
Evaluation of Incipient Enamel Caries at Smooth Tooth Surfaces Using SS-OCT
 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Visual Inspection
- Score 0:
- No caries or demineralization of enamel.
- Score 1:
- Shallow enamel demineralization. Enamel demineralization appears at the outer half of the enamel thickness.
- Score 2:
- Deep enamel demineralization. Enamel demineralization appears to penetrate into the inner half of the enamel.
- Score 3:
- Enamel demineralization with remineralization.
- Score 4:
- Enamel caries with cavitated surface.
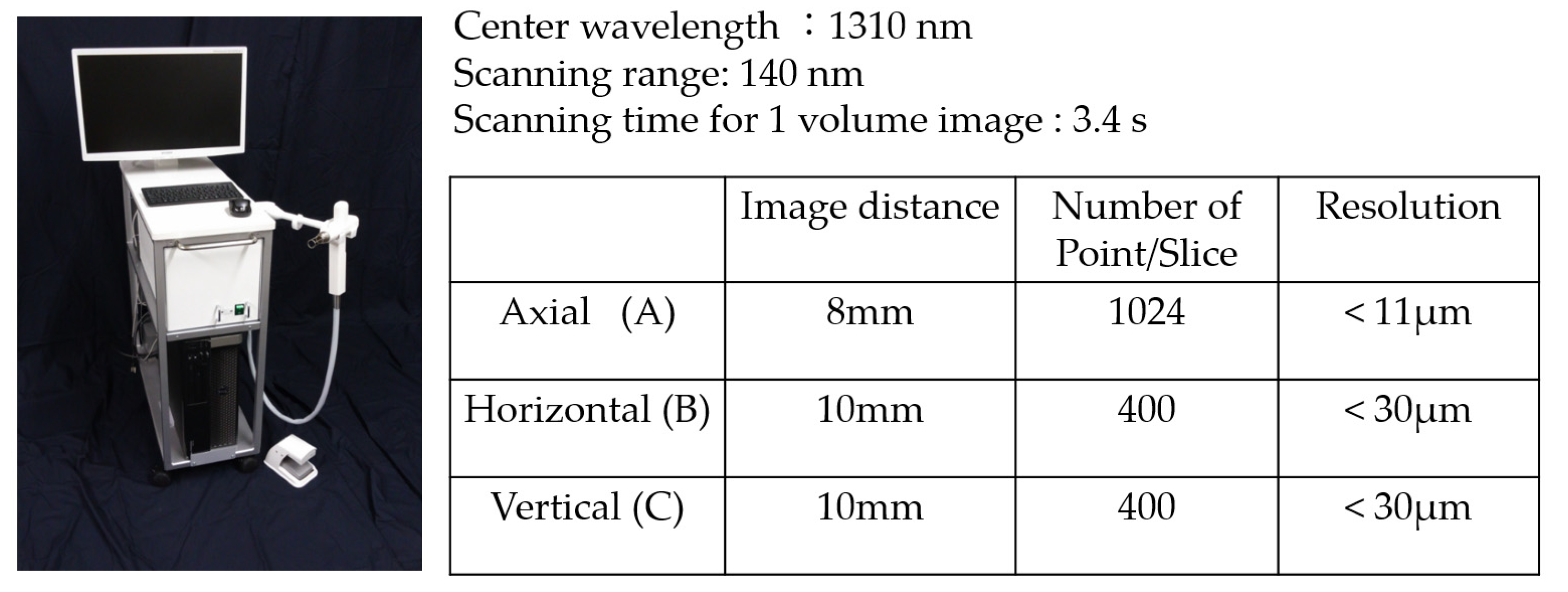
2.3. SS-OCT System
2.4. Evaluation of Enamel Lesions Using SS-OCT
- Score 0:
- No caries or demineralization of enamel. In OCT, the obtained signal was the same level as that for the surrounding normal enamel.
- Score 1:
- Shallow enamel demineralization. In OCT, the signal intensity within the outer half of enamel thickness was enhanced with no enamel surface loss.
- Score 2:
- Deep enamel demineralization. In OCT, the signal intensity within the inner half of enamel thickness was enhanced with no enamel surface loss.
- Score 3:
- Subsurface enamel demineralization with remineralization. In OCT, the signal intensity of inner enamel was enhanced but signal intensity of superficial enamel was the same level as the surrounding intact enamel. Loss of enamel was not observed.
- Score 4:
- Enamel caries with cavitated surface.
2.5. Histological Observation of Enamel Lesion
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Featherstone, J.D.B. The Continuum of Dental Caries—Evidence for a Dynamic Disease Process. J. Dent. Res. 2004, 83 (Suppl. 1), C39–C42. [Google Scholar] [CrossRef] [PubMed]
- Amaechi, B.T. Remineralisation—The buzzword for early MI caries management. Br. Dent. J. 2017, 223, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Paris, S.; Meyer-Lueckel, H.; Kielbassa, A. Resin Infiltration of Natural Caries Lesions. J. Dent. Res. 2007, 86, 662–666. [Google Scholar] [CrossRef]
- Meyer-Lueckel, H.; Wardius, A.; Krois, J.; Bitter, K.; Moser, C.; Paris, S.; Wierichs, R. Proximal Caries Infiltration—Pragmatic RCT with 4 years of follow-up. J. Dent. 2021, 111, 103733. [Google Scholar] [CrossRef] [PubMed]
- Murdoch-Kinch, C.A.; McLean, M.E. Minimally invasive dentistry. J. Am. Dent. Assoc. 2003, 134, 87–95. [Google Scholar] [CrossRef]
- Wendt, L.K.; Koch, G.; Birkhed, D. Replacements of restorations in the primary and young permanent dentition. Swed. Dent. J. 1998, 22, 149–155. [Google Scholar]
- Mjör, I.A.; Shen, C.; Eliasson, S.T.; Richter, S. Placement and replacement of restorations in general dental practice in Iceland. Oper. Dent. 2002, 27, 117–123. [Google Scholar]
- Pitts, N.B.; Ekstrand, K.; The ICDAS Foundation. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Shimada, Y.; Sadr, A.; Burrow, M.F.; Tagami, J.; Ozawa, N.; Sumi, Y. Validation of swept-source optical coherence tomography (SS-OCT) for the diagnosis of occlusal caries. J. Dent. 2010, 38, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Validation of swept source optical coherence tomography (SS-OCT) for the diagnosis of smooth surface caries in vitro. J. Dent. 2013, 41, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Colston, B.W.; Sathyam, U.S.; DaSilva, L.B.; Everett, M.; Stroeve, P.; Otis, L.L. Dental OCT. Opt. Express 1998, 3, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, A.; Dichtl, S.; Hitzenberger, C.; Sattmann, H.; Robl, B.; Moritz, A.; Fercher, A.; Sperr, W. Polarization–Sensitive Optical Coherence Tomography of Dental Structures. Caries Res. 1999, 34, 59–69. [Google Scholar] [CrossRef]
- Shimada, Y.; Nakagawa, H.; Sadr, A.; Wada, I.; Nakajima, M.; Nikaido, T.; Otsuki, M.; Tagami, J.; Sumi, Y. Noninvasive cross-sectional imaging of proximal caries using swept-source optical coherence tomography (SS-OCT) in vivo. J. Biophotonics 2013, 7, 506–513. [Google Scholar] [CrossRef]
- Imai, K.; Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Noninvasive Cross-sectional Visualization of Enamel Cracks by Optical Coherence Tomography In Vitro. J. Endod. 2012, 38, 1269–1274. [Google Scholar] [CrossRef]
- Park, K.-J.; Schneider, H.; Haak, R. Assessment of interfacial defects at composite restorations by swept source optical coherence tomography. J. Biomed. Opt. 2013, 18, 076018. [Google Scholar] [CrossRef]
- Bakhsh, T.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Non-invasive quantification of resin–dentin interfacial gaps using optical coherence tomography: Validation against confocal microscopy. Dent. Mater. 2011, 27, 915–925. [Google Scholar] [CrossRef]
- Shimada, Y.; Burrow, M.F.; Araki, K.; Zhou, Y.; Hosaka, K.; Sadr, A.; Yoshiyama, M.; Miyazaki, T.; Sumi, Y.; Tagami, J. 3D imaging of proximal caries in posterior teeth using optical coherence tomography. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Segarra, M.; Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Three-Dimensional Analysis of Enamel Crack Behavior Using Optical Coherence Tomography. J. Dent. Res. 2016, 96, 308–314. [Google Scholar] [CrossRef]
- Hayashi, J.; Shimada, Y.; Tagami, J.; Sumi, Y.; Sadr, A. Real-Time Imaging of Gap Progress during and after Composite Polymerization. J. Dent. Res. 2017, 96, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Fried, D. Remineralization of Enamel Caries Can Decrease Optical Reflectivity. J. Dent. Res. 2006, 85, 804–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, D.; Xie, J.; Shafi, S.; Featherstone, J.D.B.; Breunig, T.M.; Le, C.Q. Imaging caries lesions and lesion progression with polarization sensitive optical coherence tomography. J. Biomed. Opt. 2002, 7, 618–628. [Google Scholar] [CrossRef]
- Hariri, I.; Sadr, A.; Nakashima, S.; Shimada, Y.; Tagami, J.; Sumi, Y. Estimation of the Enamel and Dentin Mineral Content from the Refractive Index. Caries Res. 2012, 47, 18–26. [Google Scholar] [CrossRef]
- Chan, K.H.; Tom, H.; Lee, R.C.; Kang, H.; Simon, J.C.; Staninec, M.; Darling, C.L.; Pelzner, R.B.; Fried, D. Clinical monitoring of smooth surface enamel lesions using CP-OCT during nonsurgical intervention. Lasers Surg. Med. 2016, 48, 915–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Visual Inspection | SS-OCT | Significance | |
|---|---|---|---|
| shallow demineralization | 0.67 | 0.78 | NS |
| deep demineralization | 0.15 | 0.65 | S |
| remineralization | 0.036 | 0.69 | S |
| cavitation | 0.42 | 0.83 | S |
| Visual Inspection | SS-OCT | Significance |
|---|---|---|
| 0.85 | 0.88 | NS |
| Visual Inspection | SS-OCT | Significance |
|---|---|---|
| 0.83 | 0.97 | S |
| Visual Inspection | SS-OCT | Significance |
|---|---|---|
| 0.52 | 0.77 | S |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimada, Y.; Sato, T.; Inoue, G.; Nakagawa, H.; Tabata, T.; Zhou, Y.; Hiraishi, N.; Gondo, T.; Takano, S.; Ushijima, K.; et al. Evaluation of Incipient Enamel Caries at Smooth Tooth Surfaces Using SS-OCT. Materials 2022, 15, 5947. https://doi.org/10.3390/ma15175947
Shimada Y, Sato T, Inoue G, Nakagawa H, Tabata T, Zhou Y, Hiraishi N, Gondo T, Takano S, Ushijima K, et al. Evaluation of Incipient Enamel Caries at Smooth Tooth Surfaces Using SS-OCT. Materials. 2022; 15(17):5947. https://doi.org/10.3390/ma15175947
Chicago/Turabian StyleShimada, Yasushi, Takaaki Sato, Go Inoue, Hisaichi Nakagawa, Tomoko Tabata, Yuan Zhou, Noriko Hiraishi, Tadamu Gondo, Syunsuke Takano, Kei Ushijima, and et al. 2022. "Evaluation of Incipient Enamel Caries at Smooth Tooth Surfaces Using SS-OCT" Materials 15, no. 17: 5947. https://doi.org/10.3390/ma15175947
APA StyleShimada, Y., Sato, T., Inoue, G., Nakagawa, H., Tabata, T., Zhou, Y., Hiraishi, N., Gondo, T., Takano, S., Ushijima, K., Iwabuchi, H., Tsuji, Y., Alireza, S., Sumi, Y., & Tagami, J. (2022). Evaluation of Incipient Enamel Caries at Smooth Tooth Surfaces Using SS-OCT. Materials, 15(17), 5947. https://doi.org/10.3390/ma15175947