


Impact of Irradiation on the Adhesive Performance of Resin-Based Dental Biomaterials: A Systematic Review of Laboratory Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Eligibility Criteria
2.3. Inclusion Criteria
- In vitro/laboratory study
- Use of pre-irradiation or post-irradiation bonding with a resin-based dental biomaterial (i.e., dental adhesives, resin-based composites, resin-based luting materials, resin-modified glass ionomer cements, compomers, resin-based sealants, and blocks made from resin-based composite for use in computer-aided design and computer-aided manufacturing)
- Data on adhesive performance in terms of bond strength, marginal discoloration, microleakage, marginal adaptation, debonding, or interfacial fracture toughness
- Specimens made from or featuring human or bovine enamel, dentin, or both
2.4. Exclusion Criteria
- In silico study
- Clinical study
- Animal study
- Case report
- Review article
- Study assessing laser irradiation as surface pretreatment
- Study assessing irradiation as disinfection method
- Poster
- Abstract-only paper
2.5. Search Strategy
2.6. Selection Process
2.7. Data Collection
2.8. Risk-of-Bias Assessment
3. Results
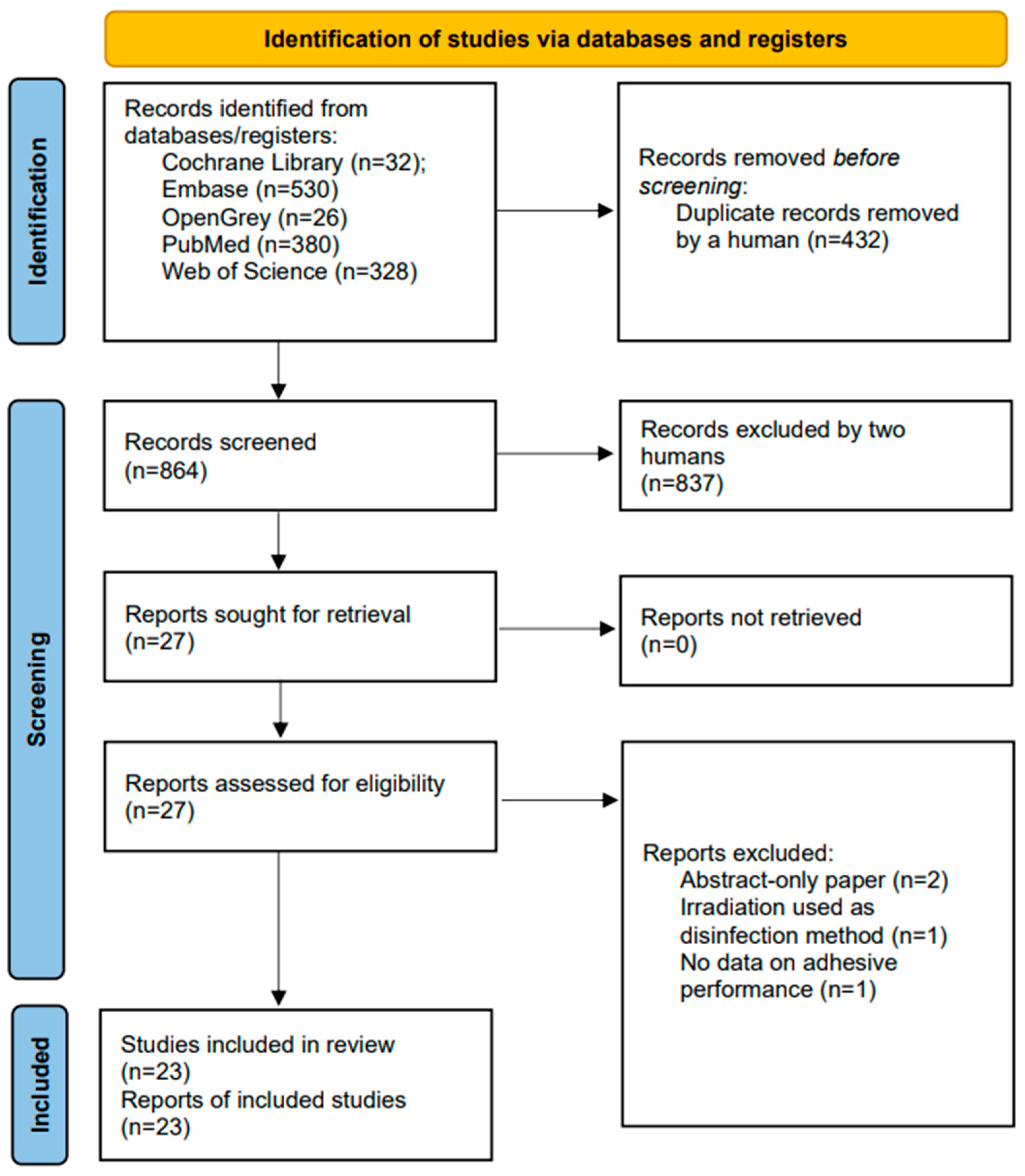
3.1. Included Studies
3.2. Characteristics of Included Studies
3.2.1. Dental Specimens
3.2.2. Bonding
3.2.3. Irradiation Protocols
3.2.4. Resin-Based Biomaterials
3.2.5. Methods to Evaluate Adhesive Performance
3.2.6. Effects of Irradiation on Bond Strength
3.2.7. Effects of Irradiation on Microleakage
3.2.8. Effects of Irradiation on Marginal Adaptation
3.3. Risk of Bias
4. Discussion
5. Conclusions
- Evidence derived from laboratory studies suggests that irradiation has a detrimental effect on the adhesive performance of resin-based dental biomaterials.
- The long-term impact of radiation on dental adhesion remains unclear, but it is plausible that the adverse effects may lessen with time between radiation therapy and the restorative procedure. However, current evidence on this is scanty.
- Significant differences have been observed in the performance of different adhesives on irradiated enamel and dentin. To achieve favorable restorative outcomes, it is, therefore, crucial to choose adhesives with a proven performance record in both laboratory and clinical studies, and to take painstaking care during bonding and buildup procedures.
- Further research is necessary to gain a comprehensive understanding of the effects of irradiation on teeth with restorations, develop methods to mitigate the adverse effects of irradiation, and explore ways to improve the efficacy of dental restorations.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Study | Dental Specimens (Enamel, Dentin, or Both; Human, Bovine, or Both) | Number of Specimens | Specimen Fabrication | Specimen Shape | Sample Grouping | Irradiation Protocol | Adhesives and Resin-Based Materials Used | Test Method(s) Used to Assess Adhesive Performance | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| Aggarwal et al., 2009 [44] | Human mandibular premolars | 60 in total (15 per group) | Quartz fiber posts bonded with an E&R adhesive and dual curing RBLM in root canal treated teeth | Root canal-treated teeth | Four groups (no irradiation, irradiation before restoration, restoration during irradiation, restoration after irradiation) | 6 weeks with daily irradiation to a total dose of 60 Gy | E&R adhesive (All Bond 2 Bisco, Schaumburg, IL, USA); dual-curing RBLM (Duolink, Bisco, Schaumburg, IL, USA) RBC build-up (Light-Core Composite resin core material, Bisco, Schaumburg, IL, USA) | Push-out bond strength | Irradiation decreased bond strength to root dentin. The timepoint of irradiation had a significant impact on bond strength, with the most detrimental effect occurring in specimens that underwent irradiation prior to restorative treatment. |
| Anushree et al., 2021 [45] | Human enamel from premolars | 66 in total (22 per group) | Metallic orthodontic brackets bonded to enamel (with or without subsequent thermocycling) | Premolars embedded in acrylic | 3 groups (unirradiated without thermocycling, unirradiated with thermocycling, irradiated with thermocycling) | 2 Gy per day for 5 consecutive days per week over 6 weeks (total dose of 60 Gy) after the bonding procedure | E&R adhesive (Transbond XT, 3M, St. Paul, MN, USA) | Shear bond strength assessment | Significant decrease in shear bond strength in irradiated specimens compared with unirradiated specimens. |
| Arid et al., 2020 [34] | Human enamel and dentin | 120 enamel and 120 dentin specimens made from 60 third molars (15 specimens per group) | Flat, ground enamel and dentin surfaces | Standardized RBC restorations (3 separate increments) | 4 groups (no irradiation, restoration immediately before irradiation, restoration immediately after irradiation, restoration 6 months after irradiation); 2 subgroups (E&R adhesive vs. SE adhesive) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (Adper Single Bond 2, 3M, St. Paul, MN, USA); SE adhesive (Clearfil SE Bond, Kuraray, Okayama, Japan) | Shear bond strength assessment | Irradiation changed the morphological surface of enamel and dentin and reduced the bond strength. The SE adhesive produced higher bond strength than the E&R adhesive. Restoration before irradiation resulted in the lowest bond strength on enamel and dentin. |
| Bulucu et al., 2006 [43] | Human dentin from molars | 30 teeth in total (six subgroups, each with 10 teeth) | Flat, ground dentin surfaces | Standardized restorations made with direct RBC | 3 main groups (no irradiation, irradiation before restoration, irradiation after restoration); two subgroups (two different adhesives) | 2 Gy per day for 5 consecutive days per week over 6 weeks (total dose of 60 Gy) before or after the bonding procedure | Two-step SE adhesive (Clearfil SE Bond, Kuraray, Japan); E&R adhesive (Prime & Bond NT, Dentsply, Milford, DE, USA); RBC (Clearfil ST, Kuraray, Okayama, Japan) | Shear bond strength assessment | Depending on the adhesive, irradiation before or after the restorative procedure can decrease bond strength. |
| Mellara et al., 2020 [30] | Human deciduous molars | 120 enamel and 120 dentin specimens made from 60 deciduous molars (4 subgroups each with 30 enamel and 30 dentin specimens) | Flat enamel and dentin surfaces | Standardized RBC restorations (RBC applied in increments) | Four groups (no irradiation, restoration immediately before irradiation, restoration 24 h after irradiation, restoration 6 months after irradiation) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (Adper Single Bond 2, 3M, St. Paul, MN, USA); SE adhesive (Clearfil SE Bond, Kuraray, Okayama, Japan) | Shear bond strength assessment | The restorations placed immediately after irradiation had the lowest shear bond strength, and the restorations placed 6 months after irradiation had similar bond strength compared with the unirradiated teeth in enamel, regardless of the adhesive system used. In dentin, the SE adhesive performed better performance than the E&R adhesive. |
| Muñoz et al., 2020 [33] | Human enamel and dentin | 52 third molars, 40 teeth used for bond strength testing (8 subgroups each with 5 specimens) | Flat, ground dentin surfaces | Standardized restorations made with direct RBC | 4 main groups (no irradiation, irradiation with 20 Gy, 40 Gy, or 70 Gy before restoration); 2 subgroups (universal adhesive applied in E&R mode vs. SE mode) | Total doses of 0 Gy, 20 Gy, 40 Gy, or 70 Gy | Universal adhesive (Scotchbond Universal Adhesive, 3M, St. Paul, MN, USA) | Shear bond strength assessment | On enamel and dentin, irradiation with ≥40 Gy decreased bond strength regardless of the adhesive strategy. The universal adhesive applied in E&R mode showed a better adhesive performance compared with the SE mode. |
| Neto et al., 2022 [46] | Human enamel | 60 human premolars | Flat enamel surface | Orthodontic brackets bonded to flat enamel surface | 4 groups with 15 teeth each (no irradiation vs. irradiation before bonding procedure; Transbond XT vs. Light Bond) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesives (Transbond XT Primer, 3M, St. Paul, MN, USA), E&R adhesive (Light Bond, Reliance Orthodontic Products, Itasca, IL, USA); RBC (Transbond XT, 3M, Monrovia, CA, USA); RBC (Light Bond, Reliance Orthodontic Products, Itasca, IL, USA) | Shear bond strength assessment | Irradiation impaired the adhesion of ceramic brackets, regardless of the RBC used for bonding. |
| Oglakci et al., 2022 [41] | Human enamel and dentin | 90 enamel and 90 dentin specimens made from 90 human molars (12 subgroups, each with 15 specimens) | Polished enamel and dentin surfaces on whole teeth | Flattened lingual and buccal surfaces of molar teeth | Enamel (control, restoration before irradiation, restoration after irradiation); dentin (control, restoration before irradiation, restoration after irradiation); adhesive applied in E&R or SE mode | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | Universal adhesive (Clearfil Universal Bond Quick, Kuraray, Okayama, Japan); RBC (Estelite Posterior Quick, Tokuyama Dental, Tokyo, Japan) | Shear bond strength assessment | On enamel, the bond strength of the universal adhesive was higher in the E&R mode and the SE mode. On dentin, the universal adhesive achieved similar bond strength in E&R and SE mode. Irradiation and the timing of the restorative procedure had no significant impact on the adhesive performance on enamel and dentin. |
| Santin et al., 2018 [36] | Human enamel from premolars | 90 teeth (6 groups with 15 specimens each) | Flat enamel surface | Orthodontic brackets bonded to flat enamel surface | Two main groups (irradiation before bonding vs. no irradiation); three subgroups (RBC, GIC, RMGIC) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (XT Primer, 3M, St. Paul, MN, USA); RBC (Transbond XT, 3M, St. Paul, MN, USA); RMGIC (Fuji Ortho LC resin, GC, Tokyo, Japan) | Shear bond strength assessment | Irradiation had no significant impact on the adhesion of brackets bonded with RBC and RMGIC. RBC and RMGIC achieved higher bond strength than GIC. |
| Santin et al., 2015 [47] | Human molars and premolars | 10 human molars and 90 human premolars (six subgroups with 15 specimens each) | Polished buccal enamel surfaces | Metallic and ceramic orthodontic brackets bonded to enamel | 2 main groups (metal and ceramic brackets bonded to enamel). Three subgroups (no irradiation, no irradiation, thermocycling after bonding; irradiation before bonding and thermocycling after bonding) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (XT Primer, 3M, St. Paul, MN, USA); RBC (Transbond XT, 3M, St. Paul, MN, USA) | Shear bond strength assessment | Irradiation decreased enamel bond strength. |
| Tikku et al., 2023 [40] | Human dentin | 100 molars (10 subgroups each with 10 teeth) | Flat, ground dentin surfaces | Standardized restorations made with direct RBC (separate, 2.5 mm thick increments) | Two main groups (irradiation after bonding vs. no irradiation); five subgroups (three different RBCs and two different GICs) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (Adper Single Bond Plus, 3M, St. Paul, MN, USA); RBC (Filtek Z250, 3M, St. Paul, MN, USA), RBC (Filtek Z350XT, 3M, St. Paul, MN, USA, RBC (Filtek Bulk Fill, 3M, St. Paul, MN, USA) | Shear bond strength assessment; marginal gap assessment | Regardless of the material, lower bond strength and larger marginal gaps were observed in specimens subjected to irradiation. |
| Bernard et al., 2015 [31] | Human dentin | 40 teeth total (10 per group) | Direct Class I restorations on molars; direct Class V restorations on premolars canines, and incisors | 1 mm2 sticks | 2 main groups (irradiated vs. unirradiated teeth) 2 subgroups (a three-step E&R adhesive vs. a two-step SE adhesive | In vivo irradiation with total dose of ≥50 Gy | Three-step E&R adhesive (Optibond FL, Kerr, Creteil, France); Two-step SE adhesive (Optibond XTR, Kerr, Creteil, France); RBC (Herculite XRV Ultra, Kerr, Creteil, France) | Microtensile bond strength | The SE adhesive achieved similar bond strength in irradiated and unirradiated teeth. The E&R adhesive achieved higher bond strengths on unirradiated than on irradiated teeth. Restorative treatment should ideally be performed before radiation therapy. |
| Galetti et al., 2014 [32] | Human dentin | 18 teeth from patients who underwent radiation therapy and 18 teeth form patients without radiation therapy (divided into six subgroups, each with 6 specimens) | Flat, ground dentin surfaces | Standardized restorations made with direct RBC | Two main groups (irradiated teeth vs. unirradiated teeth); three subgroups (three different adhesives) | Clinical radiation therapy prior to tooth removal (total dose 60–70 Gy) | E&R adhesive (Single Bond 2, 3M, St. Paul, MN, USA); two step SE adhesives (Easy Bond, 3M, St. Paul, MN, USA), SE adhesive (Clearfil SE Bond, Kuraray, Okayama, Japan) | Microtensile bond strength assessment | No significant difference was observed between irradiated and unirradiated teeth. The adhesives obtained similar bond strength. |
| Gernhardt et al., 2001 [42] | Human third molars | 120 teeth in total (60 with and 60 without irradiation) 4 subgroups, each with 15 specimens | Occlusal surface ground to expose dentin With simulated intra-pulpal pressure | Flat, ground dentin surfaces | 2 main groups (irradiated vs. unirradiated) 4 subgroups (4 different adhesives) | 5 days/week to a total dose of 60 Gy | Universal Adhesive (Scotchbond 1, 3M, Loughborough, UK); Universal Adhesive (Solobond Plus, Voco, Cuxhaven, Germany); 2-step E&R adhesive (Prime & Bond 2.1, DeTrey Dentsply, Dreieich, Germany); 4-step total etch adhesive (Syntac, Vivadent, Schaan, Liechtenstein); RBC (Tetric, Vivadent, Schaan, Lichtenstein) | Tensile bond strength | Irradiation had no significant influence on adhesion of RBC to dentin. On irradiated dentin, Scotchbond 1 obtained higher bond strength than Solobond Plus, and Prime & Bond obtained higher bond strength than Solobond Plus. |
| Keles et al., 2018 [29] | Enamel and dentin from deciduous human molars | 35 deciduous molars (7 subgroups with 5 specimens each) | Flat enamel and dentin surfaces | Standardized compomer restorations (3 separate increments, each 2 mm thick) | Six groups (no irradiation, 10 Gy, 20 Gy, 30 Gy, 40 Gy, 50 Gy, or 60 Gy before restorative procedure) | 2 Gy daily for 5 days per week over a maximum of 6 weeks (total dose 10–60 Gy) | SE adhesive (Futurabond M, Voco, Cuxhaven, Germany); compomer restorative resin-based material (Glossiosit, Voco, Cuxhaven, Germany | Microtensile bond strength assessment | No statistically significant difference was found between the irradiated tooth enamel and the control group. A dose-dependent decrease in bond strength was found on dentin of deciduous molars. |
| Naves et al., 2012 [37] | Human enamel and dentin | 120 specimens made from 30 third molars (40 specimens per group) | Flat, ground enamel and dentin surfaces | Standardized RBC restorations (3 separate increments) | Enamel and dentin specimens without irradiation; enamel and dentin specimens with irradiation before restoration; enamel and dentin specimens with irradiation after restoration | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | E&R adhesive (Adper Single Bond 2, 3M, St, Paul, MN, USA); RBC (Filtek Z250, 3M, St. Paul, MN, USA) | Microtensile bond strength assessment | Irradiation reduced bond strength to human enamel and dentin when the adhesive procedure was performed after irradiation. When the adhesive procedure was performed before irradiation, no significant change in bond strength was observed. |
| Rodrigues et al., 2018 [38] | Dentin from human third molars | 43 specimens (depending on the type of assessment, the subgroups comprised 1–10 specimens) | Standardized sections of dentin | Standardized restorations made with direct RBC (separate increments) | Three groups (no irradiation, irradiation before restoration, irradiation after restoration) | 1.8 Gy daily, 5 days per week, for 8 weeks (total dose 72 Gy) | E&R adhesive (Scotchbond Multi-Purpose, 3M, St. Paul, MN, USA); RBC (Filtek Z350 XT, 3M, St. Paul, MN, USA) | Microtensile bond strength assessment | In the group with irradiation before the restorative procedure, significantly lower bond strengths were observed compared with the other groups. |
| Soares et al., 2016 [39] | Human dentin | 60 human molars (12 subgroups with 5 specimens each) | Flat, ground dentin surfaces | Standardized restorations made with direct RBC (separate, 2.0 mm thick increments) | Three main groups (no irradiation, irradiation before restoration, irradiation after restoration); four subgroups (two different adhesives with and without prior application of doxycycline) | 2 Gy daily for 5 days per week over six weeks (total dose 60 Gy) | E&R adhesive (Adper Scotchbond Multi-Purpose, 3M, St. Paul, MN, USA); SE adhesive (Clearfil SE Bond, Kuraray, Okayama, Japan); RBC (Filtek Z250, 3M, St. Paul, MN, USA) | Microtensile bond strength assessment | Irradiation before the adhesive procedure decreased bond strength. No statistical difference was observed between the adhesive systems. |
| Bulucu et al., 2009 [49] | Human enamel and dentin from molars | 84 teeth in total (six subgroups, each with 14 teeth) | Direct Class V restorations in molars (cavities margins in enamel and dentin) | Box-shaped Class V cavities and direct restorations | 2 main groups (irradiation after restoration vs. no irradiation), three subgroups (three different adhesives) | 2 Gy per day for 5 consecutive days per week over 6 weeks (total dose of 60 Gy) after the bonding procedure | One-step SE adhesive (Clearfil S3 Bond, 3M, St. Paul, MN, USA); a two-step SE adhesive (Clearfil SE Bond, 3M, St. Paul, MN, USA); a E&R adhesive (Prime & Bond NT, Dentsply, Milford, DE, USA); RBC (Filtek Z250, 3M, St. Paul, MN, USA) | Microleakage assessment using dye penetration | No statistically significant differences in microleakage were found between irradiated and unirradiated specimens. Specimens bonded with SE adhesives showed less microleakage at cervical margins than the E&R adhesive. |
| Gupta et al., 2022 [35] | Human premolars | 75 teeth (5 groups with 15 teeth each) | Direct Class V restorations on buccal surfaces; thermocycling; preparation of sections | Direct Class V restorations on buccal surfaces | 5 groups ( no irradiation; irradiation before restoration; irradiation with shielding before restoration; irradiation after restoration; irradiation with shielding after restoration) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | SE adhesive (Adper Easy 1, 3M, St. Paul, MN, USA); RBC (Valux Plus, 3M, St. Paul, MN, USA)) | Microleakage assessment using dye penetration | Irradiation increased microleakage. Microleakage was higher if restorations were placed after irradiation. Shielding reduced microleakage. Restorations should ideally be placed before irradiation. |
| Jornet et al., 2013 [28] | Bovine incisors | 60 teeth in total (6 groups with 10 specimens each) | Direct RBC restorations | Class V restorations in anterior teeth | 2 main groups (irradiated after restoration vs. unirradiated specimens) 3 subgroups (storage in artificial saliva, fluoride solution, or chlorhexidine) | 2 Gy daily for 5 days per week over 6 weeks (total dose 60 Gy) | Universal adhesive (Single Bond, 3M, St. Paul, MN, USA); RBC (Z250, 3M St. Paul, MN, USA) | Microleakage assessment using methylene blue penetration | Irradiated teeth showed more microleakage. Irradiated teeth immersed in chlorhexidine showed the highest leakage. Among irradiated teeth, those immersed in fluoride solution showed the lowest leakage. |
| Rasmy et al., 2017 [48] | Human enamel and dentin | 40 teeth, 80 specimens of buccal and lingual segments (20 specimens per group) | Class V restorations | Standardized Class V restorations made with direct RBC | Two main groups (irradiation before bonding vs. no irradiation); two subgroups (enamel conditioning with laser vs. phosphoric acid) | 60 Gy | E&R adhesive (Adper Single Bond, 3M, St. Paul, MN, USA); RBC (Filtek Z 250, 3M, St. Paul, MN, USA) | Microleakage assessment | Favorable results were found in specimens without irradiation. Regardless of the surface conditioning, a high degree of microleakage was found in specimens with irradiation. |
| Oglakci et al., 2022b [18] | Human molars | 60 in total (six subgroups, each with 10 specimens) | MOD restorations evaluated at the enamel and dentin margins | Molar teeth with MOD restorations | 3 main groups (no irradiation; irradiation before restoration; irradiation after restoration); 2 subgroups (universal adhesive applied in E&R or SE mode) | 60 Gy at 2 Gy/day, 5 days a week for 6 weeks | Universal adhesive (Clearfil Universal Bond Quick, Kuraray, Okayama, Japan); RBC (Estelite Posterior Quick, Tokuyama Dental, Tokyo, Japan) | Analysis of marginal adaptation done using X-ray microtomography | Irradiation did not affect the marginal adaptation of the universal adhesive at the cervical regions. In specimens subjected to irradiation before the restorative procedure, more adhesive defects at the dentin margin were observed in the SE group than in the E&R group. |
| D1 | D2 | D3 | D4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | (1.1) Control Group | (1.2) Randomization of Samples | (1.3) Sample Size Rationale and Reporting | (2.1) Standardization of Samples and Materials | (2.2) Identical Experimental Conditions Across Groups | (3.1) Adequate and Standardized Testing Procedures and Outcomes | (3.2) Blinding of the Test Operator | (4.1) Statistical Analysis | (4.2) Reporting Study Outcomes |
| Aggarwal et al., 2009 [44] | 1 | 3 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Anushree et al., 2021 [45] | 1 | 2 | 1 | 1 | 1 | 1 | 3 | 1 | 1 |
| Arid et al., 2020 [34] | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 1 |
| Bernard et al., 2015 [31] | 1 | 2 | 2 | 1 | 1 | 1 | 3 | 1 | 1 |
| Bulucu et al., 2006 [43] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Bulucu et al., 2009 [49] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Galetti et al., (2014) [32] | 1 | 2 | 3 | 3 | 1 | 1 | 3 | 1 | 1 |
| Gernhardt et al., 2001 [42] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Gupta et al., 2022 [35] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Jornet et al., 2013 [28] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Keles et al., 2018 [29] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Mellara et al., 2020 [30] | 1 | 2 | 3 | 1 | 1 | 1 | 1 | 1 | 1 |
| Muñoz et al., 2020 [33] | 1 | 1 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Naves et al., 2012 [37] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Neto et al., 2022 [46] | 1 | 2 | 1 | 1 | 1 | 1 | 3 | 1 | 1 |
| Oglakci et al., 2022 [41] | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Oglakci et al., 2022 [18] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Rasmy et al., 2017 [48] | 1 | 3 | 3 | 1 | 1 | 2 | 1 | 1 | 1 |
| Rodrigues et al., 2018 [38] | 1 | 2 | 3 | 1 | 1 | 2 | 3 | 1 | 1 |
| Santin et al., 2018 [36] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Santin et al., 2015 [47] | 1 | 3 | 3 | 1 | 2 | 1 | 3 | 2 | 2 |
| Soares et al., 2016 [39] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
| Tikku et al., 2023 [40] | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 1 | 1 |
References
- Patterson, R.H.; Fischman, V.G.; Wasserman, I.; Siu, J.; Shrime, M.G.; Fagan, J.J.; Koch, W.; Alkire, B.C. Global burden of head and neck cancer: Economic consequences, health, and the role of surgery. Otolaryngol. Head Neck Surg. 2020, 162, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourhis, J.; Overgaard, J.; Audry, H.; Ang, K.K.; Saunders, M.; Bernier, J.; Horiot, J.-C.; Le Maître, A.; Pajak, T.F.; Poulsen, M.G.; et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: A meta-analysis. Lancet 2006, 368, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and neck cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Pignon, J.-P.; Le Maître, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Winquist, E.; Agbassi, C.; Meyers, B.M.; Yoo, J.; Chan, K.K.W. Systemic therapy in the curative treatment of head and neck squamous cell cancer: A systematic review. J. Otolaryngol. Head Neck Surg. 2017, 46, 29. [Google Scholar] [CrossRef]
- Sroussi, H.Y.; Epstein, J.B.; Bensadoun, R.-J.; Saunders, D.P.; Lalla, R.V.; Migliorati, C.A.; Heaivilin, N.; Zumsteg, Z.S. Common oral complications of head and neck cancer radiation therapy: Mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017, 6, 2918–2931. [Google Scholar] [CrossRef]
- Moore, C.; McLister, C.; Cardwell, C.; O’Neill, C.; Donnelly, M.; McKenna, G. Dental caries following radiotherapy for head and neck cancer: A systematic review. Oral Oncol. 2020, 100, 104484. [Google Scholar] [CrossRef]
- Dezanetti, J.M.P.; Nascimento, B.L.; Orsi, J.S.R.; Souza, E.M. Effectiveness of glass ionomer cements in the restorative treatment of radiation-related caries—A systematic review. Support. Care Cancer 2022, 30, 8667–8678. [Google Scholar] [CrossRef]
- Palmier, N.R.; Prado-Ribeiro, A.C.; Mariz, B.A.L.A.; Rodrigues-Oliveira, L.; Paglioni, M.d.P.; Napimoga, J.T.C.; Pedroso, C.M.; Morais-Faria, K.; Oliveira, M.C.Q.d.; Vechiato-Filho, A.J.; et al. The impact of radiation caries on morbidity and mortality outcomes of head and neck squamous cell carcinoma patients. Spec. Care Dentist. 2023. [Google Scholar] [CrossRef] [PubMed]
- Douchy, L.; Gauthier, R.; Abouelleil-Sayed, H.; Colon, P.; Grosgogeat, B.; Bosco, J. The effect of therapeutic radiation on dental enamel and dentin: A systematic review. Dent. Mater. 2022, 38, e181–e201. [Google Scholar] [CrossRef] [PubMed]
- Lieshout, H.F.J.; Bots, C.P. The effect of radiotherapy on dental hard tissue--a systematic review. Clin. Oral Investig. 2014, 18, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Mante, F.K.; Kim, A.; Truong, K.N.; Mittal, K.; Alapati, S.; Hagan, S.; Deng, J. Effect of preirradiation fluoride treatment on the physical properties of dentin. Int. J. Dent. 2022, 2022, 3215048. [Google Scholar] [CrossRef]
- Gupta, N.; Pal, M.; Rawat, S.; Grewal, M.S.; Garg, H.; Chauhan, D.; Ahlawat, P.; Tandon, S.; Khurana, R.; Pahuja, A.K.; et al. Radiation-induced dental caries, prevention and treatment—A systematic review. Natl. J. Maxillofac. Surg. 2015, 6, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Hong, C.H.L.; Hu, S.; Haverman, T.; Stokman, M.; Napeñas, J.J.; Braber, J.B.; Gerber, E.; Geuke, M.; Vardas, E.; Waltimo, T.; et al. A systematic review of dental disease management in cancer patients. Support. Care Cancer 2018, 26, 155–174. [Google Scholar] [CrossRef]
- Bornstein, M.; Filippi, A.; Buser, D. Early and late intraoral sequelae after radiotherapy. Schweiz. Monatsschr. Zahnmed. 2001, 111, 61–73. [Google Scholar]
- Oglakci, B.; Burduroglu, D.; Eris, A.H.; Mayadagli, A.; Arhun, N. The effect of radiotherapy on the marginal adaptation of Class II direct resin composite restorations: A micro-computed tomography analysis. Oper. Dent. 2022, 47, 43–54. [Google Scholar] [CrossRef]
- Heintze, S.D.; Loguercio, A.D.; Hanzen, T.A.; Reis, A.; Rousson, V. Clinical efficacy of resin-based direct posterior restorations and glass-ionomer restorations—An updated meta-analysis of clinical outcome parameters. Dent. Mater. 2022, 38, e109–e135. [Google Scholar] [CrossRef]
- Peumans, M.; Kanumilli, P.; de Munck, J.; van Landuyt, K.; Lambrechts, P.; van Meerbeek, B. Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dent. Mater. 2005, 21, 864–881. [Google Scholar] [CrossRef]
- Ma, K.S.-K.; Wang, L.-T.; Blatz, M.B. Efficacy of adhesive strategies for restorative dentistry: A systematic review and network meta-analysis of double-blind randomized controlled trials over 12 months of follow-up. J. Prosthodont. Res. 2023, 67, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.H.; Sauro, S.; Lima, A.F.; Loguercio, A.D.; Della Bona, A.; Mazzoni, A.; Collares, F.M.; Staxrud, F.; Ferracane, J.; Tsoi, J.; et al. RoBDEMAT: A risk of bias tool and guideline to support reporting of pre-clinical dental materials research and assessment of systematic reviews. J. Dent. 2022, 127, 104350. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, A.; Francisco De Oliveira, H.; Nelson Filho, P.; Arid, J.; Guenca Paula Dibb, R.; Assed Bezerra Da Silva, L.; Assed Segato, R. Effect of radiotherapy on bonding and bonding interface to substrate of permanent teeth. Radiother. Oncol. 2018, 127, S613–S614. [Google Scholar] [CrossRef]
- Queiroz, A.; Mellara, T.; Nelson-Filho, P.; Arid, J.; Romano, J.; Oliveira, H.; Palma-Dibb, R. Radiotherapy impairs on the bonding system in primary teeth. Radiother. Oncol. 2017, 123, S1014–S1015. [Google Scholar] [CrossRef]
- Titley, K.C.; Chernecky, R.; Rossouw, P.E.; Kulkarni, G.V. The effect of various storage methods and media on shear-bond strengths of dental composite resin to bovine dentine. Arch. Oral Biol. 1998, 43, 305–311. [Google Scholar] [CrossRef]
- Gernhardt, C.R.; Koravu, T.; Gerlach, R.; Schaller, H.G. The influence of dentin adhesives on the demineralization of irradiated and non-irradiated human root dentin. Oper. Dent. 2004, 29, 454–461. [Google Scholar]
- Lopez Jornet, P.; Camacho Alonso, F.; Molina Minano, F. Application of chlorhexidine, fluoride and artificial saliva during radiotherapy: An in vitro study of microleakage in Class V restorations. Aust. Dent. J. 2013, 58, 339–343. [Google Scholar] [CrossRef]
- Keles, S.; Yilmaz, Y.; Sezen, O. Microtensile bond strength of polyacid-modified composite resin to irradiated primary molars. J. Contemp. Dent. Pract. 2018, 19, 189–195. [Google Scholar] [CrossRef]
- Mellara, T.d.S.; Garcia Paula-Silva, F.W.; Arid, J.; de Oliveira, H.F.; Nelson-Filho, P.; Bezerra Silva, R.A.; Torres, F.M.; Faraoni, J.J.; Palma-Dibb, R.G.; de Queiroz, A.M. Radiotherapy impairs adhesive bonding in primary teeth: An in vitro study. J. Dent. Child. 2020, 87, 69–76. [Google Scholar]
- Bernard, C.; Villat, C.; Abouelleil, H.; Gustin, M.-P.; Grosgogeat, B. Tensile bond strengths of two adhesives on irradiated and nonirradiated human dentin. BioMed Res. Int. 2015, 2015, 798972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galetti, R.; Santos-Silva, A.R.; Antunes, A.N.; Alves, F.; Lopes, M.A.; de Goes, M.F. Radiotherapy does not impair dentin adhesive properties in head and neck cancer patients. Clin. Oral Investig. 2014, 18, 1771–1778. [Google Scholar] [CrossRef]
- Muñoz, M.A.; Garín-Correa, C.; González-Arriagada, W.; Quintela Davila, X.; Häberle, P.; Bedran-Russo, A.; Luque-Martínez, I. The adverse effects of radiotherapy on the structure of dental hard tissues and longevity of dental restoration. Int. J. Radiat. Biol. 2020, 96, 910–918. [Google Scholar] [CrossRef]
- Arid, J.; Palma-Dibb, R.G.; de Oliveira, H.F.; Nelson-Filho, P.; de Carvalho, F.K.; Da Silva, L.; de Siqueira Mellara, T.; Da Silva, R.; Faraoni, J.J.; de Queiroz, A.M. Radiotherapy impairs adhesive bonding in permanent teeth. Support. Care Cancer 2020, 28, 239–247. [Google Scholar] [CrossRef]
- Gupta, S.; Bogra, P.; Sharma, D.; Goyal, R.; Dhir, S.; Gupta, B. Impact of radiotherapy and shielding on the efficacy of the self-etch adhesive technique. J. Conserv. Dent. 2022, 25, 444–447. [Google Scholar] [CrossRef]
- Santin, G.C.; Queiroz, A.M.; Palma-Dibb, R.G.; Oliveira, H.F.; Nelson Filho, P.; Romano, F.L. Glass ionomer cements can be used for bonding orthodontic brackets after cancer radiation treatment? Braz. Dent. J. 2018, 29, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naves, L.Z.; Novais, V.R.; Armstrong, S.R.; Correr-Sobrinho, L.; Soares, C.J. Effect of gamma radiation on bonding to human enamel and dentin. Support. Care Cancer 2012, 20, 2873–2878. [Google Scholar] [CrossRef]
- Rodrigues, R.B.; Soares, C.J.; Junior, P.C.S.; Lara, V.C.; Arana-Chavez, V.E.; Novais, V.R. Influence of radiotherapy on the dentin properties and bond strength. Clin. Oral Investig. 2018, 22, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Freitas Soares, E.; Zago Naves, L.; Bertolazzo Correr, A.; Costa, A.R.; Consani, S.; Soares, C.J.; Garcia-Godoy, F.; Correr-Sobrinho, L. Effect of radiotherapy, adhesive systems and doxycycline on the bond strength of the dentin-composite interface. Am. J. Dent. 2016, 29, 352–356. [Google Scholar]
- Tikku, A.P.; Bhatt, M.; Painuly, N.K.; Bharti, R.; Bains, R.; Misra, S. Shear bond strength analysis and marginal gap evaluation of restoration-tooth interface of aesthetic restorations after simulated Co-60 gamma irradiation. J. Radiother. Pract. 2023, 22, e13. [Google Scholar] [CrossRef]
- Oglakci, B.; Burduroglu, D.; Eri, A.H.; Mayadagli, A.; Arhun, N. How does radiotherapy affect the adhesion of universal adhesive to enamel and dentin? A qualitative and quantitative analysis? Odovtos-Int. J. Dent. Sc. 2022, 24, 75–90. [Google Scholar] [CrossRef]
- Gernhardt, C.R.; Kielbassa, A.M.; Hahn, P.; Schaller, H.G. Tensile bond strengths of four different dentin adhesives on irradiated and non-irradiated human dentin in vitro. J. Oral Rehabil. 2001, 28, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Bulucu, B.; Yesilyurt, C.; Çakir, S.; Meydan, A.D. Influence of radiation on bond strength. J. Adhes. Dent. 2006, 8, 217–221. [Google Scholar] [PubMed]
- Aggarwal, V. An in vitro evaluation of effect of ionizing radiotherapy on push-out strength of fiber posts under cyclic loading. J. Endod. 2009, 35, 695–698. [Google Scholar] [CrossRef] [PubMed]
- Anushree, A.; Shetty, A.; Soans, C.R.; Kuttappa, M.N.; Shetty, A.; Shetty, K.; Nayak, U.S.K. Evaluation of physical and adhesive properties of enamel after a therapeutic dose of radiation and bonding of orthodontic metal brackets: An in vitro study. J. Radiother. Pract. 2021, 20, 78–82. [Google Scholar] [CrossRef]
- Neto, A.T.; Amaral, F.; Romano, F. Effects of ionizing radiation and different resin composites on shear strength of ceramic brackets: An in vitro study. Dental Press J. Orthod. 2022, 27, e2219330. [Google Scholar] [CrossRef]
- Santin, G.C.; Palma-Dibb, R.G.; Romano, F.L.; de Oliveira, H.F.; Nelson Filho, P.; de Queiroz, A.M. Physical and adhesive properties of dental enamel after radiotherapy and bonding of metal and ceramic brackets. Am. J. Orthod. Dentofacial Orthop. 2015, 148, 283–292. [Google Scholar] [CrossRef]
- Rasmy, A.; Harhash, T.A.; Ghali, R.; El Maghraby, E.; El Rouby, D.H. Comparative study between laser and conventional techniques for Class V cavity preparation in gamma-irradiated teeth (in vitro study). J. Appl. Oral Sci. 2017, 25, 657–665. [Google Scholar] [CrossRef] [Green Version]
- Bulucu, B.; Avsar, A.; Demiryürek, E.O.; Yesilyurt, C. Effect of radiotherapy on the microleakage of adhesive systems. J. Adhes. Dent. 2009, 11, 305–309. [Google Scholar]
- Lu, H.; Zhao, Q.; Guo, J.; Zeng, B.; Yu, X.; Yu, D.; Zhao, W. Direct radiation-induced effects on dental hard tissue. Radiat. Oncol. 2019, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Cuevas-Suárez, C.E.; da Rosa, W.L.d.O.; Lund, R.G.; da Silva, A.F.; Piva, E. Bonding performance of universal adhesives: An updated systematic review and meta-analysis. J. Adhes. Dent. 2019, 21, 7–26. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, S.S.; Cesar, P.F.; Swain, M.V. Direct comparison of the bond strength results of the different test methods: A critical literature review. Dent. Mater. 2010, 26, e78–e93. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Keam, B.; Ahn, S.-H.; Choi, C.H.; Wu, H.-G. Feasibility and safety of neck level IB-sparing radiotherapy in nasopharyngeal cancer: A long-term single institution analysis. Radiat. Oncol. J. 2022, 40, 260–269. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eggmann, F.; Hwang, J.D.; Ayub, J.M.; Mante, F.K. Impact of Irradiation on the Adhesive Performance of Resin-Based Dental Biomaterials: A Systematic Review of Laboratory Studies. Materials 2023, 16, 2580. https://doi.org/10.3390/ma16072580
Eggmann F, Hwang JD, Ayub JM, Mante FK. Impact of Irradiation on the Adhesive Performance of Resin-Based Dental Biomaterials: A Systematic Review of Laboratory Studies. Materials. 2023; 16(7):2580. https://doi.org/10.3390/ma16072580
Chicago/Turabian StyleEggmann, Florin, Jonathan D. Hwang, Jose M. Ayub, and Francis K. Mante. 2023. "Impact of Irradiation on the Adhesive Performance of Resin-Based Dental Biomaterials: A Systematic Review of Laboratory Studies" Materials 16, no. 7: 2580. https://doi.org/10.3390/ma16072580
APA StyleEggmann, F., Hwang, J. D., Ayub, J. M., & Mante, F. K. (2023). Impact of Irradiation on the Adhesive Performance of Resin-Based Dental Biomaterials: A Systematic Review of Laboratory Studies. Materials, 16(7), 2580. https://doi.org/10.3390/ma16072580