

Additive Manufacturing of Lithium Disilicate with the LCM Process for Classic and Non-Prep Veneers: Preliminary Technical and Clinical Case Experience

 , ,
, ,
Abstract
:1. Introduction
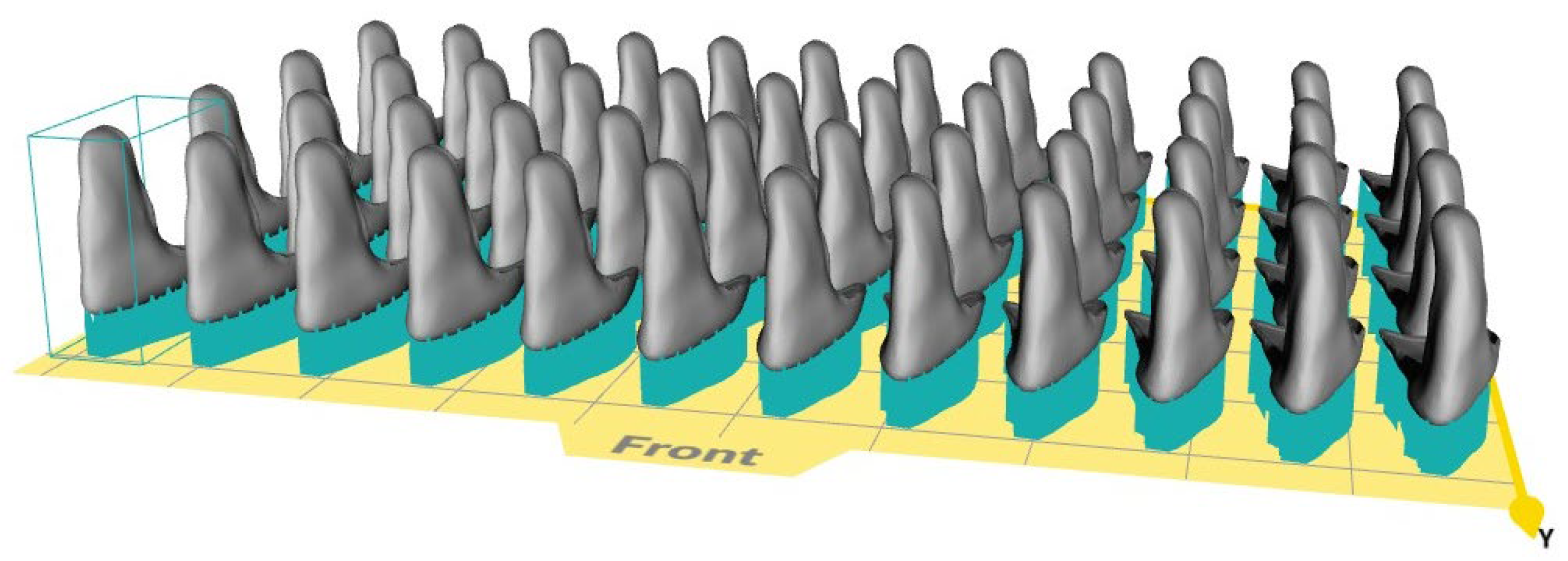
2. Materials and Methods
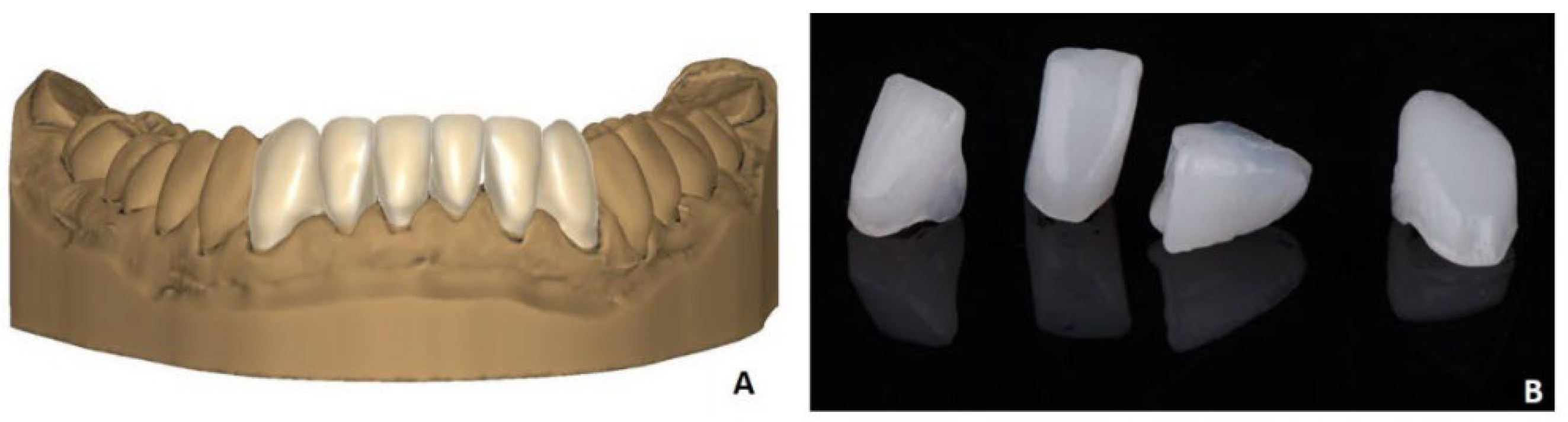
2.1. Clinical Presentation of Classic Venners
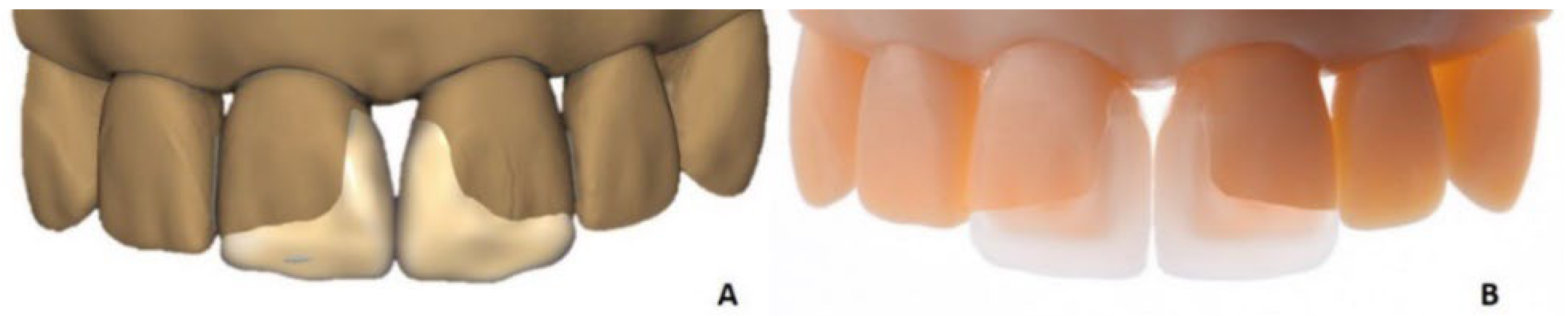
2.2. Non-Prep Veneers
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raptis, N.V.; Michalakis, K.X.; Hirayama, H. Optical behavior of current ceramic systems. Int. J. Periodontics Restor. Dent. 2006, 26, 31–41. [Google Scholar]
- Blatz, M.B.; Conejo, J. The Current State of Chairside Digital Dentistry and Materials. Dent. Clin. N. Am. 2019, 63, 175–197. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Agnini, A.; Apponi, R.; Maffei, S.; Agnini, A. Digital dental workflow for a smile makeover restoration. Int. J. Esthet. Dent. 2020, 15, 374–389. [Google Scholar] [PubMed]
- Unkovskiy, A.; Unkovskiy, N.; Spintzyk, S. A virtual patient concept for esthetic and functional rehabilitation in a fully digital workflow. Int. J. Comput. Dent. 2021, 24, 405–417. [Google Scholar] [PubMed]
- Homsy, F.R.; Özcan, M.; Khoury, M.; Majzoub, Z.A.K. Comparison of fit accuracy of pressed lithium disilicate inlays fabricated from wax or resin patterns with conventional and CAD-CAM technologies. J. Prosthet. Dent. 2018, 120, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Braian, M.; Jönsson, D.; Kevci, M.; Wennerberg, A. Geometrical accuracy of metallic objects produced with additive or subtractive manufacturing: A comparative in vitro study. Dent. Mater. 2018, 34, 978–993. [Google Scholar] [CrossRef]
- Khanlar, L.N.; Rios, A.S.; Tahmaseb, A.; Zandinejad, A. Additive Manufacturing of Zirconia Ceramic and Its Application in Clinical Dentistry: A Review. Dent. J. 2021, 9, 104. [Google Scholar] [CrossRef]
- Montelongo, S.A.; Chiou, G.; Ong, J.L.; Bizios, R.; Guda, T. Development of bioinks for 3D printing microporous, sintered calcium phosphate scaffolds. J. Mater. Sci. Mater. Med. 2021, 32, 94. [Google Scholar] [CrossRef]
- Stampfl, J. Method for the Construction of a Shaped Body. 2013. Available online: https://patents.google.com/patent/US9764513?oq=us9764513b2 (accessed on 30 June 2022).
- Baumgartner, S.; Gmeiner, R.; Schönherr, J.A.; Stampfl, J. Stereolithography-based additive manufacturing of lithium disilicate glass ceramic for dental applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 116, 111180. [Google Scholar] [CrossRef]
- Ioannidis, A.; Mühlemann, S.; Özcan, M.; Hüsler, J.; Hämmerle, C.H.F.; Benic, G.I. Ultra-thin occlusal veneers bonded to enamel and made of ceramic or hybrid materials exhibit load-bearing capacities not different from conventional restorations. J. Mech. Behav. Biomed. Mater. 2019, 90, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, A.; Bomze, D.; Hämmerle, C.H.F.; Hüsler, J.; Birrer, O.; Mühlemann, S. Load-bearing capacity of CAD/CAM 3D-printed zirconia, CAD/CAM milled zirconia, and heat-pressed lithium disilicate ultra-thin occlusal veneers on molars. Dent. Mater. 2020, 36, e109–e116. [Google Scholar] [CrossRef]
- Van Meerbeek, B. Dentin/enamel bonding. J. Esthet. Restor. Dent. 2010, 22, 157. [Google Scholar] [CrossRef]
- Gresnigt, M.M.M.; Cune, M.S.; Jansen, K.; van der Made, S.A.M.; Özcan, M. Randomized clinical trial on indirect resin composite and ceramic laminate veneers: Up to 10-year findings. J. Dent. 2019, 86, 102–109. [Google Scholar] [CrossRef]
- Garcia, P.P.; da Costa, R.G.; Calgaro, M.; Ritter, A.V.; Correr, G.M.; da Cunha, L.F.; Gonzaga, C.C. Digital smile design and mock-up technique for esthetic treatment planning with porcelain laminate veneers. J. Conserv. Dent. 2018, 21, 455–458. [Google Scholar] [CrossRef]
- Blunck, U.; Fischer, S.; Hajtó, J.; Frei, S.; Frankenberger, R. Ceramic laminate veneers: Effect of preparation design and ceramic thickness on fracture resistance and marginal quality in vitro. Clin. Oral Investig. 2020, 24, 2745–2754. [Google Scholar] [CrossRef]
- Gresnigt, M.M.M.; Cune, M.S.; Schuitemaker, J.; van der Made, S.A.M.; Meisberger, E.W.; Magne, P.; Özcan, M. Performance of ceramic laminate veneers with immediate dentine sealing: An 11 year prospective clinical trial. Dent. Mater. 2019, 35, 1042–1052. [Google Scholar] [CrossRef]
- Dolev, E.; Bitterman, Y.; Meirowitz, A. Comparison of marginal fit between CAD-CAM and hot-press lithium disilicate crowns. J. Prosthet. Dent. 2019, 121, 124–128. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Demir, N.; Ozturk, A.N.; Malkoc, M.A. Evaluation of the marginal fit of full ceramic crowns by the microcomputed tomography (micro-CT) technique. Eur. J. Dent. 2014, 8, 437–444. [Google Scholar] [CrossRef]
- Schönherr, J.A.; Baumgartner, S.; Hartmann, M.; Stampfl, J. Stereolithographic Additive Manufacturing of High Precision Glass Ceramic Parts. Materials 2020, 13, 1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ceramic material | Lithium disilicate generic color with 45 Vol% solid loading and chemical composition based on IPS e.max® Press LT (Ivoclar Vivadent AG, Liechtenstein) |
| Layer height | 25 µm |
| Number of layers | 606 |
| Layer time | 36 s |
| Runtime for whole print run | 6 h |
| Exposure intensity starting layers | 200 mJ/cm2 |
| Exposure intensity general layers | 175 mJ/cm2 |
| Lateral (XY) shrinking compensation | 1.31 |
| Build direction (Z) shrinking compensation | 1.35 |
| Z curing depth compensation | Off |
| Z curing depth compensation layers | 0 |
| Contour offset | 0 µm |
| Support structure thickness | 380 µm |
| Vat type | Ultra-High-Contrast (UHC) with CeraVat F |
| Cleaning fluid | LithaSol 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unkovskiy, A.; Beuer, F.; Metin, D.S.; Bomze, D.; Hey, J.; Schmidt, F. Additive Manufacturing of Lithium Disilicate with the LCM Process for Classic and Non-Prep Veneers: Preliminary Technical and Clinical Case Experience. Materials 2022, 15, 6034. https://doi.org/10.3390/ma15176034
Unkovskiy A, Beuer F, Metin DS, Bomze D, Hey J, Schmidt F. Additive Manufacturing of Lithium Disilicate with the LCM Process for Classic and Non-Prep Veneers: Preliminary Technical and Clinical Case Experience. Materials. 2022; 15(17):6034. https://doi.org/10.3390/ma15176034
Chicago/Turabian StyleUnkovskiy, Alexey, Florian Beuer, Dilan Seda Metin, Daniel Bomze, Jeremias Hey, and Franziska Schmidt. 2022. "Additive Manufacturing of Lithium Disilicate with the LCM Process for Classic and Non-Prep Veneers: Preliminary Technical and Clinical Case Experience" Materials 15, no. 17: 6034. https://doi.org/10.3390/ma15176034