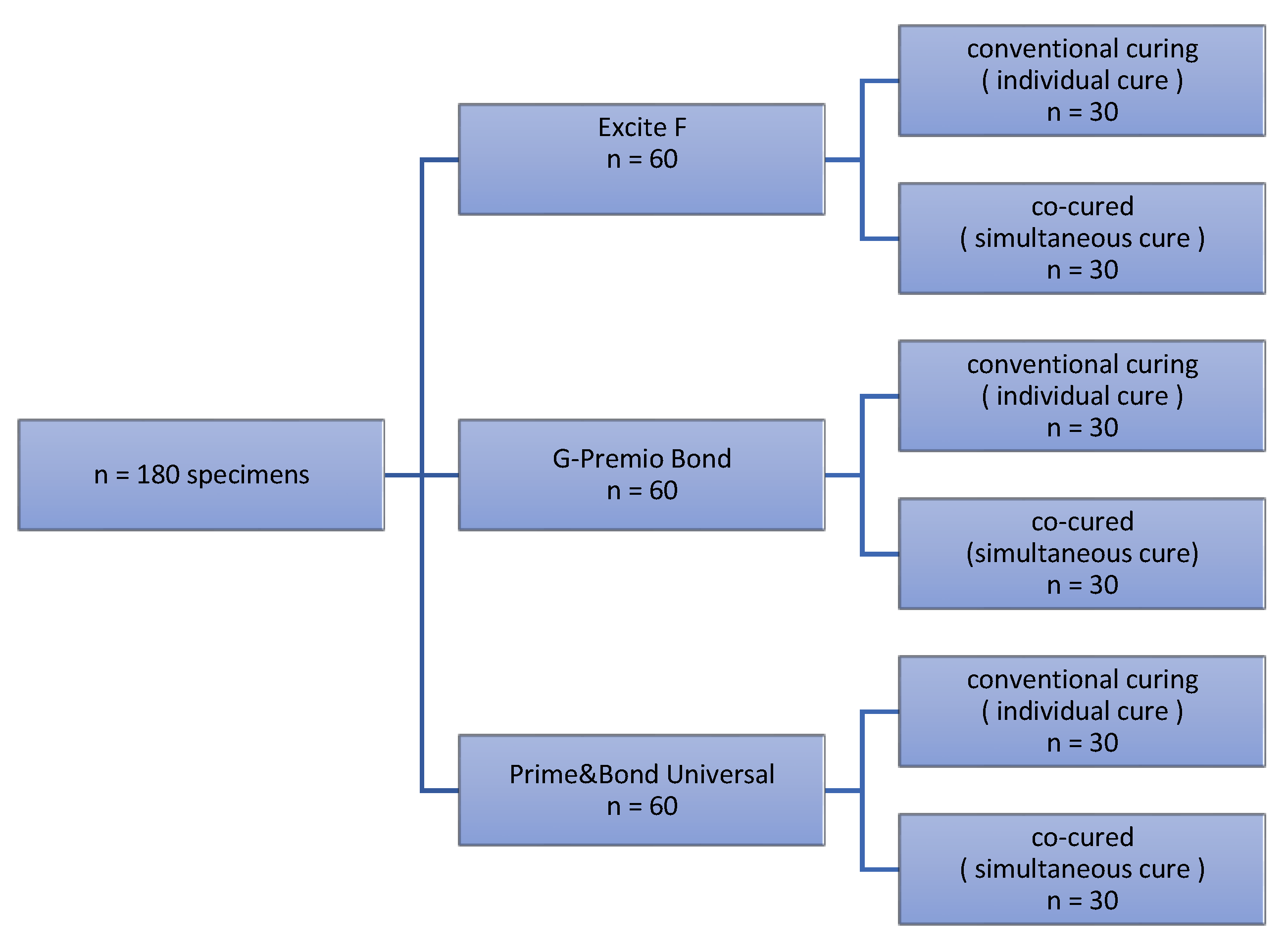
2.2. Bonding Procedure
2.3. Shear Bond Strength Testing
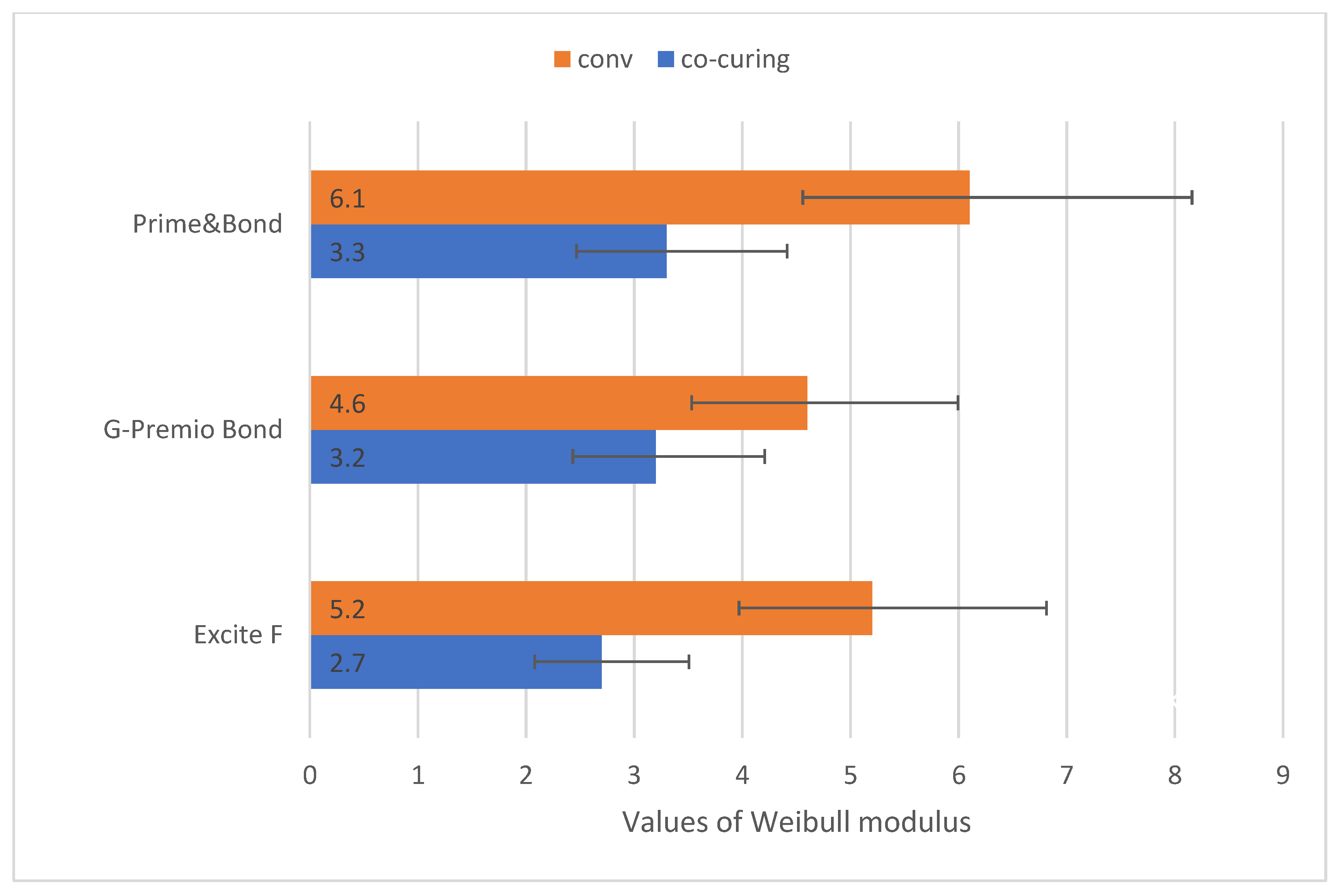
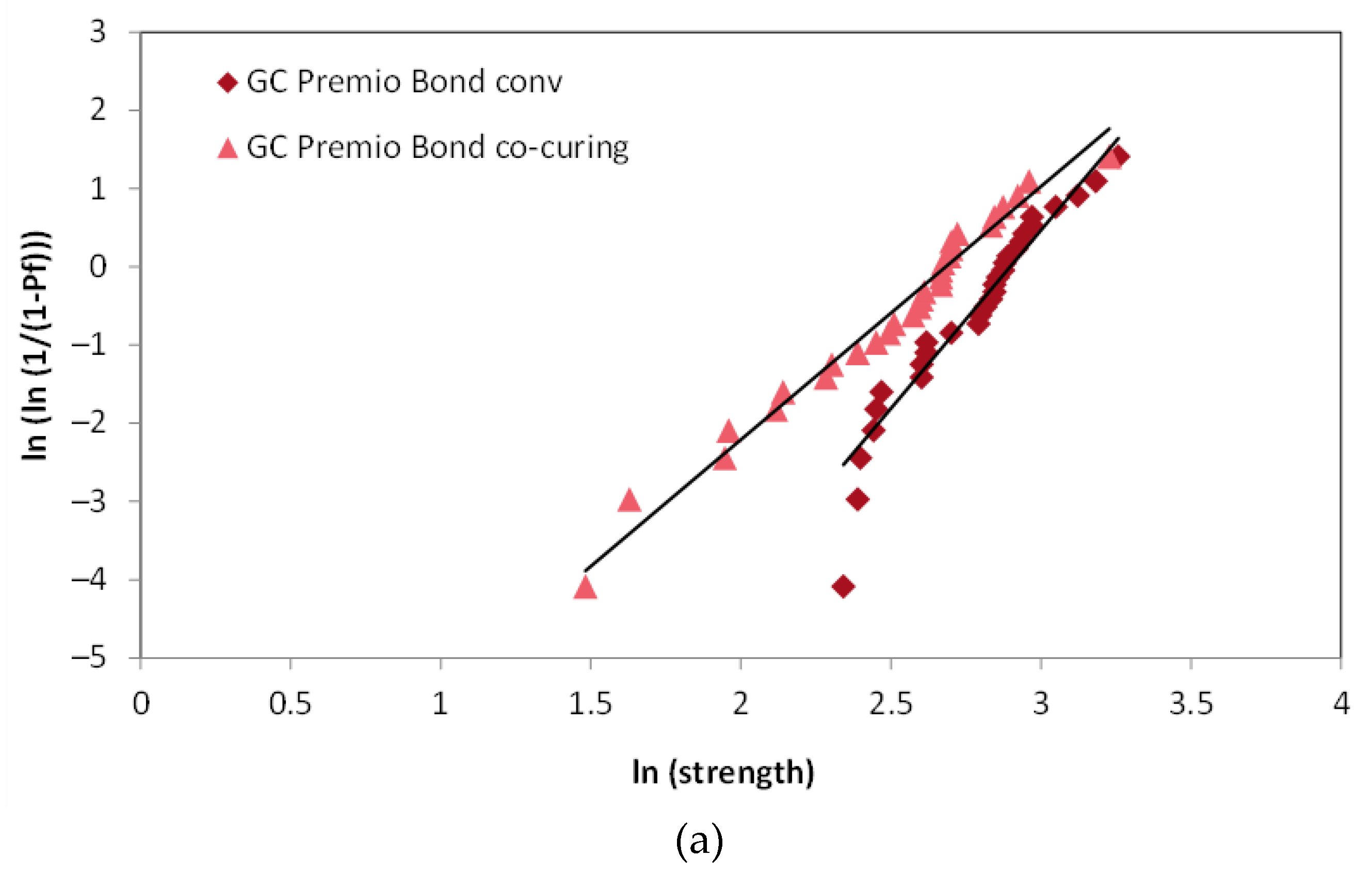
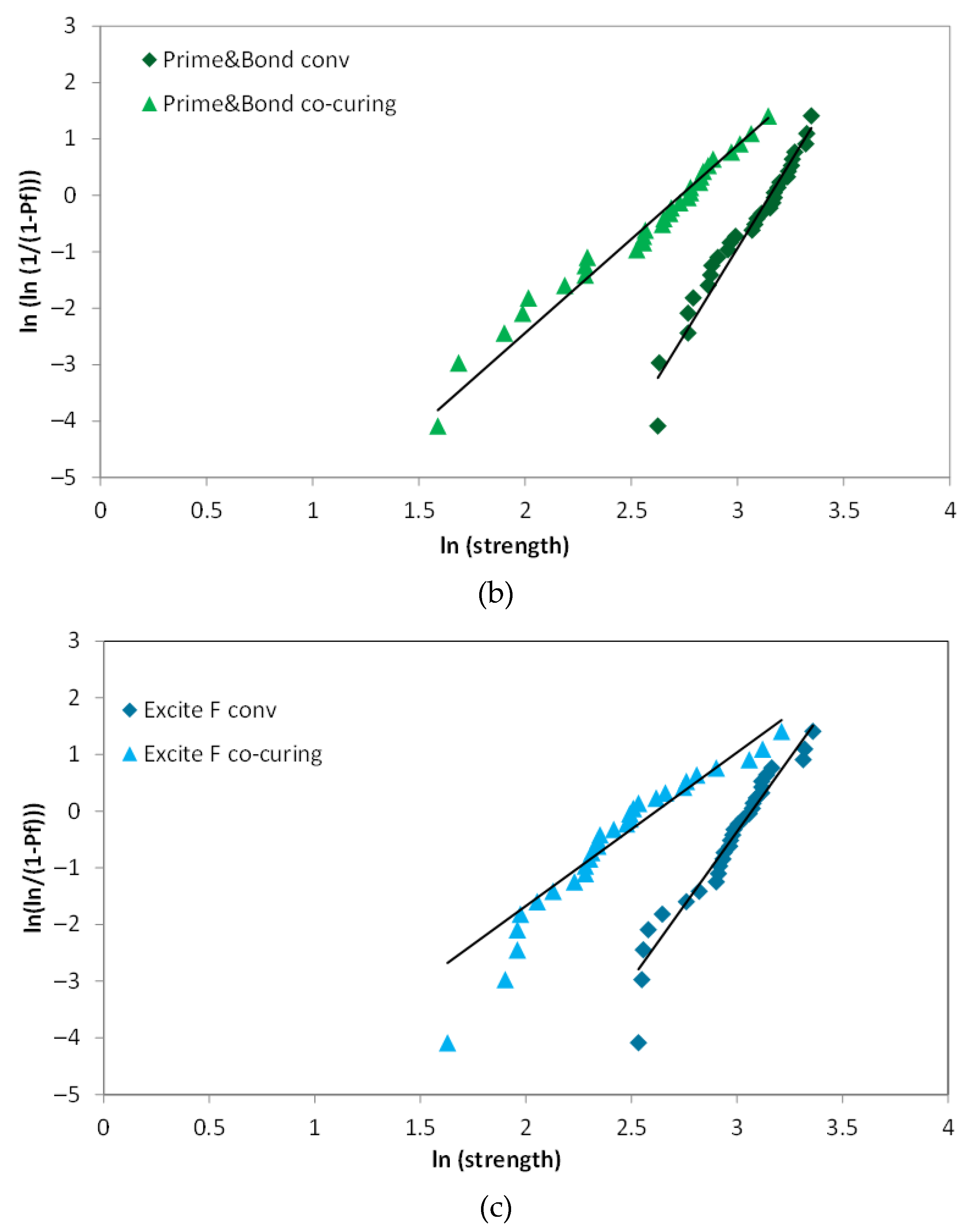
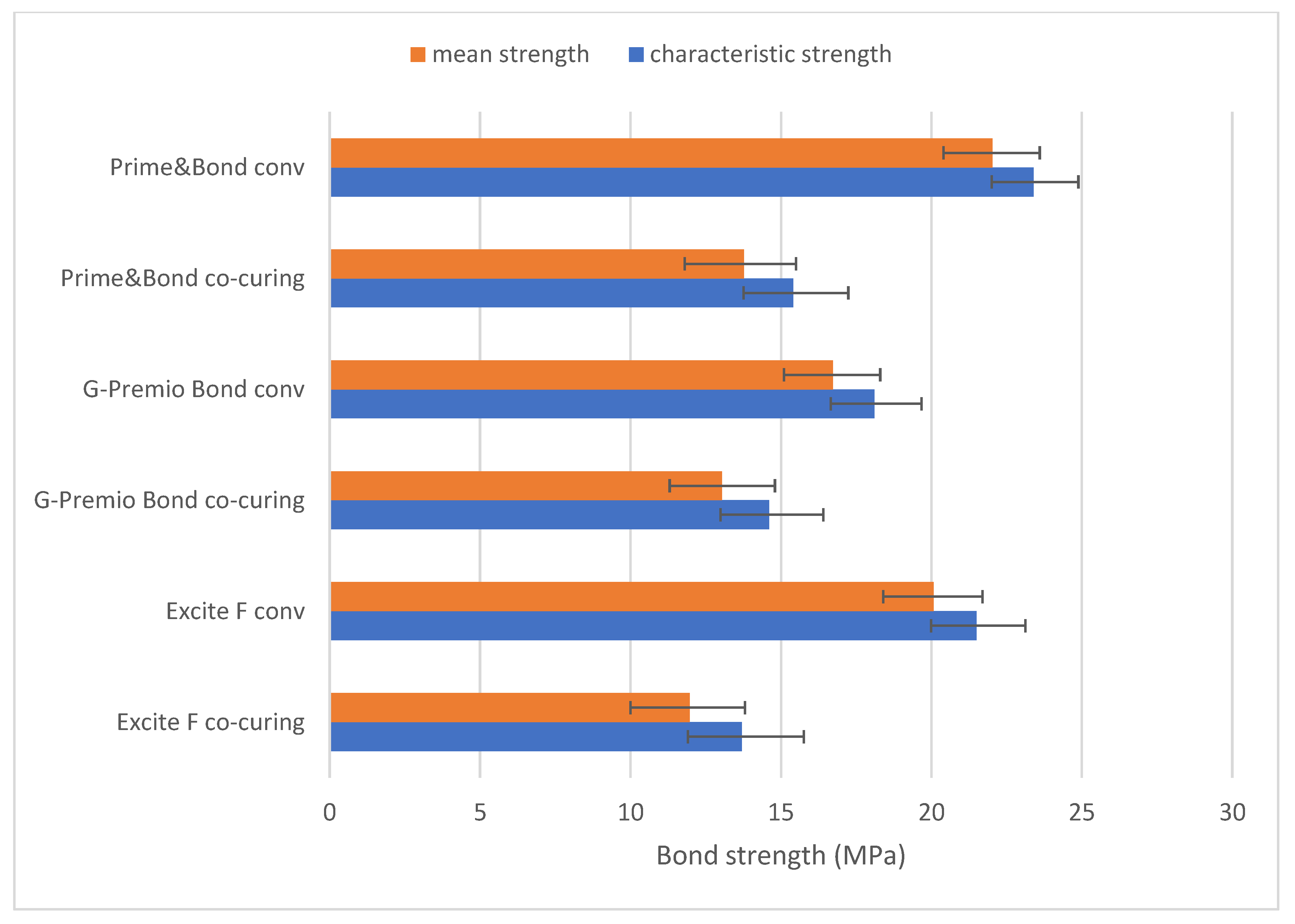
2.4. Weibull Analysis
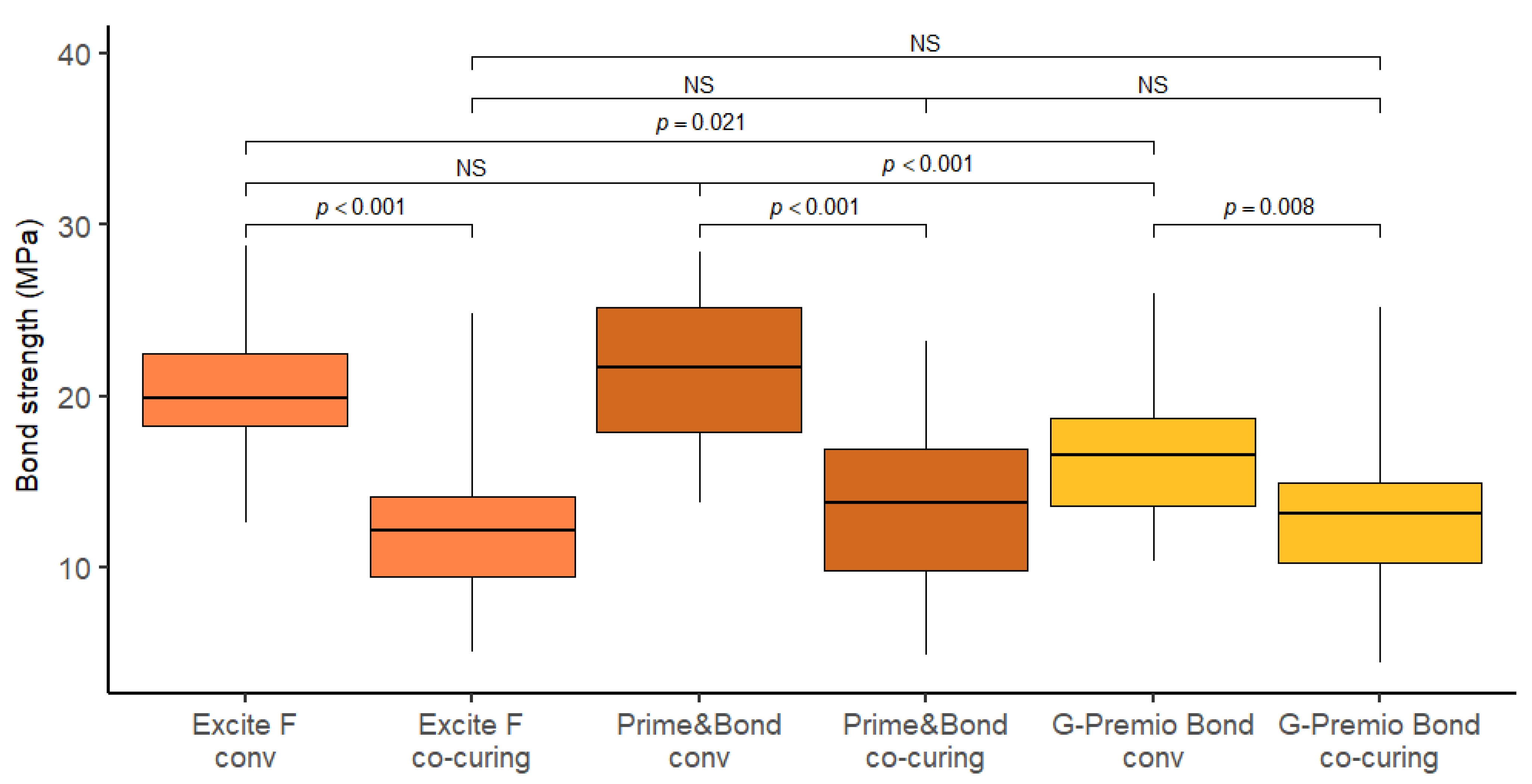
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sensi, L.G.; Marson, F.C.; Monteiro, S., Jr.; Baratieri, L.N. Caldeira de Andrada MA. Flowable composites as “filled adhesives:” A microleakage study. J. Contemp. Dent. Pract. 2004, 15, 32–41. [Google Scholar] [CrossRef]
- Kaisarly, D.; El Gezawi, M. Polymerization shrinkage assessment of dental resin composites: A literature review. Odontology 2016, 104, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.M.; Pereira, J.C.; Yoshiyama, M.; Pashley, D.H. A review of polymerisation contraction: The influence of stress development versus stress relief. Oper. Dent. 1996, 21, 17–24. [Google Scholar] [PubMed]
- Al-Yousifany, N.N. Effects of flowable composite resin and curing method on microleakage. Al–Rafidain Dent. J. 2010, 10, 1–7. [Google Scholar]
- Rosatto, C.M.; Bicalho, A.A.; Veríssimo, C.; Bragança, G.F.; Rodrigues, M.P.; Tantbirojn, D.; Versluis, A.; Soares, C.J. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J. Dent. 2015, 43, 1519–1528. [Google Scholar] [CrossRef]
- Braga, R.R.; Ballester, R.Y.; Ferracane, J.L. Factors involved in the development of polymerization shrinkage stress in resin-composites: A systematic review. Dent. Mater. 2005, 21, 962–970. [Google Scholar] [CrossRef]
- Kleverlaan, C.J.; Feilzer, A.J. Polymerization shrinkage and contraction stress of dental resin composites. Dent. Mater. 2005, 21, 1150–1157. [Google Scholar] [CrossRef]
- Miletic, V.; Pongprueksa, P.; De Munck, J.; Brooks, N.R.; Van Meerbeek, B. Curing characteristics of flowable and sculptable bulk-fill composites. Clin. Oral Investig. 2017, 21, 1201–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzante, F.A.P.; Duque, J.A.; Duarte, M.A.H.; Mondelli, R.F.L.; Mendonça, G.; Ishikiriama, S.K. Polymerization shrinkage, microhardness and depth of cure of bulk fill resin composites. Dent. Mater. J. 2019, 38, 403–410. [Google Scholar] [CrossRef] [Green Version]
- Al Sunbul, H.; Silikas, N.; Watts, D.C. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent. Mater. 2016, 32, 998–1006. [Google Scholar] [CrossRef] [Green Version]
- Unterbrink, G.L.; Müssner, R. Influence of light intensity on two restorative systems. J. Dent. 1995, 3, 183–189. [Google Scholar] [CrossRef]
- Ferracane, J.; Hilton, T.J. Polymerization stress—Is it clinically meaningful? Dent. Mater. 2016, 32, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Unterbrink, G.L.; Liebenberg, W.H. Flowable resin composites as “filled adhesives”: Literature review and clinical recommendations. Quintessence Int. 1999, 30, 249–257. [Google Scholar] [PubMed]
- Chapman, J.L.; Burgess, O.; Holst, S.; Sadan, A.; Biatz, M.B. Pre-curing of self-etching bonding agents and its effect on the bond strengths of the resin composite to the dentin and enamel. Quintessence Int. 2007, 38, 637–641. [Google Scholar]
- Viswanathan, R.; Shashibhushan, K.K.; Subba Reddy, V.V. Short communication: Pre- and co-curing effect of adhesives on shear bond strengths of composite resins to primary enamel and dentine: An in vitro study. Eur. Arch. Paediatr. Dent. 2011, 12, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Bucuta, S.; Ilie, N. Light transmittance and micro-mechanical properties of bulk fill vs. conventional resin based composites. Clin. Oral Investig. 2014, 18, 1991–2000. [Google Scholar] [CrossRef]
- Savadi Oskoee, S.; Bahari, M.; Jafari Navimipour, E.; Ajami, A.A.; Ghiasvand, N.; Savadi Oskoee, A. Factors affecting marginal integrity of class II bulk-fill composite resin restorations. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 101–109. [Google Scholar] [CrossRef]
- Farahat, F.; Daneshkazemi, A.R.; Hajiahmadi, Z. The effect of bulk depth and irradiation time on the surface hardness and degree of cure of bulk-fill composites. J. Dent. Biomater. 2016, 3, 284–291. [Google Scholar]
- Abdelaziz, K.M.; Saleh, A.A. Influence of adhesive-composite application modalities on their bonding to tooth structure and resistance of the performed restorations to failure. J. Dent. Sci. 2018, 13, 378–385. [Google Scholar] [CrossRef]
- Deliperi, S.; Bardwell, D.N.; Papathanasiou, A.; Kastali, S.; Garcia-Godoy, F. Microleakage of a microhybrid composite resin using three different adhesive placement techniques. J. Adhes. Dent. 2004, 6, 135–139. [Google Scholar]
- De Munck, J.; Van Landuyt, K.; Peumans, M.; Poitevin, A.; Lambrechts, P.; Braem, M.; Van Meerbeek, B. A critical review of the durability of adhesion to tooth tissue: Methods and results. J. Dent. Res. 2005, 84, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Sano, H.; Takatsu, T.; Ciucchi, B.; Horner, J.A.; Matthews, W.G.; Pashley, D.H. Nanoleakage: Leakage within the hybrid layer. Oper. Dent. 1995, 20, 18–25. [Google Scholar] [PubMed]
- Pashley, D.H.; Tay, F.R.; Breschi, L.; Tjäderhane, L.; Carvalho, R.M.; Carrilho, M.; Tezvergil-Mutluay, A. State of the art etch-and-rinse adhesives. Dent. Mater. 2011, 27, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alex, G. Universal adhesives: The next evolution in adhesive dentistry? Compend. Contin. Educ. Dent. 2015, 36, 15–26. [Google Scholar]
- Yoshihara, K.; Nagaoka, N.; Sonoda, A.; Maruo, Y.; Makita, Y.; Okihara, T.; Irie, M.; Yoshida, Y.; Van Meerbeek, B. Effectiveness and stability of silane coupling agent incorporated in ‘universal’ adhesives. Dent. Mater. 2016, 32, 1218–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makishi, P.; André, C.B.; Silva, J.L.; Bacelar-Sá, R.; Correr-Sobrinho, L.; Giannini, M. Effect of storage time on bond strength performance of multimode adhesives to indirect resin composite and lithium disilicate glass ceramic. Oper. Dent. 2016, 41, 541–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Meerbeek, B.; Yoshihara, K.; Van Landuyt, K.; Yoshida, Y.; Peumans, M. From Buonocore’s pioneering acid-etch technique to self-adhering restoratives. A status perspective of rapidly advancing dental adhesive technology. J. Adhes. Dent. 2020, 22, 7–34. [Google Scholar]
- Torres, C.P.; Balbo, P.; Gomes-Silva, J.M.; Ramos, R.P.; Palma-Dibb, R.G.; Borsatto, M.C. Effect of individual or simultaneous curing on sealant bond strength. J. Dent. Child. 2005, 72, 31–35. [Google Scholar]
- ISO 29022:2013. Dentistry—Adhesion—Notched-Edge Shear Bond Strength Test; European Standard: Geneva, Switzerland, 2013. [Google Scholar]
- Quinn, J.B.; Quinn, G.D. A practical and systematic review of Weibull statistics for reporting strengths of dental materials. Dent. Mater. 2010, 26, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Burke, F.J.; Hussain, A.; Nolan, L.; Fleming, G.J. Methods used in dentine bonding tests: An analysis of 102 investigations on bond strength. Eur. J. Prosthodont. Restor. Dent. 2008, 16, 158–165. [Google Scholar] [PubMed]
- De Munck, J.; Mine, A.; Poitevin, A.; Van Ende, A.; Cardoso, M.V.; Van Landuyt, K.L.; Peumans, M.; Van Meerbeek, B. Meta-analytical review of parameters involved in dentin bonding. J. Dent. Res. 2012, 91, 351–357. [Google Scholar] [CrossRef]
- Heintze, S.D. Clinical relevance of tests on bond strength, microleakage and marginal adaptation. Dent. Mater. 2013, 29, 59–84. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, J.N.; Schumacher, G.E.; Antonucci, J.M.; Skrtic, D. Adhesion of amorphous calcium phosphate composites bonded to dentin: A study in failure modality. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 90, 238–249. [Google Scholar] [CrossRef] [Green Version]
- Braga, R.R.; Meira, J.B.; Boaro, L.C.; Xavier, T.A. Adhesion to tooth structure: A critical review of “macro” test methods. Dent. Mater. 2010, 26, 38–49. [Google Scholar] [CrossRef]
- Pecora, N.; Yaman, P.; Dennison, J.; Herrero, A. Comparison of shear bond strength relative to two testing devices. J. Prosthet. Dent. 2002, 88, 511–515. [Google Scholar] [CrossRef]
- Van Meerbeek, B.; Peumans, M.; Poitevin, A.; Mine, A.; Van Ende, A.; Neves, A.; De Munck, J. Relationship Between Bond-Strength Tests and Clinical Outcomes. Dent. Mater. 2010, 26, 100–121. [Google Scholar] [CrossRef]
- ISO/TS 11405:2003. Dental Materials—Testing of Adhesion to Tooth Structure; European Standard: Geneva, Switzerland, 2003. [Google Scholar]
- Sirisha, K.; Rambabu, T.; Shankar, Y.R.; Ravikumar, P. Validity of bond strength tests: A critical review: Part I. J. Conserv. Dent. 2014, 17, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leloup, G.; D’Hoore, W.; Bouter, D.; Degrange, M.; Vreven, J. Meta-analytical review of factors involved in dentin adherence. J. Dent. Res. 2001, 80, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Pashley, E.L.; Tao, L.; Matthews, W.G.; Pashley, D.H. Bond strengths to superficial, intermediate and deep dentin in vivo with four dentin bonding systems. Dent. Mater. 1993, 9, 19–22. [Google Scholar] [CrossRef]
- Perdigao, J. Dentin bonding-variables related to the clinical situation and the substrate treatment. Dent. Mater. 2010, 26, 24–37. [Google Scholar] [CrossRef]
- McCabe, J.F.; Rusby, S. Dentine bonding—The effect of pre-curing the bonding resin. Br. Dent. J. 1994, 176, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Davidson, C.L. In vivo resin-dentin interdiffusion and tag formation with lateral branches of two adhesive systems. J. Prosthet. Dent. 1996, 76, 250–253. [Google Scholar] [CrossRef]
- Cadenaro, M.; Maravic, T.; Comba, A.; Mazzoni, A.; Fanfoni, L.; Hilton, T.; Ferracane, J.; Breschi, L. The role of polymerization in adhesive dentistry. Dent. Mater. 2019, 35, e1–e22. [Google Scholar] [CrossRef]
- Mahn, E. Clinical criteria for the successful curin gof composite materials. Rev. Clin. Periodoncia Implantol. Rehabil. Oral 2013, 6, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Sperling, L.H. Introduction to Physical Polymer Science, 4th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Tabassum, S.; Hameed, M.H.; Khan, F.R. Comparison of the Depth of Cure of Flowable Composites Polymerized at Variable Increment Thicknesses and Voltages: An In vitro Study. Contemp. Clin. Dent. 2019, 10, 220–225. [Google Scholar]
- Polydorou, O.; Manolakis, A.; Hellwing, E.; Hahn, P. Evaluation of the curing depth of two translucent composite materials using halogen and two LED curing units. Clin. Oral Investig. 2008, 12, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hickel, R. Investigations on a methacrylate-based flowable composite based on the SDR™ technology. Dent. Mater. 2011, 27, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Mansour, K.; Sada, A.; Sinan, H. Curing depth of bulk fill composite an in vitro study. Pak. Oral Dent. J. 2015, 35, 270–275. [Google Scholar]
- Van Ende, A.; De Munck, J.; Van Landuyt, K.L.; Poitevin, A.; Peumans, M.; Van Meerbeek, B. Bulk-filling of high C-factor posterior cavities: Effect on adhesion to cavity-bottom dentin. Dent. Mater. 2013, 29, 269–277. [Google Scholar] [CrossRef]
- Tarle, Z.; Attin, T.; Marovic, D.; Andermatt, L.; Ristic, M.; Taubock, T.T. Influence of irradiation time on subsurface degree of conversion and microhardness of high-viscosity bulk-fill resin composites. Clin. Oral Investig. 2015, 19, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Comba, A.; Scotti, N.; Maravić, T.; Mazzoni, A.; Carossa, M.; Breschi, L.; Cadenaro, M. Vickers Hardness and Shrinkage Stress Evaluation of Low and High Viscosity Bulk-Fill Resin Composite. Polymers 2020, 12, 1477. [Google Scholar] [CrossRef]
- Van Meerbeek, B.; Yoshihara, K.; Yoshida, Y.; Mine, A.; De Munck, J.; Van Landuyt, K.L. State of the art of self-etch adhesives. Dent. Mater. 2011, 27, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; Kanumilli, P.; De Munck, J.; Van Landuyt, K.; Lambrechts, P.; Van Meerbeek, B. Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dent. Mater. 2005, 21, 864–881. [Google Scholar] [CrossRef]
- Yoshida, Y.; Nagakane, K.; Fukuda, R.; Nakayama, Y.; Okazaki, M.; Shintani, H.; Inoue, S.; Tagawa, Y.; Suzuki, K.; De Munck, J.; et al. Comparative study on adhesive performance of functional monomers. J. Dent. Res. 2004, 83, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Abate, P.F.; Rodrigues, V.I.; Macchi, R.L. Evaporation of solvent in one-bottle adhesives. J. Dent. 2000, 28, 437–440. [Google Scholar] [CrossRef]
- Choi, A.-N.; Lee, J.-H.; Son, S.-A.; Jung, K.-H.; Kwon, Y.H.; Park, J.-K. Effect of dentin wetness on the bond strength of universal adhesives. Materials 2017, 10, 1224. [Google Scholar] [CrossRef] [Green Version]
- Pashley, D.H.; Carvalho, R.M.; Tay, F.R.; Agee, K.A.; Lee, K.W. Solvation of dried dentin matrix by water and other polar solvents. Am. J. Dent. 2002, 15, 97–102. [Google Scholar]
- Van Meerbeek, B.; Vargas, M.; Inoue, S.; Yoshida, Y.; Peumans, M.; Lambrechts, P.; Vanherle, G. Adhesives and cements to promote preservation dentistry. Oper. Dent. 2001, 26, 119–144. [Google Scholar]
- Heintze, S.; Rousson, V.; Mahn, E. Bond strength tests of dental adhesive systems and their correlation with clinical results—A meta-analysis. Dent. Mater. 2015, 31, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Burrow, M.F.; Thomas, D.; Swain, M.V.; Tyas, M.J. Analysis of tensile bond strength using Weibull statistics. Biomaterials 2004, 25, 5031–5035. [Google Scholar] [CrossRef]
- Lu, C.S.; Danzer, R.; Fischer, F.D. Fracture statistics of brittle materials: Weibull or normal distribution. Phys. Rev. E 2002, 65, 067102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradna, P.; Vrbova, R.; Dudek, M.; Roubickova, A.; Housova, D. Comparison of bonding performance of self-etching and etch-and-rinse adhesives on human dentin using reliability analysis. J. Adhes. Dent. 2008, 10, 423–429. [Google Scholar] [PubMed]
- Roos, M.; Schatz, C.; Stawarczyk, B. Two independent prospectively planned blinded Weibull statistical analyses of flexural strength data of zirconia materials. Materials 2016, 9, 512. [Google Scholar] [CrossRef] [Green Version]
- Luhrs, A.K.; Guhr, S.; Schilke, R.; Borchers, L.; Geurtsen, W.; Gunay, H. Shear bond strength of self-etch adhesives to enamel with additional phosphoric acid etching. Oper. Dent. 2008, 33, 155–162. [Google Scholar] [CrossRef]
- Placido, E.; Meira, J.B.; Lima, R.G.; Muench, A.; de Souza, R.M.; Ballester, R.Y. Shear versus micro-shear bond strength test: A finite element stress analysis. Dent. Mater. 2007, 23, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, S.S.; Cesar, P.F.; Swain, M.V. Direct comparison of the bond strength results of the different test methods: A critical literature review. Dent. Mater. 2010, 26, 78–93. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Type | Chemical Formulation * | pH | Manufacturerand LOT No. |
|---|---|---|---|---|
| Total Etch | Etchant | phosphoric acid (37 wt.% in water), thickening agent and colour pigments | Ivoclar Vivadent AG, Schaan, Liechtenstein LOT: Y39066 EXP: 2022-01 | |
| Excite F | Adhesive (total-etch) | HEMA, Bis-GMA, UDMA, Phosphonic acid acrylate, highly dispersed siliconedioxide, initiators, stabilizers and potassium fluoride in an ethanol solution, camphorquinone, trimethylbenzoyldiphenylphosphine oxide | 2.5 | Ivoclar Vivadent AG, Schaan, Liechtenstein LOT: Z020C1 EXP: 2023-11 |
| G-Premio Bond | Adhesive (universal) | 10-MDP, 4-MET, MDTP, methacrylic acid ester, silica, acetone, water, photoinitiators | 1.5 | GC Corp., Tokyo, Japan LOT: 1906132 EXP: 2021-06 |
| Prime&Bond Universal | Adhesive (universal) | Bi- and multifunctional acrylate, 10-MDP, PENTA, phosphoric acid modified acrylate resin stabilizer, isopropanol, camphorquinone /tertiary amine | >2.5 | Dentsply Sirona, Konstanz, Germany LOT: 2009000399 EXP: 2022-08 |
| SDR Plus Bulk Fill Flowable | Bulk fill flowable resin composite | Polymerizable dimethacrylate resins, polymerizable UDMA, barium boron fluoro–alumino-silicate glass, silicon dioxide, titanium dioxide, synthetic inorganic iron oxides, photoinitiators | Dentsply Sirona, Konstanz, Germany LOT: 00028647 EXP: 2022-08 |
| Excite F |
|
| |
| |
| |
| |
| G-Premio Bond |
|
| |
| |
| Prime&Bond Universal |
|
| |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vukelja, J.; Klarić Sever, E.; Sever, I.; Jukić Krmek, S.; Tarle, Z. Effect of Conventional Adhesive Application or Co-Curing Technique on Dentin Bond Strength. Materials 2021, 14, 7664. https://doi.org/10.3390/ma14247664
Vukelja J, Klarić Sever E, Sever I, Jukić Krmek S, Tarle Z. Effect of Conventional Adhesive Application or Co-Curing Technique on Dentin Bond Strength. Materials. 2021; 14(24):7664. https://doi.org/10.3390/ma14247664
Chicago/Turabian StyleVukelja, Josipa, Eva Klarić Sever, Ivan Sever, Silvana Jukić Krmek, and Zrinka Tarle. 2021. "Effect of Conventional Adhesive Application or Co-Curing Technique on Dentin Bond Strength" Materials 14, no. 24: 7664. https://doi.org/10.3390/ma14247664
APA StyleVukelja, J., Klarić Sever, E., Sever, I., Jukić Krmek, S., & Tarle, Z. (2021). Effect of Conventional Adhesive Application or Co-Curing Technique on Dentin Bond Strength. Materials, 14(24), 7664. https://doi.org/10.3390/ma14247664