
Advancing Pulmonary Nodule Diagnosis by Integrating Engineered and Deep Features Extracted from CT Scans



Abstract

1. Introduction
2. Materials and Methods
2.1. Engineered Features
2.1.1. Local Binary Pattern (LBP)
- Nodule Misclassification: Traditional LBP’s sensitivity to noise may incorrectly identify benign nodules as malignant, affecting patient treatment and prognosis.
- Diagnostic Accuracy Decline: Noise and distortions compromise LBP’s textural analysis, lowering the reliability of lung nodule diagnosis and potentially delaying appropriate treatment.
2.1.2. 3D-Local Octal Pattern (LOP)
2.1.3. Texture Direction
2.1.4. Texture Magnitude
2.1.5. Model Deployment
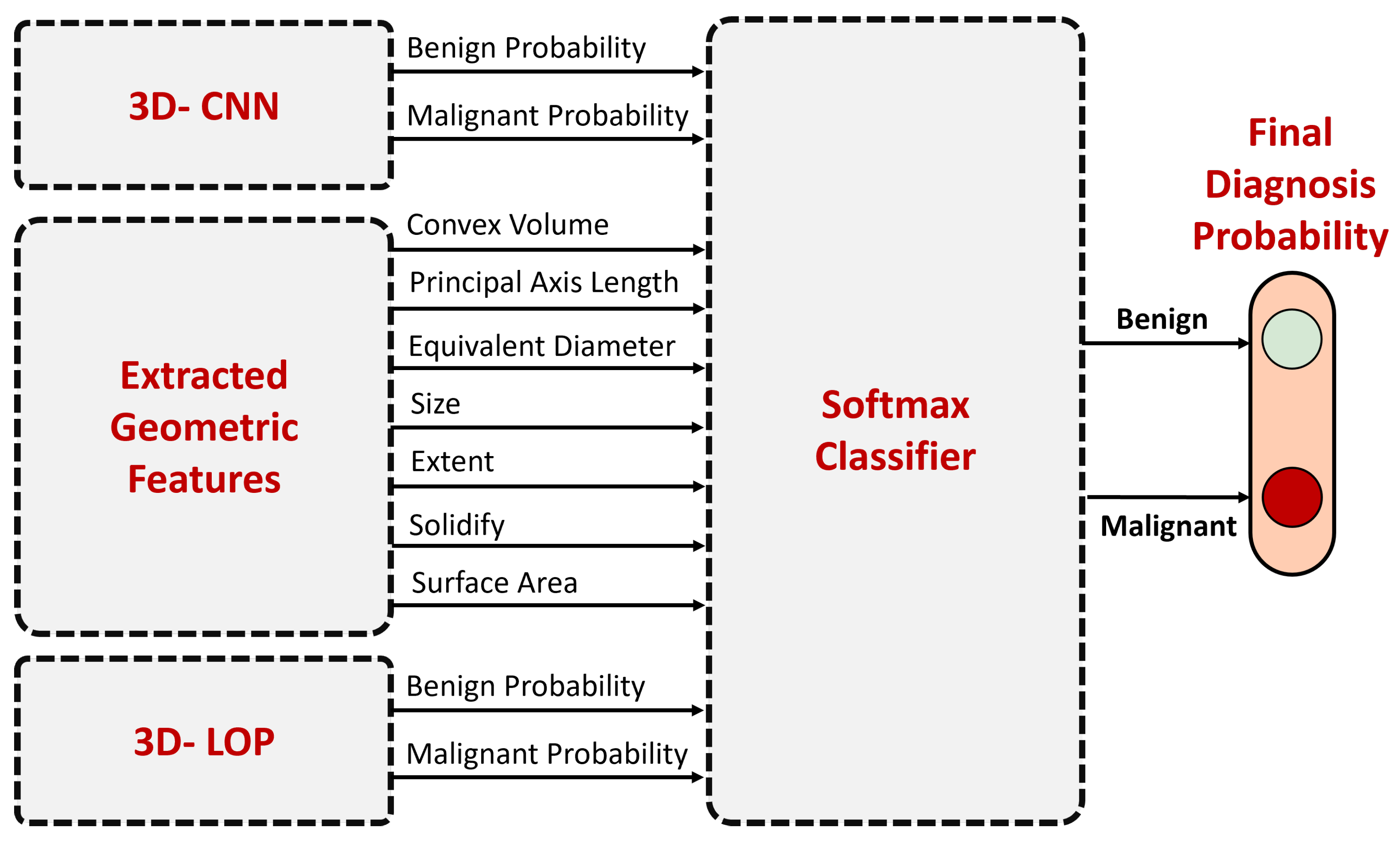
2.2. Deep Features and Fusion
- Convex Volume ():Equation:Description: The sum of voxels () within the nodule’s convex hull.
- Volume (V):Equation:Description: The total count of voxels () composing the nodule.
- Equivalent Diameter ():Equation:Description: Diameter of an equivalent-volume sphere.
- Surface Area ():Equation: [Complex calculations involving voxel neighborhood assessments]Description: Total area surrounding the nodule’s boundary.
- Solidity (S):Equation:Description: Ratio of voxel count within the nodule to that within its convex hull.
- Principal Axis Length:Equation: Derived from the eigenvalues () of the covariance matrix.Description: Major axes lengths of the corresponding ellipsoid.
- Extent (E):Equation:Description: Proportion of nodules’ voxels to total voxels in the bounding box.
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Team, N.L.S.T.R. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar]
- Siddiqui, E.A.; Chaurasia, V.; Shandilya, M. Detection and classification of lung cancer computed tomography images using a novel improved deep belief network with Gabor filters. Chemom. Intell. Lab. Syst. 2023, 235, 104763. [Google Scholar] [CrossRef]
- El Hamdi, D.; Elouedi, I.; Slim, I. Computer-Aided Classification of Cell Lung Cancer Via PET/CT Images Using Convolutional Neural Network. Int. J. Image Graph. 2023, 2450040. [Google Scholar] [CrossRef]
- Raza, R.; Zulfiqar, F.; Khan, M.O.; Arif, M.; Alvi, A.; Iftikhar, M.A.; Alam, T. Lung-EffNet: Lung cancer classification using EfficientNet from CT-scan images. Eng. Appl. Artif. Intell. 2023, 126, 106902. [Google Scholar] [CrossRef]
- Thakur, S.K.; Singh, D.P.; Choudhary, J. Lung cancer: Detection and classification of malignancies. In Proceedings of the Artificial Intelligence and Sustainable Computing: Proceedings of ICSISCET 2020; Springer: Berlin/Heidelberg, Germany, 2022; pp. 451–463. [Google Scholar]
- Shafi, I.; Din, S.; Khan, A.; Díez, I.D.L.T.; Casanova, R.d.J.P.; Pifarre, K.T.; Ashraf, I. An effective method for lung cancer diagnosis from ct scan using deep learning-based support vector network. Cancers 2022, 14, 5457. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, T.I.; Oyelade, O.N.; Ezugwu, A.E. Automatic detection and classification of lung cancer CT scans based on deep learning and ebola optimization search algorithm. PLoS ONE 2023, 18, e0285796. [Google Scholar] [CrossRef] [PubMed]
- Dodia, S.; Annappa, B.; Padukudru, M.A. A novel bi-level lung cancer classification system on CT scans. In Proceedings of the Annual Conference On Medical Image Understanding and Analysis; Springer: Berlin/Heidelberg, Germany, 2022; pp. 578–593. [Google Scholar]
- Xu, Y.; Wang, S.; Sun, X.; Yang, Y.; Fan, J.; Jin, W.; Li, Y.; Su, F.; Zhang, W.; Cui, Q.; et al. Identification of benign and malignant lung nodules in CT images based on ensemble learning method. Interdiscip. Sci. Comput. Life Sci. 2022, 14, 130–140. [Google Scholar] [CrossRef] [PubMed]
- AR, B. A deep learning-based lung cancer classification of CT images using augmented convolutional neural networks. ELCVIA Electron. Lett. Comput. Vis. Image Anal. 2022, 21, 130–142. [Google Scholar] [CrossRef]
- Bishnoi, V.; Goel, N.; Tayal, A. Automated system-based classification of lung cancer using machine learning. Int. J. Med. Eng. Inform. 2023, 15, 403–415. [Google Scholar] [CrossRef]
- Damayanti, N.P.; Ananda, M.N.D.; Nugraha, F.W. Lung cancer classification using convolutional neural network and DenseNet. J. Soft Comput. Explor. 2023, 4, 133–141. [Google Scholar] [CrossRef]
- Vaiyapuri, T.; Liyakathunisa; Alaskar, H.; Parvathi, R.; Pattabiraman, V.; Hussain, A. Cat swarm optimization-based computer-aided diagnosis model for lung cancer classification in computed tomography images. Appl. Sci. 2022, 12, 5491. [Google Scholar] [CrossRef]
- Yadlapalli, P.; Bhavana, D.; Gunnam, S. Intelligent classification of lung malignancies using deep learning techniques. Int. J. Intell. Comput. Cybern. 2022, 15, 345–362. [Google Scholar] [CrossRef]
- Guo, Z.; Yang, J.; Zhao, L.; Yuan, J.; Yu, H. 3D SAACNet with GBM for the classification of benign and malignant lung nodules. Comput. Biol. Med. 2023, 153, 106532. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Liang, C.; Li, Y.; Shi, X.; Zhang, J.; Huang, H. Self-supervised transfer learning framework driven by visual attention for benign–malignant lung nodule classification on chest CT. Expert Syst. Appl. 2023, 215, 119339. [Google Scholar] [CrossRef]
- Qiao, J.; Fan, Y.; Zhang, M.; Fang, K.; Li, D.; Wang, Z. Ensemble framework based on attributes and deep features for benign-malignant classification of lung nodule. Biomed. Signal Process. Control. 2023, 79, 104217. [Google Scholar] [CrossRef]
- Ojala, T.; Pietikainen, M.; Maenpaa, T. Multiresolution gray-scale and rotation invariant texture classification with local binary patterns. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 971–987. [Google Scholar] [CrossRef]
- Olson, E. Particle shape factors and their use in image analysis part 1: Theory. J. Gxp Compliance 2011, 15, 85. [Google Scholar]
- Armato III, S.G.; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; Meyer, C.R.; Reeves, A.P.; Zhao, B.; Aberle, D.R.; Henschke, C.I.; Hoffman, E.A.; et al. The lung image database consortium (LIDC) and image database resource initiative (IDRI): A completed reference database of lung nodules on CT scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Shaffie, A.; Soliman, A.; Khalifeh, H.A.; Ghazal, M.; Taher, F.; Keynton, R.; Elmaghraby, A.; El-Baz, A. On the integration of ct-derived features for accurate detection of lung cancer. In Proceedings of the 2018 IEEE International Symposium on Signal Processing and Information Technology (ISSPIT), Louisville, KY, USA, 6–8 December 2018; pp. 435–440. [Google Scholar]
- Shaffie, A.; Soliman, A.; Khalifeh, H.A.; Taher, F.; Ghazal, M.; Dunlap, N.; Elmaghraby, A.; Keynton, R.; El-Baz, A. A novel ct-based descriptors for precise diagnosis of pulmonary nodules. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019; pp. 1400–1404. [Google Scholar]
- Alksas, A.; Shaffie, A.; Ghazal, M.; Taher, F.; Khelifi, A.; Yaghi, M.; Soliman, A.; Bogaert, E.V.; El-Baz, A. A novel higher order appearance texture analysis to diagnose lung cancer based on a modified local ternary pattern. Comput. Methods Programs Biomed. 2023, 240, 107692. [Google Scholar] [CrossRef] [PubMed]
- Bhende, M.; Thakare, A.; Saravanan, V.; Anbazhagan, K.; Patel, H.N.; Kumar, A. Attention layer-based multidimensional feature extraction for diagnosis of lung cancer. BioMed Res. Int. 2022, 2022, 3947434. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Li, B.; Liao, R.; Mo, H.; Tian, L. An ISHAP-based interpretation-model-guided classification method for malignant pulmonary nodule. Knowl.-Based Syst. 2022, 237, 107778. [Google Scholar] [CrossRef]
- Jiang, H.; Shen, F.; Gao, F.; Han, W. Learning efficient, explainable and discriminative representations for pulmonary nodules classification. Pattern Recognit. 2021, 113, 107825. [Google Scholar] [CrossRef]
- Zheng, B.; Yang, D.; Zhu, Y.; Liu, Y.; Hu, J.; Bai, C. 3D gray density coding feature for benign-malignant pulmonary nodule classification on chest CT. Med. Phys. 2021, 48, 7826–7836. [Google Scholar] [CrossRef] [PubMed]
- Saied, M.; Raafat, M.; Yehia, S.; Khalil, M.M. Efficient pulmonary nodules classification using radiomics and different artificial intelligence strategies. Insights Imaging 2023, 14, 91. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Direction | |||
|---|---|---|---|
| 1 | ✓ | ✓ | ✓ |
| 2 | ✓ | ✓ | ✗ |
| 3 | ✓ | ✗ | ✓ |
| 4 | ✓ | ✗ | ✗ |
| 5 | ✗ | ✓ | ✓ |
| 6 | ✗ | ✓ | ✗ |
| 7 | ✗ | ✗ | ✓ |
| 8 | ✗ | ✗ | ✗ |
| Layer | Output Shape |
|---|---|
| Input | (1, 64, 64, 64) |
| Conv1 | (64, 64, 64, 64) |
| ReLU1 | (64, 64, 64, 64) |
| MaxPool1 | (64, 32, 32, 32) |
| Conv2 | (128, 32, 32, 32) |
| ReLU2 | (128, 32, 32, 32) |
| MaxPool2 | (128, 16, 16, 16) |
| Conv3 | (256, 16, 16, 16) |
| ReLU3 | (256, 16, 16, 16) |
| MaxPool3 | (256, 8, 8, 8) |
| Flatten | (256 × 8 × 8 × 8) |
| Fully connected 1 | (512,) |
| ReLu4 | (512,) |
| Fully connected 2 | 2 |
| Evaluation Metrics | |||
|---|---|---|---|
| Accuracy | Sensitivity | Specificity | |
| Original 3D-LBP | 89.33 | 92.43 | 83.56 |
| Adjustable 3D-LBP [22] | 91.74 | 94.62 | 89.60 |
| Resolved Ambiguity 3D-LBP [23] | 92.20 | 90.32 | 93.60 |
| 3D-LTP [24] | 92.19 | 93.33 | 91.21 |
| Proposed 3D-LOP | 96.23 | 97.55 | 93.71 |
| Evaluation Metrics | ||||
|---|---|---|---|---|
| Accuracy | Sensitivity | Specificity | AUC | |
| 3D-LOP | 96.23 | 97.55 | 93.71 | 0.9894 |
| 3D-CNN | 93.52 | 95.57 | 89.89 | 0.9697 |
| Fusion | 97.84 | 98.11 | 94.73 | 0.9912 |
| Bhende, et al. [25] | 92.70 | 90.90 | 94.50 | - |
| He, et al. [26] | 87.30 | 86.20 | 88.50 | 0.873 |
| Jiang, et al. [27] | 90.77 | 85.37 | 95.04 | - |
| Alksas, et al. [24] | 96.17 | 97.14 | 95.33 | 0.9832 |
| Zheng, et al. [28] | 93.17 | 90.38 | - | 0.9753 |
| Saied, et al. [29] | 90.39 | 90.32 | 93.65 | 0.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Safta, W.; Shaffie, A. Advancing Pulmonary Nodule Diagnosis by Integrating Engineered and Deep Features Extracted from CT Scans. Algorithms 2024, 17, 161. https://doi.org/10.3390/a17040161
Safta W, Shaffie A. Advancing Pulmonary Nodule Diagnosis by Integrating Engineered and Deep Features Extracted from CT Scans. Algorithms. 2024; 17(4):161. https://doi.org/10.3390/a17040161
Chicago/Turabian StyleSafta, Wiem, and Ahmed Shaffie. 2024. "Advancing Pulmonary Nodule Diagnosis by Integrating Engineered and Deep Features Extracted from CT Scans" Algorithms 17, no. 4: 161. https://doi.org/10.3390/a17040161
APA StyleSafta, W., & Shaffie, A. (2024). Advancing Pulmonary Nodule Diagnosis by Integrating Engineered and Deep Features Extracted from CT Scans. Algorithms, 17(4), 161. https://doi.org/10.3390/a17040161