
Nonlinear and Multidelayed Effects of Meteorological Drivers on Human Respiratory Syncytial Virus Infection in Japan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design Setting
2.2. Empirical Datasets
2.2.1. National HRSV Surveillance Data
2.2.2. Meteorological Data
2.3. Statistical Analysis
2.3.1. Descriptive Statistics
2.3.2. Construction of the Time-Series Statistical Model
2.4. Ethical Considerations
3. Results
3.1. Descriptive Analysis
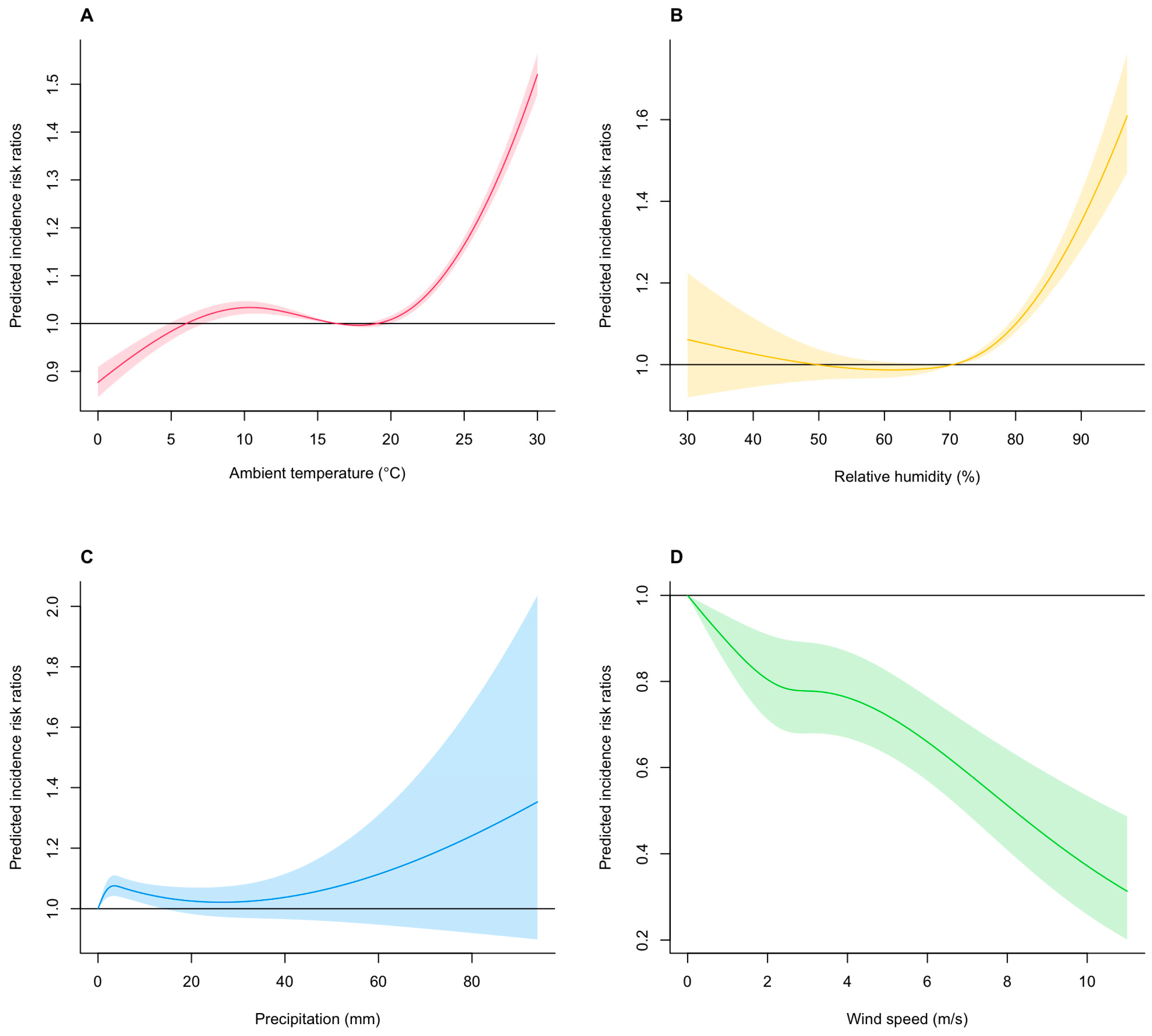
3.2. Assessing the Nonlinear Effects of Meteorological Drivers on HRSV Infection Incidence
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piedimonte, G.; Perez, M.K. Respiratory syncytial virus infection and bronchiolitis. Pediatr. Rev. 2014, 35, 519–530. [Google Scholar] [CrossRef]
- Nair, H.; Nokes, D.J.; Gessner, B.D.; Dherani, M.; Madhi, S.A.; Singleton, R.J.; O’Brien, K.L.; Roca, A.; Wright, P.F.; Bruce, N.; et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: A systematic review and meta-analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef] [PubMed]
- Hirve, S.; Crawford, N.; Palekar, R.; Zhang, W. Clinical characteristics, predictors, and performance of case definition-Interim results from the WHO global respiratory syncytial virus surveillance pilot. Influenza Other Respir. Viruses 2020, 14, 647–657. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Deloria-Knoll, M.; Madhi, S.A.; Cohen, C.; Ali, A.; Basnet, S.; Bassat, Q.; Brooks, W.A.; Chittaganpitch, M.; et al. Global burden of acute lower respiratory infection associated with human metapneumovirus in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Health 2021, 9, e33–e43. [Google Scholar] [CrossRef]
- Mazur, N.I.; Higgins, D.; Nunes, M.C.; Melero, J.A.; Langedijk, A.C.; Horsley, N.; Buchholz, U.J.; Openshaw, P.J.; McLellan, J.S.; Englund, J.A.; et al. The respiratory syncytial virus vaccine landscape: Lessons from the graveyard and promising candidates. Lancet Infect. Dis. 2018, 18, e295–e311. [Google Scholar] [CrossRef]
- Miyama, T.; Iritani, N.; Nishio, T.; Ukai, T.; Satsuki, Y.; Miyata, H.; Shintani, A.; Hiroi, S.; Motomura, K.; Kobayashi, K. Seasonal shift in epidemics of respiratory syncytial virus infection in Japan. Epidemiol. Infect. 2021, 149, e55. [Google Scholar] [CrossRef]
- Yamagami, H.; Kimura, H.; Hashimoto, T.; Kusakawa, I.; Kusuda, S. Detection of the Onset of the Epidemic Period of Respiratory Syncytial Virus Infection in Japan. Front. Public Health 2019, 7, 39. [Google Scholar] [CrossRef]
- Wagatsuma, K.; Koolhof, I.S.; Shobugawa, Y.; Saito, R. Shifts in the epidemic season of human respiratory syncytial virus associated with inbound overseas travelers and meteorological conditions in Japan, 2014–2017: An ecological study. PLoS ONE 2021, 16, e0248932. [Google Scholar] [CrossRef]
- Shobugawa, Y.; Takeuchi, T.; Hibino, A.; Hassan, M.R.; Yagami, R.; Kondo, H.; Odagiri, T.; Saito, R. Occurrence of human respiratory syncytial virus in summer in Japan. Epidemiol. Infect. 2017, 145, 272–284. [Google Scholar] [CrossRef]
- Broberg, E.K.; Waris, M.; Johansen, K.; Snacken, R.; Penttinen, P. Seasonality and geographical spread of respiratory syncytial virus epidemics in 15 European countries, 2010 to 2016. Eurosurveillance 2018, 23, 17-00284. [Google Scholar] [CrossRef]
- Wagatsuma, K.; Koolhof, I.S.; Shobugawa, Y.; Saito, R. Decreased human respiratory syncytial virus activity during the COVID-19 pandemic in Japan: An ecological time-series analysis. BMC Infect. Dis. 2021, 21, 734. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- Florin, T.A.; Plint, A.C.; Zorc, J.J. Viral bronchiolitis. Lancet 2017, 389, 211–224. [Google Scholar] [CrossRef]
- Sloan, C.; Moore, M.L.; Hartert, T. Impact of pollution, climate, and sociodemographic factors on spatiotemporal dynamics of seasonal respiratory viruses. Clin. Transl. Sci. 2011, 4, 48–54. [Google Scholar] [CrossRef]
- Tang, J.W.; Loh, T.P. Correlations between climate factors and incidence--a contributor to RSV seasonality. Rev. Med. Virol. 2014, 24, 15–34. [Google Scholar] [CrossRef]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodríguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejías, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory Syncytial Virus Seasonality: A Global Overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Broberg, E.K.; Campbell, H.; Nair, H. Seasonality of respiratory syncytial virus and its association with meteorological factors in 13 European countries, week 40 2010 to week 39 2019. Eurosurveillance 2022, 27, 2100619. [Google Scholar] [CrossRef]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P.; et al. Respiratory syncytial virus bronchiolitis, weather conditions and air pollution in an Italian urban area: An observational study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef]
- Baker, R.E.; Mahmud, A.S.; Wagner, C.E.; Yang, W.; Pitzer, V.E.; Viboud, C.; Vecchi, G.A.; Metcalf, C.J.E.; Grenfell, B.T. Epidemic dynamics of respiratory syncytial virus in current and future climates. Nat. Commun. 2019, 10, 5512. [Google Scholar] [CrossRef]
- Pitzer, V.E.; Viboud, C.; Alonso, W.J.; Wilcox, T.; Metcalf, C.J.; Steiner, C.A.; Haynes, A.K.; Grenfell, B.T. Environmental drivers of the spatiotemporal dynamics of respiratory syncytial virus in the United States. PLoS Pathog. 2015, 11, e1004591. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Liu, C.; Xiao, Y.; Xiang, Z.; Zhou, H.; Chen, L.; Shen, K.; Xie, Z.; Ren, L.; Wang, J. Respiratory Syncytial Virus Seasonality, Beijing, China, 2007–2015. Emerg. Infect. Dis. 2019, 25, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wen, S.; Zheng, J.; Chen, X.; Lv, F.; Liu, L. Meteorological factors affecting respiratory syncytial virus infection: A time-series analysis. Pediatr. Pulmonol. 2020, 55, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Fu, J.F.; Mao, J.H.; Shang, S.Q. Haze is a risk factor contributing to the rapid spread of respiratory syncytial virus in children. Environ. Sci. Pollut. Res. Int. 2016, 23, 20178–20185. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wang, J.; Li, Z.; Xu, C.; Liao, Y.; Hu, M.; Yang, J.; Lai, S.; Wang, L.; Yang, W. Seasonal association between viral causes of hospitalised acute lower respiratory infections and meteorological factors in China: A retrospective study. Lancet Planet. Health 2021, 5, e154–e163. [Google Scholar] [CrossRef]
- Lapeña, S.; Robles, M.B.; Castañón, L.; Martínez, J.P.; Reguero, S.; Alonso, M.P.; Fernández, I. Climatic factors and lower respiratory tract infection due to respiratory syncytial virus in hospitalised infants in northern Spain. Eur. J. Epidemiol. 2005, 20, 271–276. [Google Scholar] [CrossRef]
- Tang, J.W.; Lai, F.Y.; Wong, F.; Hon, K.L. Incidence of common respiratory viral infections related to climate factors in hospitalized children in Hong Kong. Epidemiol. Infect. 2010, 138, 226–235. [Google Scholar] [CrossRef]
- Fall, A.; Dia, N.; Cisse, E.H.A.; Kiori, D.E.; Sarr, F.D.; Sy, S.; Goudiaby, D.; Richard, V.; Niang, M.N. Epidemiology and Molecular Characterization of Human Respiratory Syncytial Virus in Senegal after Four Consecutive Years of Surveillance, 2012–2015. PLoS ONE 2016, 11, e0157163. [Google Scholar] [CrossRef]
- Rodriguez-Martinez, C.E.; Sossa-Briceño, M.P.; Acuña-Cordero, R. Relationship between meteorological conditions and respiratory syncytial virus in a tropical country. Epidemiol. Infect. 2015, 143, 2679–2686. [Google Scholar] [CrossRef]
- Djelantik, I.G.; Gessner, B.D.; Soewignjo, S.; Steinhoff, M.; Sutanto, A.; Widjaya, A.; Linehan, M.; Moniaga, V. Incidence and clinical features of hospitalization because of respiratory syncytial virus lower respiratory illness among children less than two years of age in a rural Asian setting. Pediatr. Infect. Dis. J. 2003, 22, 150–157. [Google Scholar] [CrossRef]
- Chan, P.K.; Sung, R.Y.; Fung, K.S.; Hui, M.; Chik, K.W.; Adeyemi-Doro, F.A.; Cheng, A.F. Epidemiology of respiratory syncytial virus infection among paediatric patients in Hong Kong: Seasonality and disease impact. Epidemiol. Infect. 1999, 123, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Sutanto, A.; Sarwo, H.; Linehan, M.; Djelantik, I.G.; Mercer, D.; Moniaga, V.; Moulton, L.H.; Widjaya, A.; Muljati, P.; et al. Climatic, temporal, and geographic characteristics of respiratory syncytial virus disease in a tropical island population. Epidemiol. Infect. 2008, 136, 1319–1327. [Google Scholar] [CrossRef]
- Nyoka, R.; Omony, J.; Mwalili, S.M.; Achia, T.N.O.; Gichangi, A.; Mwambi, H. Effect of climate on incidence of respiratory syncytial virus infections in a refugee camp in Kenya: A non-Gaussian time-series analysis. PLoS ONE 2017, 12, e0178323. [Google Scholar] [CrossRef]
- Nottmeyer, L.; Armstrong, B.; Lowe, R.; Abbott, S.; Meakin, S.; O’Reilly, K.; von Borries, R.; Schneider, R.; Royé, D.; Hashizume, M.; et al. The association of COVID-19 incidence with temperature, humidity, and UV radiation—A global multi-city analysis. Sci. Total. Environ. 2022, 854, 158636. [Google Scholar] [CrossRef]
- Weaver, A.K.; Head, J.R.; Gould, C.F.; Carlton, E.J.; Remais, J.V. Environmental Factors Influencing COVID-19 Incidence and Severity. Annu. Rev. Public Health 2022, 43, 271–291. [Google Scholar] [CrossRef]
- Villeneuve, P.J.; Goldberg, M.S. Methodological Considerations for Epidemiological Studies of Air Pollution and the SARS and COVID-19 Coronavirus Outbreaks. Environ. Health Perspect. 2020, 128, 95001. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Dubrow, R. Climate change: An enduring challenge for vector-borne disease prevention and control. Nat. Immunol. 2020, 21, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, P.; Tozan, Y.; Overgaard, H.J.; Aravinda Tissera, H.; Rocklöv, J. Effect of El Niño-Southern Oscillation and local weather on Aedes dvector activity from 2010 to 2018 in Kalutara district, Sri Lanka: A two-stage hierarchical analysis. Lancet Planet. Health 2022, 6, e577–e585. [Google Scholar] [CrossRef]
- Chen, Y.; Li, N.; Lourenço, J.; Wang, L.; Cazelles, B.; Dong, L.; Li, B.; Liu, Y.; Jit, M.; Bosse, N.I.; et al. Measuring the effects of COVID-19-related disruption on dengue transmission in southeast Asia and Latin America: A statistical modelling study. Lancet Infect. Dis. 2022, 22, 657–667. [Google Scholar] [CrossRef]
- Kim, Y.; Ratnam, J.V.; Doi, T.; Morioka, Y.; Behera, S.; Tsuzuki, A.; Minakawa, N.; Sweijd, N.; Kruger, P.; Maharaj, R.; et al. Malaria predictions based on seasonal climate forecasts in South Africa: A time series distributed lag nonlinear model. Sci. Rep. 2019, 9, 17882. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Park, J.W.; Cheong, H.K. Estimated effect of climatic variables on the transmission of Plasmodium vivax malaria in the Republic of Korea. Environ. Health Perspect. 2012, 120, 1314–1319. [Google Scholar] [CrossRef]
- Moirano, G.; Gasparrini, A.; Acquaotta, F.; Fratianni, S.; Merletti, F.; Maule, M.; Richiardi, L. West Nile Virus infection in Northern Italy: Case-crossover study on the short-term effect of climatic parameters. Environ. Res. 2018, 167, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.; Aik, J. The abundance of Culex mosquito vectors for West Nile Virus and other flaviviruses: A time-series analysis of rainfall and temperature dependence in Singapore. Sci. Total Environ. 2021, 754, 142420. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases, Japan (NIID). National Epidemiological Surveillance of Infectious Diseases (NESID) Infectious Diseases Weekly Report (IDWR). Available online: https://www.niid.go.jp/niid/ja/idwr.html (accessed on 1 February 2023).
- Hibino, A.; Saito, R.; Taniguchi, K.; Zaraket, H.; Shobugawa, Y.; Matsui, T.; Suzuki, H. Molecular epidemiology of human respiratory syncytial virus among children in Japan during three seasons and hospitalization risk of genotype ON1. PLoS ONE 2018, 13, e0192085. [Google Scholar] [CrossRef]
- Zaraket, H.; Saito, R. Japanese Surveillance Systems and Treatment for Influenza. Curr. Treat. Options Infect. Dis. 2016, 8, 311–328. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare, Japan (MHLW). Notification of Physicians and Veterinarians Based on the Infectious Diseases Law (Human Respiratory Syncytial Virus). Available online: http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou11/01-05-15.html (accessed on 1 February 2023).
- Japan Meteorological Agency. Meteorological Data Search. Available online: https://www.data.jma.go.jp/obd/stats/etrn/index.php (accessed on 19 July 2023).
- Lee, M.H.; Mailepessov, D.; Yahya, K.; Loo, L.H.; Maiwald, M.; Aik, J. Air quality, meteorological variability and pediatric respiratory syncytial virus infections in Singapore. Sci. Rep. 2023, 13, 1001. [Google Scholar] [CrossRef]
- Ali, S.T.; Tam, C.C.; Cowling, B.J.; Yeo, K.T.; Yung, C.F. Meteorological drivers of respiratory syncytial virus infections in Singapore. Sci. Rep. 2020, 10, 20469. [Google Scholar] [CrossRef]
- Thongpan, I.; Vongpunsawad, S.; Poovorawan, Y. Respiratory syncytial virus infection trend is associated with meteorological factors. Sci. Rep. 2020, 10, 10931. [Google Scholar] [CrossRef]
- Wagatsuma, K.; Koolhof, I.S.; Saito, R. The Relative Roles of Ambient Temperature and Mobility Patterns in Shaping the Transmission Heterogeneity of SARS-CoV-2 in Japan. Viruses 2022, 14, 2232. [Google Scholar] [CrossRef]
- Wagatsuma, K.; Koolhof, I.S.; Saito, R. Was the Reduction in Seasonal Influenza Transmission during 2020 Attributable to Non-Pharmaceutical Interventions to Contain Coronavirus Disease 2019 (COVID-19) in Japan? Viruses 2022, 14, 1417. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. 2003 Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Gasparrini, A.; Masselot, P.; Scortichini, M.; Schneider, R.; Mistry, M.N.; Sera, F.; Macintyre, H.L.; Phalkey, R.; Vicedo-Cabrera, A.M. Small-area assessment of temperature-related mortality risks in England and Wales: A case time series analysis. Lancet Planet. Health 2022, 6, e557–e564. [Google Scholar] [CrossRef]
- Lessler, J.; Reich, N.G.; Brookmeyer, R.; Perl, T.M.; Nelson, K.E.; Cummings, D.A. Incubation periods of acute respiratory viral infections: A systematic review. Lancet Infect. Dis. 2009, 9, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Hashimoto, S.; Kawado, M.; Murakami, Y.; Izumida, M.; Ohta, A.; Tada, Y.; Shigematsu, M.; Yasui, Y.; Nagai, M. Overview of infectious disease surveillance system in Japan, 1999–2005. J. Epidemiol. 2007, 17, S3–S13. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef]
- Imai, C.; Hashizume, M. A systematic review of methodology: Time series regression analysis for environmental factors and infectious diseases. Trop. Med. Health 2015, 43, 1–9. [Google Scholar] [CrossRef]
- Imai, C.; Armstrong, B.; Chalabi, Z.; Mangtani, P.; Hashizume, M. Time series regression model for infectious disease and weather. Environ. Res. 2015, 142, 319–327. [Google Scholar] [CrossRef]
- Prefecture/City/Town/Village. Population Data. Available online: https://uub.jp/rnk/rnk.cgi?T=p&S=j&B=20201001 (accessed on 1 January 2023).
- Ma, Y.; Pei, S.; Shaman, J.; Dubrow, R.; Chen, K. Role of meteorological factors in the transmission of SARS-CoV-2 in the United States. Nat. Commun. 2021, 12, 3602. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar]
- Papi, A.; Ison, M.G.; Langley, J.M.; Lee, D.-G.; Leroux-Roels, I.; Martinon-Torres, F.; Schwarz, T.F.; van Zyl-Smit, R.N.; Campora, L.; Dezutter, N.; et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine in Older Adults. N. Engl. J. Med. 2023, 388, 595–608. [Google Scholar] [CrossRef]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe, J.E., Jr.; Cutland, C.L.; Eckert, L.; et al. Respiratory syncytial virus prevention within reach: The vaccine and monoclonal antibody landscape. Lancet Infect. Dis. 2023, 23, e2–e21. [Google Scholar] [CrossRef] [PubMed]
- Lopes, G.P.; Amorim, Í.P.S.; Melo, B.O.; Maramaldo, C.E.C.; Bomfim, M.R.Q.; Lima Neto, L.G.; Alves, M.S.; Silva, F.B.; Soeiro-Pereira, P.V.; Falcai, A. Identification and seasonality of rhinovirus and respiratory syncytial virus in asthmatic children in tropical climate. Biosci. Rep. 2020, 40, BSR20200634. [Google Scholar] [CrossRef]
- Polozov, I.V.; Bezrukov, L.; Gawrisch, K.; Zimmerberg, J. Progressive ordering with decreasing temperature of the phospholipids of influenza virus. Nat. Chem. Biol. 2008, 4, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Peiris, J.S.; Lam, S.Y.; Poon, L.L.; Yuen, K.Y.; Seto, W.H. The Effects of Temperature and Relative Humidity on the Viability of the SARS Coronavirus. Adv. Virol. 2011, 2011, 734690. [Google Scholar] [CrossRef] [PubMed]
- Shaman, J.; Kohn, M. Absolute humidity modulates influenza survival, transmission, and seasonality. Proc. Natl. Acad. Sci. USA 2009, 106, 3243–3248. [Google Scholar] [CrossRef]
- Lowen, A.C.; Mubareka, S.; Steel, J.; Palese, P. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog. 2007, 3, 1470–1476. [Google Scholar] [CrossRef]
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal variations in seasonal activity of influenza and respiratory syncytial virus (RSV): A global comparative review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef]
- Yusuf, S.; Piedimonte, G.; Auais, A.; Demmler, G.; Krishnan, S.; Van Caeseele, P.; Singleton, R.; Broor, S.; Parveen, S.; Avendano, L.; et al. The relationship of meteorological conditions to the epidemic activity of respiratory syncytial virus. Epidemiol. Infect. 2007, 135, 1077–1090. [Google Scholar] [CrossRef]
- Hall, C.B.; Douglas, R.G., Jr.; Geiman, J.M. Possible transmission by fomites of respiratory syncytial virus. J. Infect. Dis. 1980, 141, 98–102. [Google Scholar] [CrossRef]
- Vandini, S.; Corvaglia, L.; Alessandroni, R.; Aquilano, G.; Marsico, C.; Spinelli, M.; Lanari, M.; Faldella, G. Respiratory syncytial virus infection in infants and correlation with meteorological factors and air pollutants. Ital. J. Pediatr. 2013, 39, 1. [Google Scholar] [CrossRef]
- Paynter, S.; Yakob, L.; Simões, E.A.; Lucero, M.G.; Tallo, V.; Nohynek, H.; Ware, R.S.; Weinstein, P.; Williams, G.; Sly, P.D. Using mathematical transmission modelling to investigate drivers of respiratory syncytial virus seasonality in children in the Philippines. PLoS ONE 2014, 9, e90094. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M. How do low wind speeds and high levels of air pollution support the spread of COVID-19? Atmos. Pollut. Res. 2021, 12, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Wu, Y.; Jing, W.; Liu, J.; Du, M.; Wang, Y.; Liu, M. Association between meteorological factors and daily new cases of COVID-19 in 188 countries: A time series analysis. Sci. Total Environ. 2021, 780, 146538. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.L.; Klein, M.; Brondi, L.; McGowan, J.E., Jr.; van Mels, C.; Brooks, W.A.; Kleinbaum, D.; Goswami, D.; Ryan, P.B.; Bridges, C.B. Rainfall, household crowding, and acute respiratory infections in the tropics. Epidemiol. Infect. 2012, 140, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Dowell, S.F. Seasonality—Still confusing. Epidemiol. Infect. 2012, 140, 87–90. [Google Scholar] [CrossRef]
- Tang, J.W. The effect of environmental parameters on the survival of airborne infectious agents. J. R. Soc. Interface 2009, 6 (Suppl. S6), S737–S746. [Google Scholar] [CrossRef]
- Lei, H.; Yang, M.; Dong, Z.; Hu, K.; Chen, T.; Yang, L.; Zhang, N.; Duan, X.; Yang, S.; Wang, D.; et al. Indoor relative humidity shapes influenza seasonality in temperate and subtropical climates in China. Int. J. Infect. Dis. 2023, 126, 54–63. [Google Scholar] [CrossRef]
- Verheyen, C.A.; Bourouiba, L. Associations between indoor relative humidity and global COVID-19 outcomes. J. R. Soc. Interface 2022, 19, 20210865. [Google Scholar] [CrossRef]
- White, L.J.; Waris, M.; Cane, P.A.; Nokes, D.J.; Medley, G.F. The transmission dynamics of groups A and B human respiratory syncytial virus (hRSV) in England & Wales and Finland: Seasonality and cross-protection. Epidemiol. Infect. 2005, 133, 279–289. [Google Scholar] [CrossRef]
- Waris, M.; White, L.J. Seasonality of respiratory syncytial virus infection. Clin. Infect. Dis. 2006, 43, 541. [Google Scholar] [CrossRef] [PubMed]
- Paiva, T.M.; Ishida, M.A.; Benega, M.A.; Constantino, C.R.; Silva, D.B.; Santos, K.C.; Oliveira, M.I.; Barbosa, H.A.; Carvalhanas, T.R.; Schuck-Paim, C.; et al. Shift in the timing of respiratory syncytial virus circulation in a subtropical megalopolis: Implications for immunoprophylaxis. J. Med. Virol. 2012, 84, 1825–1830. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef]
- Casalegno, J.S.; Ploin, D.; Cantais, A.; Masson, E.; Bard, E.; Valette, M.; Fanget, R.; Targe, S.C.; Myar-Dury, A.F.; Doret-Dion, M.; et al. Characteristics of the delayed respiratory syncytial virus epidemic, 2020/2021, Rhône Loire, France. Eurosurveillance 2021, 26, 2100630. [Google Scholar] [CrossRef] [PubMed]
- Onozuka, D. The influence of diurnal temperature range on the incidence of respiratory syncytial virus in Japan. Epidemiol. Infect. 2015, 143, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Boogaard, I.; van Oosten, M.; van Rijt, L.S.; Muskens, F.; Kimman, T.G.; Lambrecht, B.N.; Buisman, A.M. Respiratory syncytial virus differentially activates murine myeloid and plasmacytoid dendritic cells. Immunology 2007, 122, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Paynter, S.; Weinstein, P.; Ware, R.S.; Lucero, M.G.; Tallo, V.; Nohynek, H.; Barnett, A.G.; Skelly, C.; Simões, E.A.; Sly, P.D.; et al. Sunshine, rainfall, humidity and child pneumonia in the tropics: Time-series analyses. Epidemiol. Infect. 2013, 141, 1328–1336. [Google Scholar] [CrossRef]
- Lowe, R.; Lee, S.A.; O’Reilly, K.M.; Brady, O.J.; Bastos, L.; Carrasco-Escobar, G.; de Castro Catão, R.; Colón-González, F.J.; Barcellos, C.; Carvalho, M.S.; et al. Combined effects of hydrometeorological hazards and urbanisation on dengue risk in Brazil: A spatiotemporal modelling study. Lancet Planet. Health 2021, 5, e209–e219. [Google Scholar] [CrossRef]
- Alesemi, M.; Shahrani, J.S.A.; Iqbal, N.; Shah, R.; Nonlaopon, K. Analysis and Numerical Simulation of System of Fractional Partial Differential Equations with Non-Singular Kernel Operators. Symmetry 2023, 15, 233. [Google Scholar] [CrossRef]
- Botmart, T.; Naeem, M.; Shah, R.; Iqbal, N. Fractional View Analysis of Emden-Fowler Equations with the Help of Analytical Method. Symmetry 2022, 14, 2168. [Google Scholar] [CrossRef]
- Yasmin, H.; Aljahdaly, N.H.; Saeed, A.M.; Shah, R. Investigating Families of Soliton Solutions for the Complex Structured Coupled Fractional Biswas–Arshed Model in Birefringent Fibers Using a Novel Analytical Technique. Fractal Fract. 2023, 7, 491. [Google Scholar] [CrossRef]
- Yasmin, H.; Aljahdaly, N.H.; Saeed, A.M.; Shah, R. Probing Families of Optical Soliton Solutions in Fractional Perturbed Radhakrishnan–Kundu–Lakshmanan Model with Improved Versions of Extended Direct Algebraic Method. Fractal Fract. 2023, 7, 512. [Google Scholar] [CrossRef]
- The Lancet Planetary Health. Modelling health futures. Lancet Planet. Health 2021, 5, e395. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Potential Drivers | Mean | SD | Min | P25 | P50 | P75 | Max |
|---|---|---|---|---|---|---|---|
| Weekly newly confirmed cases | 49 | 76 | 0 | 7 | 22 | 58 | 892 |
| Mean ambient temperature (°C) | 15.7 | 8.3 | –6.7 | 8.1 | 16.3 | 22.7 | 32.2 |
| Relative humidity (%) | 69.5 | 9.5 | 30.8 | 63.1 | 70.2 | 76.4 | 97.2 |
| Precipitation (mm) | 4.7 | 6.4 | 0.0 | 0.7 | 2.9 | 6.2 | 94.1 |
| Wind speed (m/s) | 2.9 | 0.9 | 0.9 | 2.2 | 2.8 | 3.4 | 11.3 |
| Potential Drivers | Lag (Weeks) | |||
|---|---|---|---|---|
| 0 | 1 | 2 | 0–2 | |
| IRR (95% CI) | IRR (95% CI) | IRR (95% CI) | IRR (95% CI) | |
| Mean ambient temperature (°C) | ||||
| 8.1 °C | 1.053 (1.015, 1.093) | 1.117 (1.070, 1.166) | 0.869 (0.837, 0.903) | 1.023 (1.008, 1.039) |
| 22.7 °C | 0.936 (0.910, 0.964) | 1.037 (1.001, 1.073) | 1.099 (1.067, 1.131) | 1.068 (1.056, 1.079) |
| Relative humidity (%) | ||||
| 63.1% | 0.998 (0.986, 1.011) | 0.979 (0.966, 0.991) | 1.009 (0.997, 1.022) | 0.997 (0.971, 1.003) |
| 76.4% | 1.007 (0.997, 1.017) | 1.039 (1.029, 1.050) | 0.998 (0.988, 1.008) | 1.045 (1.032, 1.059) |
| Precipitation (mm) | ||||
| 0.7 mm | 1.002 (0.995, 1.008) | 1.012 (1.005, 1.019) | 1.015 (1.005, 1.019) | 1.027 (1.015, 1.038) |
| 6.2 mm | 0.983 (0.964, 1.002) | 1.033 (1.014, 1.053) | 1.047 (1.027, 1.067) | 1.064 (1.032, 1.097) |
| Wind speed (m/s) | ||||
| 2.2 m/s | 0.972 (0.877, 1.078) | 0.887 (0.799, 0.985) | 0.919 (0.829, 1.019) | 0.793 (0.697, 0.903) |
| 3.4 m/s | 0.976 (0.875, 1.088) | 0.864 (0.774, 0.965) | 0.918 (0.824, 1.022) | 0.775 (0.678, 0.885) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagatsuma, K.; Koolhof, I.S.; Saito, R. Nonlinear and Multidelayed Effects of Meteorological Drivers on Human Respiratory Syncytial Virus Infection in Japan. Viruses 2023, 15, 1914. https://doi.org/10.3390/v15091914
Wagatsuma K, Koolhof IS, Saito R. Nonlinear and Multidelayed Effects of Meteorological Drivers on Human Respiratory Syncytial Virus Infection in Japan. Viruses. 2023; 15(9):1914. https://doi.org/10.3390/v15091914
Chicago/Turabian StyleWagatsuma, Keita, Iain S. Koolhof, and Reiko Saito. 2023. "Nonlinear and Multidelayed Effects of Meteorological Drivers on Human Respiratory Syncytial Virus Infection in Japan" Viruses 15, no. 9: 1914. https://doi.org/10.3390/v15091914