
Epidemiological Changes in Respiratory Viral Infections in Children: The Influence of the COVID-19 Pandemic

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimen Selection
2.2. Specimen Testing
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Statement
3. Results
4. Discussion
- -
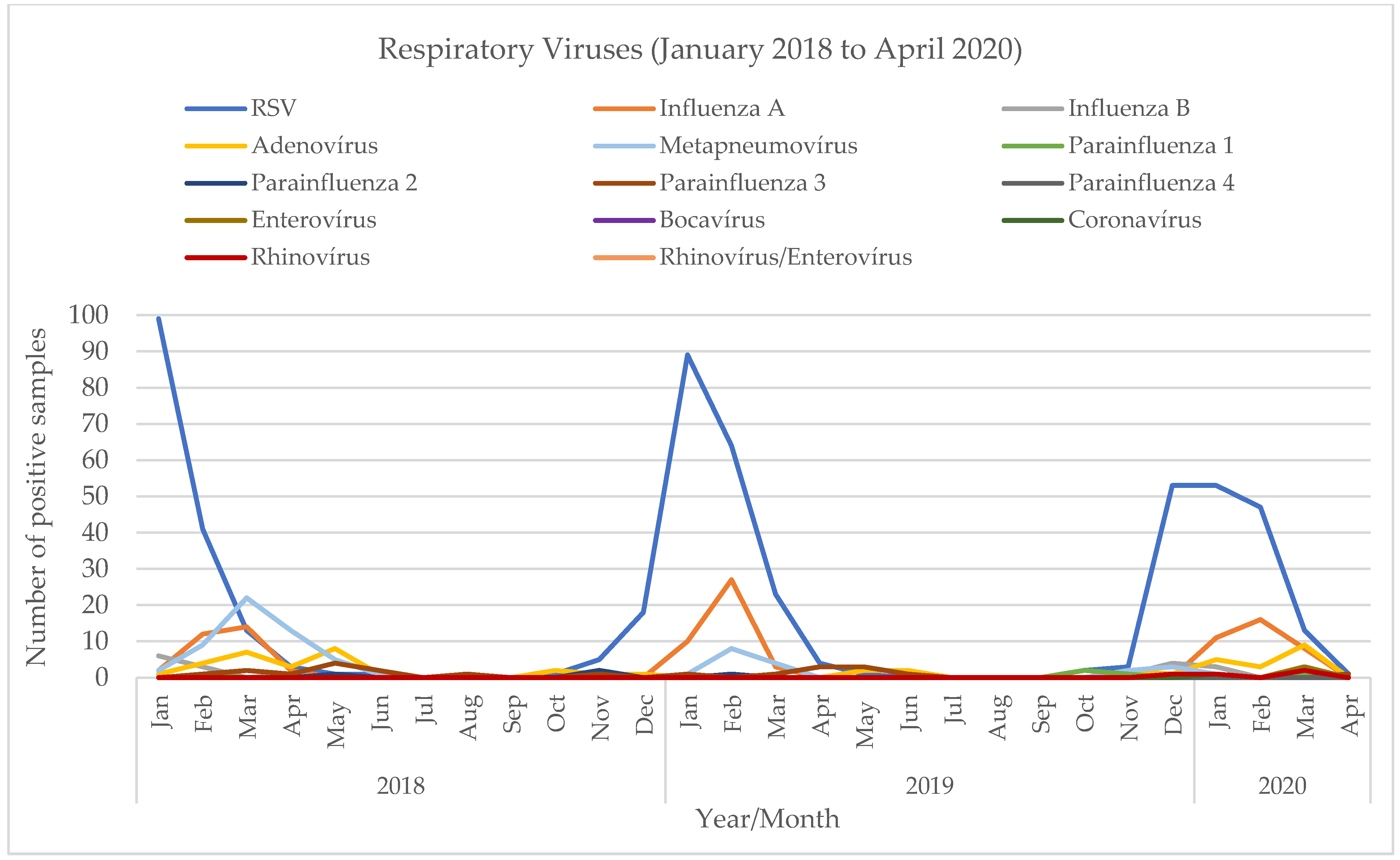
- Pre-pandemic: seasonality as described in the state of the art.
- -
- Post-pandemic:
- -
- Initial pandemic phase: disappearance of all non-SARS-CoV-2 respiratory viruses;
- -
- Evolution: detection of the first RSV cases in July 2021, reintroduction of non-SARS-CoV-2 viruses, starting with out-of-season outbreaks, and probable evolution towards the restauration of the usual epidemiological patterns.
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Mulholland, K. Global burden of acute respiratory infections in children: Implications for interventions. Pediatr. Pulmonol. 2003, 36, 469–474. [Google Scholar] [CrossRef]
- Calvo, C.; Garcia, M.; Casas, I.; Perez Breña, P. Infecciones respiratorias virales. In Protocolos Diagnóstico-Terapéuticos de la AEP: Infectología Pediátrica; AEP: Columbus, OH, USA, 2011; pp. 189–204. (In Spanish) [Google Scholar]
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of Respiratory Viral Infections. Annu. Rev. Virol. 2020, 7, 83–101. [Google Scholar] [CrossRef]
- Iannarella, R.; Lattanzi, C.; Cannata, G.; Argentiero, A.; Neglia, C.; Fainardi, V.; Pisi, G.; Esposito, S. Coronavirus infections in children: From SARS and MERS to COVID-19, a narrative review of epidemiological and clinical features. Acta Biomed. 2020, 91, e2020032. [Google Scholar] [PubMed]
- Agha, R.; Avner, J.R. Delayed Seasonal RSV Surge Observed During the COVID-19 Pandemic. Pediatrics 2021, 148, e2021052089. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, ciaa1906. [Google Scholar] [CrossRef] [PubMed]
- van Summeren, J.; Meijer, A.; Aspelund, G.; Casalegno, J.S.; Erna, G.; Hoang, U.; Lina, B.; de Lusignan, S.; Teirlinck, A.C.; VRS Study Group in Lyon; et al. Low levels of respiratory syncytial virus activity in Europe during the 2020/21 season: What can we expect in the coming summer and autumn/winter? Eurosurveillance 2021, 26, 1560–7917. [Google Scholar] [CrossRef] [PubMed]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; Van Herendael, B.; et al. Bronchiolitis in COVID-19 times: A nearly absent disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Casalegno, J.S.; Ploin, D.; Cantais, A.; Masson, E.; Bard, E.; Valette, M.; Fanget, R.; Targe, S.C.; Myar-Dury, A.F.; VRS Study Group in Lyon; et al. Characteristics of the delayed respiratory syncytial virus epidemic, 2020/2021, Rhône Loire, France. Eurosurveillance 2021, 26, 1560–7917. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, D.K.; Foley, D.A.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Blyth, C.C.; Moore, H.C. Impact of coronavirus disease 2019 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin. Infect. Dis. 2021, 72, 2199–2202. [Google Scholar] [CrossRef] [PubMed]
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Weinberger Opek, M.; Yeshayahu, Y.; Glatman-Freedman, A.; Kaufman, Z.; Sorek, N.; Brosh-Nissimov, T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. Eurosurveillance 2021, 26, 2017–2021. [Google Scholar] [CrossRef] [PubMed]
- Delestrain, C.; Danis, K.; Hau, I.; Behillil, S.; Billard, M.N.; Krajten, L.; Cohen, R.; Bont, L.; Epaud, R. Impact of COVID-19 social distancing on viral infection in France: A delayed outbreak of RSV. Pediatr. Pulmonol. 2021, 56, 3669–3673. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, L.; Deng, X.; Liang, R.; Su, M.; He, C.; Hu, L.; Su, Y.; Ren, J.; Yu, F.; et al. Recent advances in the detection of respiratory virus infection in humans. J. Med. Virol. 2020, 92, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Cepheid. Xpert® Xpress Flu/RSV. Available online: https://www.cepheid.com/pt/tests/Critical-Infectious-Diseases/Xpert-Xpress-Flu-RSV (accessed on 20 December 2021).
- Roche Diagnostics. Cobas® Influenza A/B & RSV UC Test. Available online: https://diagnostics.roche.com/global/en/products/params/Cobas-influenza-a-b-rsv-uc-test.html (accessed on 20 December 2021).
- BioFire Diagnostics. The BioFire® Respiratory 2.1 (RP2.1) Panel. Available online: https://www.biofiredx.com/products/the-filmarray-panels/filmarrayrp/ (accessed on 20 December 2021).
- Seegene. Allplex™ Respiratory Panel Assays. Available online: https://www.seegene.com/assays/allplex_respiratory_panel_assays (accessed on 20 December 2021).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, T.; Guimarães, J.T.; Rebelo, S. Epidemiological Changes in Respiratory Viral Infections in Children: The Influence of the COVID-19 Pandemic. Viruses 2023, 15, 1880. https://doi.org/10.3390/v15091880
Almeida T, Guimarães JT, Rebelo S. Epidemiological Changes in Respiratory Viral Infections in Children: The Influence of the COVID-19 Pandemic. Viruses. 2023; 15(9):1880. https://doi.org/10.3390/v15091880
Chicago/Turabian StyleAlmeida, Teresa, João Tiago Guimarães, and Sandra Rebelo. 2023. "Epidemiological Changes in Respiratory Viral Infections in Children: The Influence of the COVID-19 Pandemic" Viruses 15, no. 9: 1880. https://doi.org/10.3390/v15091880
APA StyleAlmeida, T., Guimarães, J. T., & Rebelo, S. (2023). Epidemiological Changes in Respiratory Viral Infections in Children: The Influence of the COVID-19 Pandemic. Viruses, 15(9), 1880. https://doi.org/10.3390/v15091880