
Innovating on Inhaled Bioequivalence: A Critical Analysis of the Current Limitations, Potential Solutions and Stakeholders of the Process


 and
and
Abstract
1. Introduction
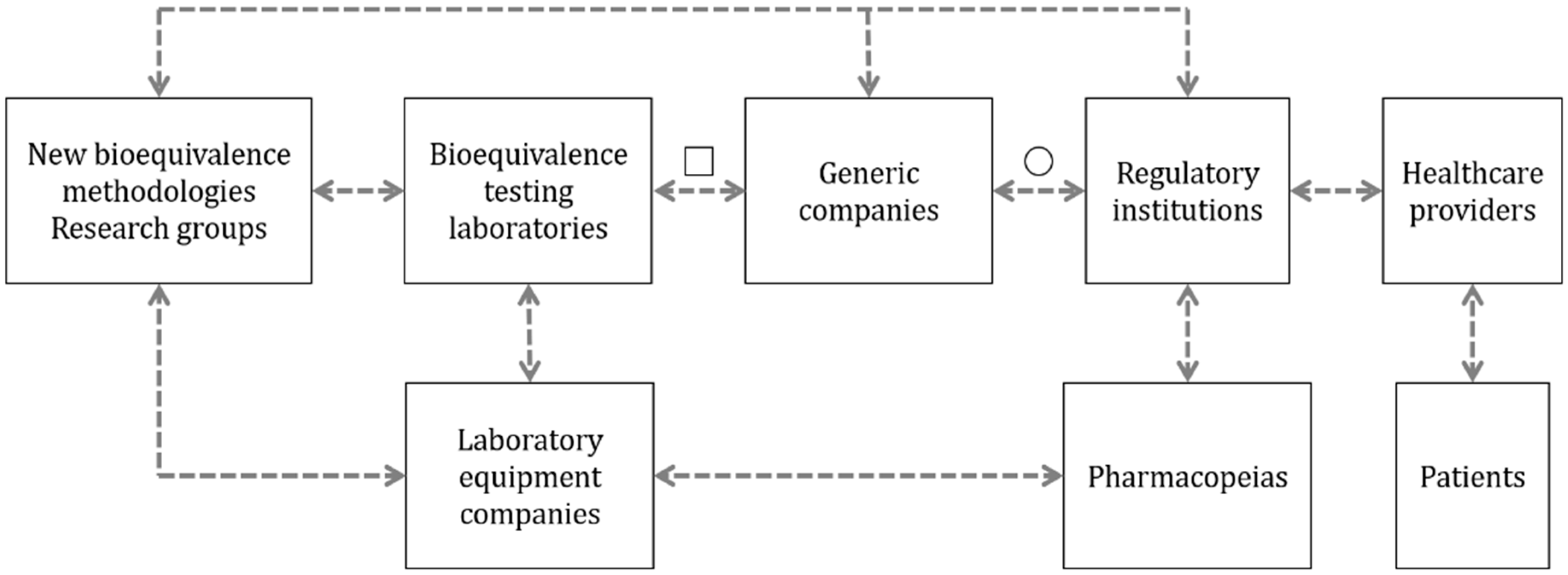
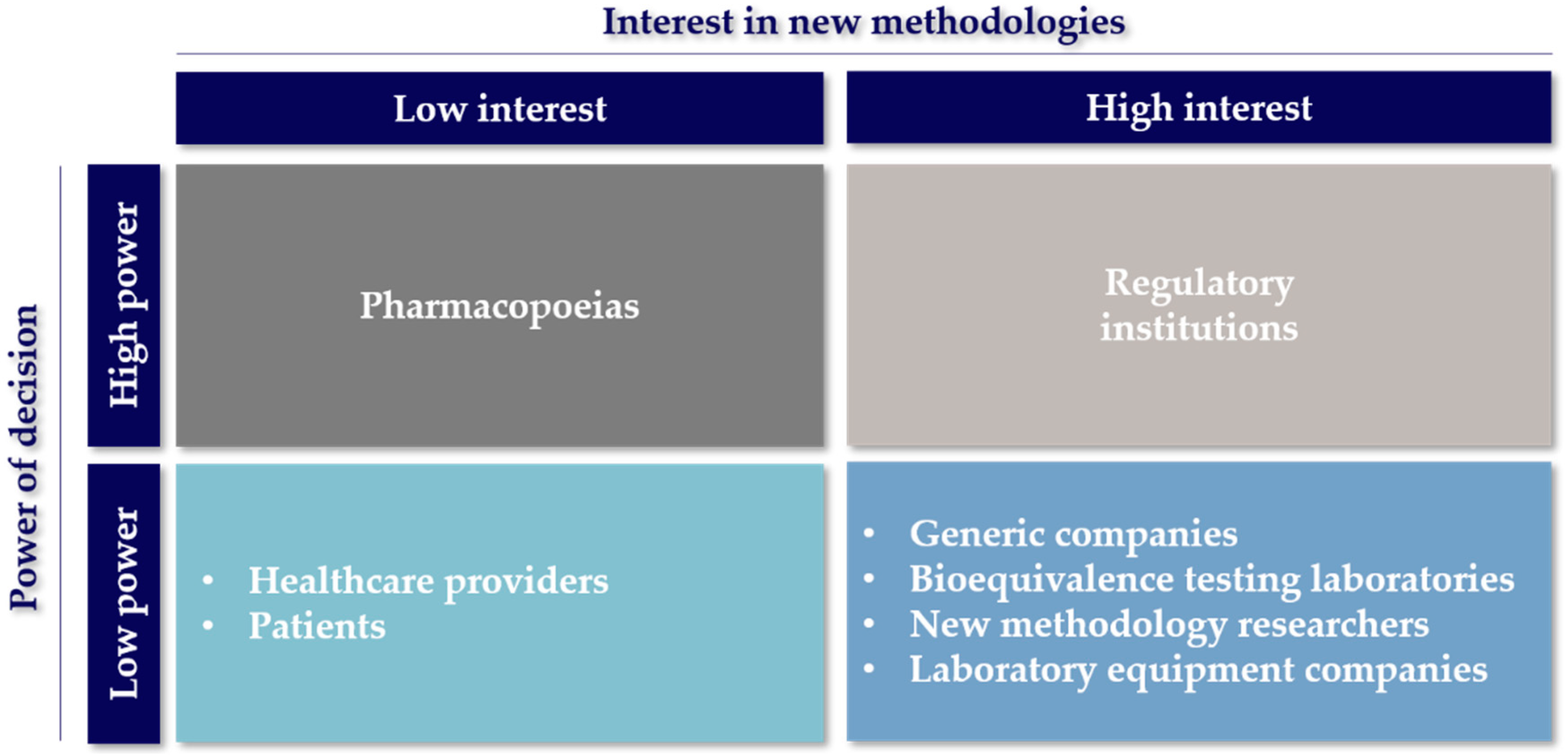
2. Relationships of the Stakeholders in the Inhaled Bioequivalence Research Field
2.1. Developers of New Bioequivalence Methodologies
2.2. Bioequivalence Testing Laboratories
2.3. Laboratory Equipment Companies
2.4. Generic Companies
2.5. Regulatory Agencies
2.6. Pharmacopoeias
2.7. Healthcare Providers
2.8. Patients
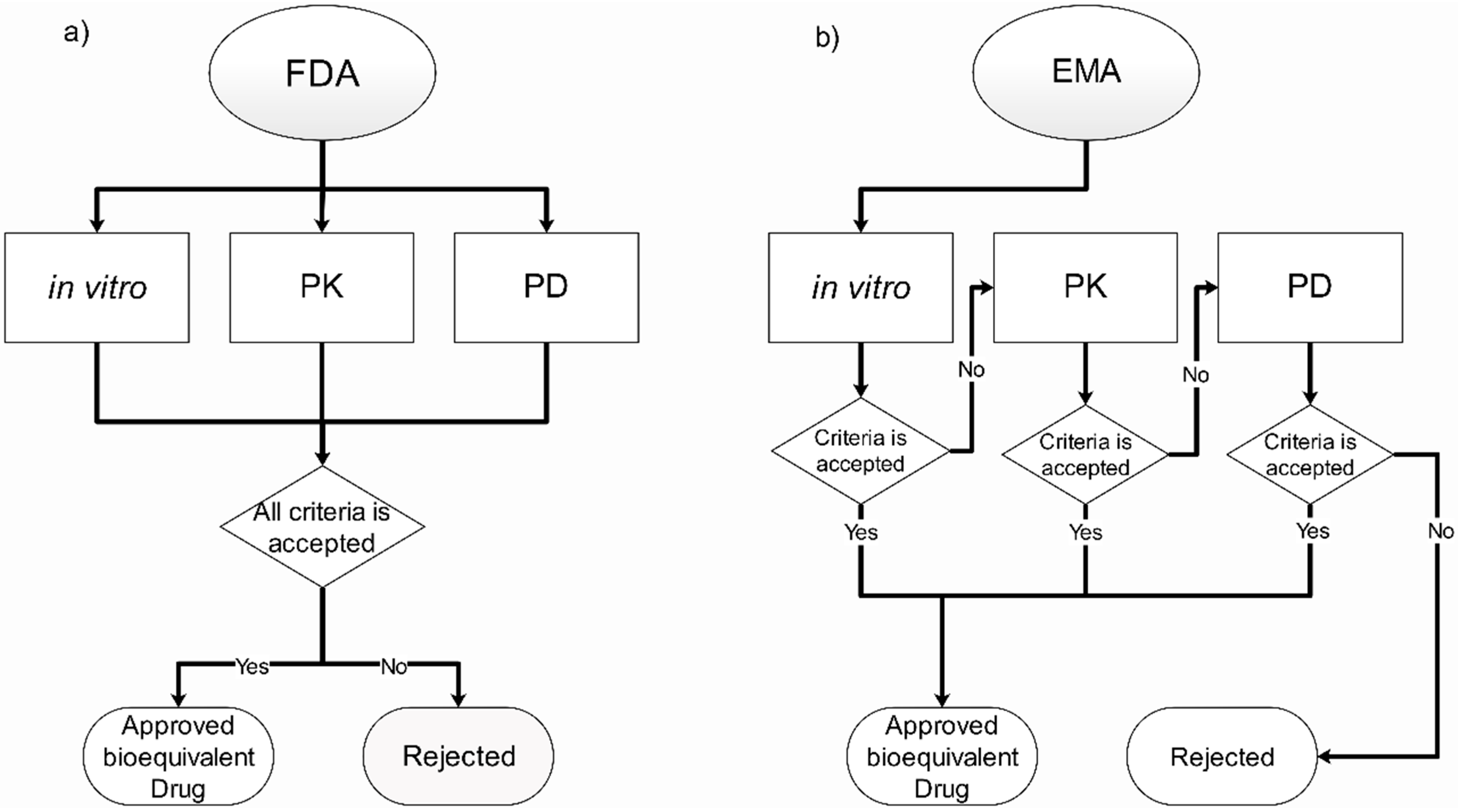
3. Current Regulation and Official Methodologies for Inhaled Bioequivalence
3.1. In Vitro Requirements
3.2. Pharmacokinetics Requirements
3.3. Pharmacodynamic Requirements
4. Alternative Methods for Bioequivalence
4.1. In Vitro Methods
4.1.1. Dissolution Test
4.1.2. Mouth-Throat Models
4.1.3. Mass-Based Plume Geometry
4.1.4. 3D-Printed Lung Models
4.2. In Vivo Methods
4.2.1. Imaging of Deposition Patterns
4.2.2. Exhaled Nitric Oxide (eNO)
4.2.3. Functional Respiratory Imaging (FRI)
4.3. In Silico Methods
4.3.1. Computational Fluid Dynamics (CFD)
4.3.2. Pharmacometrics
5. Future of Bioequivalence for Inhaled Drugs: Biopharmaceutical Classification System for Inhaled Medicines (iBCS)
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Chronic Respiratory Diseases: Asthma; World Health Organization: Geneva, Switzerland, 2020; p. 1. Available online: https://www.who.int/news-room/q-a-detail/chronic-respiratory-diseases-asthma (accessed on 14 July 2020).
- Ehrhardt, C. Inhalation Biopharmaceutics: Progress towards Comprehending the Fate of Inhaled Medicines. Pharm. Res. 2017, 34, 2451–2453. [Google Scholar] [CrossRef] [PubMed]
- Midha, K.K.; McKay, G. Editorial: Bioequivalence; its history, practice, and future. AAPS J. 2009, 11, 664–670. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Approved Prescription Drugs with Therapeutic Equivalence Evaluation (Orange Book). Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/approved-drug-products-therapeutic-equivalence-evaluations-orange-book (accessed on 14 July 2020).
- Newman, B.; Witzmann, K. Addressing the Regulatory and Scientific Challenges with Generic Orally Inhaled Drug Products. Pharmaceut. Med. 2020, 34, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Marple, V.A.; Hochrainer, D.; Roberts, D.L.; Romay, F.J.; Miller, N.C.; Truman, K.G.; Van Oort, M.; Olsson, B.; Holroyd, M.J.; Mitchell, J.P. Next Generation Pharmaceutical Impactor (a new impactor for pharmaceutical inhaler testing). Part I: Design. J. Aerosol Med. Depos. Clear. Eff. Lung 2003, 16, 283–299. [Google Scholar] [CrossRef]
- De Boer, H. Academia in the 21st Century: An Analysis of Trends and Perspectives in Higher Education and Research; Adviesraad voor het Wetenschaps-en Technologiebeleid, AWT: Den Haag, The Netherlands, 2002; ISBN 978-90-77005-12-5. [Google Scholar]
- National Institute of Healthh (NIH). Grant RFA-FD-21-020: Impulse Oscillometry Endpoint Sensitivity to Regional Lung Function Changes Using Computational Fluid Dynamics (CFD) (U01) Clinical Trial Required. 2021. Available online: https://grants.nih.gov/grants/guide/rfa-files/RFA-FD-21-020.html (accessed on 25 June 2021).
- Marple, V.A. History of Impactors—The First 110 Years. Aerosol Sci. Technol. 2004, 38, 247–292. [Google Scholar] [CrossRef]
- Taki, M.; Marriott, C.; Zeng, X.-M.; Martin, G.P. Aerodynamic deposition of combination dry powder inhaler formulations in vitro: A comparison of three impactors. Int. J. Pharm. 2010, 388, 40–51. [Google Scholar] [CrossRef]
- Stevens, J.M.; Bagby, J.W. Knowledge Transfer from Universities to Business: Returns for all Stakeholders? Organization 2001, 8, 259–268. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FY2016 Regulatory Science Report: Locally-Acting Orally-Inhaled and Nasal Drug Products. Available online: https://www.fda.gov/industry/generic-drug-user-fee-amendments/fy2016-regulatory-science-report-locally-acting-orally-inhaled-and-nasal-drug-products (accessed on 24 June 2021).
- Debackere, K.; Veugelers, R. The role of academic technology transfer organizations in improving industry science links. Res. Policy 2005, 34, 321–342. [Google Scholar] [CrossRef]
- Copley Scientific Limited Inhaler Testing Brochure. Quality Solutions for Inhaler Testing. 2019 Edition. Available online: https://www.copleyscientific.com/documents/ww/Inhaler (accessed on 14 July 2020).
- Finlay, W.H.; Golshahi, L.; Noga, M. Choosing 3-D Mouth-Throat Dimensions: A Rational Merging of Medical Imaging and Aerodynamics. In Respiratory Drug Delivery; Davis Healthcare International: River Grove, IL, USA, 2010; pp. 185–194. [Google Scholar]
- The Aerosol Research Lab of Alberta The Alberta Idealized Throat Geometry. Available online: https://sites.ualberta.ca/~arla/alberta_idealized_throat.html (accessed on 24 September 2020).
- Son, Y.-J.; Horng, M.; Copley, M.; McConville, J.T. Optimization of an In Vitro Dissolution Test Method for Inhalation Formulations. Dissolution Technol. 2010, 17, 6–13. [Google Scholar] [CrossRef]
- Velaga, S.P.; Djuris, J.; Cvijic, S.; Rozou, S.; Russo, P.; Colombo, G.; Rossi, A. Dry powder inhalers: An overview of the in vitro dissolution methodologies and their correlation with the biopharmaceutical aspects of the drug products. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2018, 113, 18–28. [Google Scholar] [CrossRef]
- Ocampo, A.; Lum, S.; Chow, F. Current challenges for FDA-regulated bioanalytical laboratories for human (BA/BE) studies. Part I: Defining the appropriate compliance standards—application of the principles of FDA GLP and FDA GMP to bioanalytical laboratories. Qual. Assur. J. 2007, 11, 3–15. [Google Scholar] [CrossRef]
- Baldeshwiler, A.M. History of FDA good laboratory practices. Qual. Assur. J. 2003, 7, 157–161. [Google Scholar] [CrossRef]
- Noonan, P.K. Outsourcing Bioavailability and Bioequivalence Studies to Contract Research Organizations. In Generic Drug Product Development and Therapeutic Equivalence; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Winterhalter, S.; Zeschky, M.B.; Neumann, L.; Gassmann, O. Business Models for Frugal Innovation in Emerging Markets: The Case of the Medical Device and Laboratory Equipment Industry. Technovation 2017, 66–67, 3–13. [Google Scholar] [CrossRef]
- Copley, M. Improving Inhaled Product Testing: Methods for Obtaining Better In vitro-In vivo Relationships. Pharm. Technol. 2013, 37. Available online: https://www.pharmtech.com/view/spray-drying-as-an-enabling-technology-for-inhalation-drug-delivery (accessed on 5 August 2020).
- The Free Library Chemimage Offers Bioequivalence Technology for Drug Makers. 2009. Available online: https://www.thefreelibrary.com/chemimage+offers+bioequivlance+technology+for+drug+makers.-a0196036571 (accessed on 26 June 2021).
- U.S. Food and Drug Administration. Draft Guidance on Albuterol Sulfate. Aerosol, Metered, Inhalation. 2016. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/psg/PSG_020503.pdf (accessed on 5 August 2020).
- U.S. Food and Drug Administration. Draft Guidance on Albuterol Sulfate. Metered Powder, Inhalation. 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/psg/PSG_205636.pdf (accessed on 5 August 2020).
- European Medicines Agency. Requirements for Clinical Documentation Orally Inhaled Products (OIP) Including the Requirements Demonstration of Therapeutic Equivalence between Two Use in Treatment Asthma and Chronic Obstructive Pulmonary Disease (COPD); European Medicines Agency: Amsterdam, The Netherlands, 2018; Available online: https://www.ema.europa.eu/en/requirements-clinical-documentation-orally-inhaled-products-oip-including-requirements-demonstration (accessed on 6 September 2020).
- Lexchin, J.; Bero, L.A.; Djulbegovic, B.; Clark, O. Pharmaceutical industry sponsorship and research outcome and quality: Systematic review. Br. Med. J. 2003, 326, 1167–1170. [Google Scholar] [CrossRef] [PubMed]
- DiMasi, J.A.; Grabowski, H.G.; Hansen, R.W. Innovation in the pharmaceutical industry: New estimates of R&D costs. J. Health Econ. 2016, 47, 20–33. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. What We Do. 2018. Available online: https://www.fda.gov/about-fda/what-we-do (accessed on 6 September 2020).
- European Medicines Agency. From Laboratory to Patient—The Journey of a Medicine Assessed by EMA. 2019. Available online: https://www.ema.europa.eu/en/documents/other/laboratory-patient-journey-centrally-authorised-medicine_en.pdf (accessed on 13 August 2020).
- U.S. Pharmacopeial Convention. USP and FDA Working Together to Protect Public Health|USP. 2018. Available online: https://www.usp.org/sites/default/files/usp/document/about/public-policy/USP-and-US-FDA-a-partnership.pdf (accessed on 13 August 2020).
- European Medicines Agency. European Directorate for the Quality of Medicines and HealthCare (EDQM) of the Council of Europe. 2008. Available online: https://www.ema.europa.eu/en/partners-networks/international-activities/multilateral-coalitions-initiatives/european-directorate-quality-medicines-healthcare-edqm-council-europe (accessed on 13 August 2020).
- U.S. Food and Drug Administration. GDUFA Reauthorization Performance Goals and Program Enhancements Fiscal Years 2018–2022. 2016. Available online: https://www.fda.gov/media/101052/download (accessed on 20 July 2020).
- U.S. Food and Drug Administration. Generic Drug User Fee Act Program Performance Goals and Procedures. 2012. Available online: https://www.fda.gov/media/82022/download (accessed on 13 July 2020).
- U.S. Food and Drug Administration. Leveraging Quantitative Methods and Modeling to Modernize Generic Drug Development and Review. In Proceedings of the Public Workshop, 2–3 October 2017; Available online: https://www.fda.gov/drugs/news-events-human-drugs/leveraging-quantitative-methods-and-modeling-modernize-generic-drug-development-and-review-public (accessed on 13 July 2020).
- DIA/FDA Conference. In Proceedings of the Complex Drug-Device Generic Combination Products Meeting, 9–10 October 2018; Available online: https://www.diaglobal.org/en/conference-listing/meetings/2018/10/complex-drug-device-generic-combination-products (accessed on 13 July 2020).
- U.S. Food and Drug Administration. New Insights for Product Development and Bioequivalence Assessments of Generic Orally Inhaled and Nasal Drug Products. 2018. Available online: https://www.fda.gov/drugs/news-events-human-drugs/new-insights-product-development-and-bioequivalence-assessments-generic-orally-inhaled-and-nasal (accessed on 13 July 2020).
- Chen, M.L.; Blume, H.; Beuerle, G.; Davit, B.; Mehta, M.; Potthast, H.; Schug, B.; Tsang, Y.C.; Wedemeyer, R.S.; Weitschies, W.; et al. The Global Bioequivalence Harmonization Initiative: Summary report for EUFEPS international conference. Eur. J. Pharm. Sci. 2018, 111, 153–157. [Google Scholar] [CrossRef]
- Hastedt, J.E.; Bäckman, P.; Clark, A.R.; Doub, W.; Hickey, A.; Hochhaus, G.; Kuehl, P.J.; Lehr, C.-M.; Mauser, P.; McConville, J.; et al. Scope and relevance of a pulmonary biopharmaceutical classification system AAPS/FDA/USP Workshop March 16–17th, 2015 in Baltimore, MD. AAPS Open 2016, 2, 1. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FY 2021 Generic Drug Science and Research Initiatives Public Workshop. 2021. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fy-2021-generic-drug-science-and-research-initiatives-public-workshop-06232021-06232021 (accessed on 26 June 2021).
- U.S. Food and Drug Administration. GDUFA Regulatory Science Priority Initiatives for Fiscal Year 2019. 2019. Available online: https://www.fda.gov/media/119040/download?utm_campaign=SBIA%3AFDApublishesFY2019GDUFAScienceandResearchReport&utm_medium=email&utm_source=Eloqua (accessed on 25 June 2021).
- U.S. Food and Drug Administration. 2018 Annual Report|Office of Generic Drugs. 2018. Available online: https://fda.report/media/120593/OGD_AnnualReport_2018_ONLINE_190515_1158.pdf (accessed on 25 June 2021).
- U.S. Food and Drug Administration. FY2020 1. U.S. Food and Drug Administration. FY2020 GDFUA Science and research report. 2021. Available online: https://www.fda.gov/media/146749/download#page=34 (accessed on 25 June 2021).
- U.S. Food and Drug Administration. GDUFA Reauthorization. 2012. Available online: https://www.fda.gov/industry/generic-drug-user-fee-amendments/gdufa-reauthorization (accessed on 24 June 2021).
- U.S. Pharmacopeial Convention. What Is a USP Monograph. 2019. Available online: https://www.usp.org/about/public-policy/overview-of-monographs (accessed on 26 June 2021).
- EDQM Council of Europe. Elaborations and Revisions of the European Pharmacopoeia—EDQM. Available online: https://www.edqm.eu/en/european-pharmacopoeia-elaboration-revisions-606.html (accessed on 26 June 2021).
- U.S. Pharmacopeial Convention. Exploring Continuous Manufacturing Technology and Applications in the Pharmaceutical Industry|U.S. Pharmacopeia Blog. 2017. Available online: https://qualitymatters.usp.org/exploring-continuous-manufacturing-technology-and-applications-pharmaceutical-industry (accessed on 1 September 2020).
- Coulter, A.; Jenkinson, C. European patients’ views on the responsiveness of health systems and healthcare providers. Eur. J. Public Health 2005, 15, 355–360. [Google Scholar] [CrossRef]
- Dunne, S.; Shannon, B.; Hannigan, A.; Dunne, C.; Cullen, W. Physician and pharmacist perceptions of generic medicines: What they think and how they differ. Health Policy 2014, 116, 214–223. [Google Scholar] [CrossRef]
- Kupferschmidt, K.; Cohen, J. Race to find COVID-19 treatments accelerates. Science 2020, 367, 1412–1413. [Google Scholar] [CrossRef]
- Webb, J.; Shah, L.D.; Lynch, H.F. Ethically Allocating COVID-19 Drugs via Pre-approval Access and Emergency Use Authorization. Am. J. Bioeth. 2020, 20, 4–17. [Google Scholar] [CrossRef]
- Rise, M.B.; Solbjør, M.; Lara, M.C.; Westerlund, H.; Grimstad, H.; Steinsbekk, A. Same description, different values. How service users and providers define patient and public involvement in health care. Heal. Expect. 2013, 16, 266–276. [Google Scholar] [CrossRef]
- Dunne, S.S.; Dunne, C.P. What do people really think of generic medicines? A systematic review and critical appraisal of literature on stakeholder perceptions of generic drugs. BMC Med. 2015, 13, 173. [Google Scholar] [CrossRef]
- Blasco Oliete, M.; Torres Bouza, C.; Medina Bustillo, B.; Sanz Cuesta, T.; Neira León, M. Opinión de los usuarios de atención primaria sobre los medicamentos genéricos y el coste de la medicación. Atención Primaria 2003, 31, 170–177. [Google Scholar] [CrossRef]
- Amidon, G.; Lesko, L.; Midha, K.; Shah, V.; Hilfinger, J. FDA Bioequivalence Standards; Advances in the Pharmaceutical Sciences Series; Springer: New York, NY, USA; Heidelberg, Germany; Dordrecht, The Netherlands; London, UK; Silver Spring, MD, USA, 2014; ISBN 978-0-9790119-0-0. [Google Scholar]
- Al-Numani, D.; Colucci, P.; Ducharme, M.P. Rethinking bioequivalence and equivalence requirements of orally inhaled drug products. Asian J. Pharm. Sci. 2015, 10, 461–471. [Google Scholar] [CrossRef][Green Version]
- Saluja, B.; Li, B.V.; Lee, S.L. Bioequivalence for orally inhaled and nasal drug products. In FDA Bioequivalence Standards; Springer: Berlin/Heidelberg, Germany, 2014; Volume 13, pp. 369–394. [Google Scholar]
- Forbes, B.; Bäckman, P.; Christopher, D.; Dolovich, M.; Li, B.V.; Morgan, B. In Vitro Testing for Orally Inhaled Products: Developments in Science-Based Regulatory Approaches. AAPS J. 2015, 17, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Chambers, F.; De, S.; Baxter, S.; Parkinson, A.; Doub, B.; Breakwell, I.; Fischer, M.; Nagao, L.M.; Ag, S.; Group, V. Plume Geometry Testing Relevance and Methodology: An IPAC-RS Survey. Respir. Drug Deliv. 2018, 437–442. Available online: https://www.rddonline.com/rdd/article.php?ArticleID=2395 (accessed on 25 March 2020).
- Kuribayashi, R.; Yamaguchi, T.; Sako, H.; Takishita, T.; Takagi, K. Bioequivalence Evaluations of Generic Dry Powder Inhaler Drug Products: Similarities and Differences Between Japan, USA, and the European Union. Clin. Pharmacokinet. 2017, 56, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, G.; Chen, M.-J.; Kurumaddali, A.; Schilling, U.; Jiao, Y.; Drescher, S.K.; Amini, E.; Kandala, B.; Tabulov, C.; Shao, J.; et al. Can Pharmacokinetic Studies Assess the Pulmonary Fate of Dry Powder Inhaler Formulations of Fluticasone Propionate? AAPS J. 2021, 23, 48. [Google Scholar] [CrossRef]
- Zou, P.; Yu, L.X. Pharmacodynamic endpoint bioequivalence studies. AAPS Adv. Pharm. Sci. Ser. 2014, 13, 217–241. [Google Scholar] [CrossRef]
- Kelly, H.W. Comparison of inhaled corticosteroids: An update. Ann. Pharmacother. 2009, 43, 519–527. [Google Scholar] [CrossRef]
- Raissy, H.H.; Kelly, H.W.; Harkins, M.; Szefler, S.J. Inhaled corticosteroids in lung diseases. Am. J. Respir. Crit. Care Med. 2013, 187, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.S.; Byron, P.R. Inhaling medicines: Delivering drugs to the body through the lungs. Nat. Rev. Drug Discov. 2007, 6, 67–74. [Google Scholar] [CrossRef]
- Smyth, H.D.C.; Hickey, A.J. Controlled Pulmonary Drug Delivery; Springer: Berlin/Heidelberg, Germany, 2011; ISBN 9781461428954. [Google Scholar]
- Forbes, B.; Richer, N.H.; Buttini, F. Dissolution: A Critical Performance Characteristic of Inhaled Products? In Pulmonary Drug Delivery; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 223–240. ISBN 978-1-118-79953-6. [Google Scholar]
- Salama, R.O.; Traini, D.; Chan, H.-K.; Young, P.M. Preparation and characterisation of controlled release co-spray dried drug–polymer microparticles for inhalation 2: Evaluation of in vitro release profiling methodologies for controlled release respiratory aerosols. Eur. J. Pharm. Biopharm. 2008, 70, 145–152. [Google Scholar] [CrossRef] [PubMed]
- May, S.; Jensen, B.; Wolkenhauer, M.; Schneider, M.; Lehr, C.M. Dissolution techniques for in vitro testing of dry powders for inhalation. Pharm. Res. 2012, 29, 2157–2166. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M.; Feddah, M.R. A novel method for assessing dissolution of aerosol inhaler products. Int. J. Pharm. 2003, 255, 175–187. [Google Scholar] [CrossRef]
- Bhagwat, S.; Schilling, U.; Chen, M.-J.; Wei, X.; Delvadia, R.; Absar, M.; Saluja, B.; Hochhaus, G. Predicting Pulmonary Pharmacokinetics from In Vitro Properties of Dry Powder Inhalers. Pharm. Res. 2017, 34, 2541–2556. [Google Scholar] [CrossRef] [PubMed]
- Arora, D.; Shah, K.A.; Halquist, M.S.; Sakagami, M. In Vitro Aqueous Fluid-Capacity-Limited Dissolution Testing of Respirable Aerosol Drug Particles Generated from Inhaler Products. Pharm. Res. 2010, 27, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Gerde, P.; Malmlöf, M.; Havsborn, L.; Sjöberg, C.-O.; Ewing, P.; Eirefelt, S.; Ekelund, K. Dissolv It: An In Vitro Method for Simulating the Dissolution and Absorption of Inhaled Dry Powder Drugs in the Lungs. Assay Drug Dev. Technol. 2017, 15, 77–88. [Google Scholar] [CrossRef]
- Radivojev, S.; Zellnitz, S.; Paudel, A.; Fröhlich, E. Searching for physiologically relevant in vitro dissolution techniques for orally inhaled drugs. Int. J. Pharm. 2019, 556, 45–56. [Google Scholar] [CrossRef]
- Price, R.; Shur, J.; Ganley, W.; Farias, G.; Fotaki, N.; Conti, D.S.; Delvadia, R.; Absar, M.; Saluja, B.; Lee, S. Development of an Aerosol Dose Collection Apparatus for In Vitro Dissolution Measurements of Orally Inhaled Drug Products. AAPS J. 2020, 22, 47. [Google Scholar] [CrossRef] [PubMed]
- García-Arieta, A. A European Perspective on Orally Inhaled Products: In Vitro Requirements for a Biowaiver. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Hindle, M.; Delvadia, R.R.; Byron, P.R. In Vitro Tests for Aerosol Deposition. V: Using Realistic Testing to Estimate Variations in Aerosol Properties at the Trachea. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Burnell, P.K.P.; Asking, L.; Borgström, L.; Nichols, S.C.; Olsson, B.; Prime, D.; Shrubb, I. Studies of the Human Oropharyngeal Airspaces Using Magnetic Resonance Imaging IV—The Oropharyngeal Retention Effect for Four Inhalation Delivery Systems. J. Aerosol Med. 2007, 20, 269–281. [Google Scholar] [CrossRef]
- Olsson, B.; Borgström, L.; Lundbäck, H.; Svensson, M. Validation of a General In Vitro Approach for Prediction of Total Lung Deposition in Healthy Adults for Pharmaceutical Inhalation Products. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Grgic, B.; Finlay, W.; Burnell, P.K.; Heenan, A. In vitro intersubject and intrasubject deposition measurements in realistic mouth–throat geometries. J. Aerosol Sci. 2004, 35, 1025–1040. [Google Scholar] [CrossRef]
- Longest, P.W.; Hindle, M.; Das Choudhuri, S.; Xi, J. Comparison of ambient and spray aerosol deposition in a standard induction port and more realistic mouth–throat geometry. J. Aerosol Sci. 2008, 39, 572–591. [Google Scholar] [CrossRef]
- Wei, X.; Hindle, M.; Kaviratna, A.; Huynh, B.K.; Delvadia, R.R.; Sandell, D.; Byron, P.R. In Vitro Tests for Aerosol Deposition. VI: Realistic Testing with Different Mouth–Throat Models and In Vitro—In Vivo Correlations for a Dry Powder Inhaler, Metered Dose Inhaler, and Soft Mist Inhaler. J. Aerosol Med. Pulm. Drug Deliv. 2018, 31, 358–371. [Google Scholar] [CrossRef]
- Moraga-Espinoza, D.; Warnken, Z.; Moore, A.; Williams, R.O.; Smyth, H.D.C. A modified USP induction port to characterize nasal spray plume geometry and predict turbinate deposition under flow. Int. J. Pharm. 2018, 548, 305–313. [Google Scholar] [CrossRef]
- Moraga-Espinoza, D.; Eshaghian, E.; Smyth, H.D.C. Mass Median Plume Angle: A novel approach to characterize plume geometry in solution based pMDIs. Int. J. Pharm. 2018, 543, 376–385. [Google Scholar] [CrossRef]
- Kerekes, A.; Veres, M.; Himics, L.; Tóth, S.; Czitrovszky, A.; Oszetzky, D.; Horváth, A.; Kugler, S.; Koós, M.; Nagy, A. Determination of the deposited amount of inhalation drugs in realistic human airways by Raman and infrared spectroscopy. Measurement 2017, 104, 237–242. [Google Scholar] [CrossRef]
- Verbanck, S.; Ghorbaniasl, G.; Biddiscombe, M.F.; Dragojlovic, D.; Ricks, N.; Lacor, C.; Ilsen, B.; de Mey, J.; Schuermans, D.; Underwood, S.R.; et al. Inhaled Aerosol Distribution in Human Airways: A Scintigraphy-Guided Study in a 3D Printed Model. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 525–533. [Google Scholar] [CrossRef]
- Kolewe, E.L.; Feng, Y.; Fromen, C.A. Realizing Lobe-Specific Aerosol Targeting in a 3D-Printed In Vitro Lung Model. J. Aerosol Med. Pulm. Drug Deliv. 2020. [Google Scholar] [CrossRef]
- Sonnenberg, A.H.; Taylor, E.; Mondoñedo, J.R.; Jawde, S.B.; Amin, S.D.; Song, J.; Grinstaff, M.W.; Suki, B. Breath Hold Facilitates Targeted Deposition of Aerosolized Droplets in a 3D Printed Bifurcating Airway Tree. Ann. Biomed. Eng. 2020. [Google Scholar] [CrossRef]
- Borojeni, A.A.T.; Noga, M.L.; Martin, A.R.; Finlay, W.H. An idealized branching airway geometry that mimics average aerosol deposition in pediatric central conducting airways. J. Aerosol Sci. 2015, 85, 10–16. [Google Scholar] [CrossRef]
- Lizal, F.; Elcner, J.; Hopke, P.K.; Jedelsky, J.; Jicha, M. Development of a realistic human airway model. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2012, 226, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Su, W.-C.; Chen, Y.; Xi, J. A new approach to estimate ultrafine particle respiratory deposition. Inhal. Toxicol. 2019, 31, 35–43. [Google Scholar] [CrossRef]
- Newman, S.P. Use of gamma scintigraphy to evaluate the performance of new inhalers. J. Aerosol Med. 1999, 12, S25–S31. [Google Scholar] [CrossRef] [PubMed]
- Perring, S.; Summers, Q.; Fleming, J.S.; Nassim, M.A.; Holgate, S.T. A new method of quantification of the pulmonary regional distribution of aerosols using combined CT and SPECT and its application to nedocromil sodium administered by metered dose inhaler. Br. J. Radiol. 1994, 67, 46–53. [Google Scholar] [CrossRef]
- Dolovich, M.; Labiris, R. Imaging drug delivery and drug responses in the lung. Proc. Am. Thorac. Soc. 2004, 1, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Dolovich, M.B.; Bailey, D.L. Positron emission tomography (PET) for assessing aerosol deposition of orally inhaled drug products. J. Aerosol Med. Pulm. Drug Deliv. 2012, 25. [Google Scholar] [CrossRef] [PubMed]
- Darquenne, C.; Fleming, J.S.; Katz, I.; Martin, A.R.; Schroeter, J.; Usmani, O.S.; Venegas, J.; Schmid, O. Bridging the Gap Between Science and Clinical Efficacy: Physiology, Imaging, and Modeling of Aerosols in the Lung. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 107–126. [Google Scholar] [CrossRef]
- Usmani, O.S.; Biddiscombe, M.F.; Barnes, P.J. Regional Lung Deposition and Bronchodilator Response as a Function of β2 -Agonist Particle Size. Am. J. Respir. Crit. Care Med. 2005, 172, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Hendeles, L.; Daley-Yates, P.T.; Hermann, R.; De Backer, J.; Dissanayake, S.; Horhota, S.T. Pharmacodynamic Studies to Demonstrate Bioequivalence of Oral Inhalation Products. AAPS J. 2015, 17, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Austin, D.J.; Daley-Yates, P.T. Evaluation Of Exhaled Nitric Oxide (eNO) As A Tool For Bioequivalence Testing Of Inhaled Corticosteroids. In A60. Assessing Pulmonary Function: Airways, Mechanics, and Gas Exchange; American Thoracic Society International Conference Abstracts; American Thoracic Society: Philadelphia, PA, USA, 2013; p. A1927. Available online: https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2013.187.1_MeetingAbstracts.A1927 (accessed on 13 July 2020).
- Hajian, B.; De Backer, J.; Vos, W.; Van Holsbeke, C.; Clukers, J.; De Backer, W. Functional respiratory imaging (FRI) for optimizing therapy development and patient care. Expert Rev. Respir. Med. 2016, 10, 193–206. [Google Scholar] [CrossRef] [PubMed]
- De Backer, J.; Van Holsbeke, C.; Vos, W.; Vinchurkar, S.; Dorinsky, P.; Rebello, J.; Mangale, M.; Hajian, B.; De Backer, W. Assessment of lung deposition and analysis of the effect of fluticasone/salmeterol hydrofluoroalkane (HFA) pressurized metered dose inhaler (pMDI) in stable persistent asthma patients using functional respiratory imaging. Expert Rev. Respir. Med. 2016, 10, 927–933. [Google Scholar] [CrossRef]
- De Backer, W.; Vos, W.; Van Holsbeke, C.; Vinchurkar, S.; Claes, R.; Hufkens, A.; Parizel, P.M.; Bedert, L.; De Backer, J. The effect of roflumilast in addition to LABA/LAMA/ICS treatment in COPD patients. Eur. Respir. J. 2014, 44, 527–529. [Google Scholar] [CrossRef]
- Topole, E.; Usmani, O.; Mignot, B.; Belmans, D.; Van Holsbeke, C.; De Backer, J.; Osello, R.; Cuoghi, E.; Georges, G.; Scichilone, N. Lung deposition of extrafine vs. non-extrafine triple therapies in patients with COPD using Functional Respiratory Imaging (FRI). In Proceedings of the ERS International Congress 2019 Abstracts; European Respiratory Society: Madrid, España, 2019; p. PA3167. [Google Scholar] [CrossRef]
- De Backer, W.; De Backer, J.; Vos, W.; Verlinden, I.; Van Holsbeke, C.; Clukers, J.; Hajian, B.; Siddiqui, S.; Jenkins, M.; Reisner, C.; et al. A randomized study using functional respiratory imaging to characterize bronchodilator effects of glycopyrrolate/formoterol fumarate delivered by a metered dose inhaler using co-suspension delivery technology in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 2673–2684. [Google Scholar] [CrossRef]
- Oldham, M.J. Computational Fluid Dynamic Predictions and Experimental Results for Particle Deposition in an Airway Model. Aerosol Sci. Technol. 2000, 32, 61–71. [Google Scholar] [CrossRef]
- Nowak, N.; Kakade, P.P.; Annapragada, A.V. Computational Fluid Dynamics Simulation of Airflow and Aerosol Deposition in Human Lungs. Ann. Biomed. Eng. 2003, 31, 374–390. [Google Scholar] [CrossRef]
- Longest, P.W.; Holbrook, L.T. In silico models of aerosol delivery to the respiratory tract—Development and applications. Adv. Drug Deliv. Rev. 2012, 64, 296–311. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Bass, K.; Dutta, R.; Rani, V.; Thomas, M.L.; El-Achwah, A.; Hindle, M. Use of computational fluid dynamics deposition modeling in respiratory drug delivery. Expert Opin. Drug Deliv. 2019, 16, 7–26. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Feng, Y. Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review. Int. J. Environ. Res. Public Health 2013, 10, 4454–4485. [Google Scholar] [CrossRef] [PubMed]
- Simulations Plus. GastroPlus PBPK Modeling Software. 2019. Available online: https://www.simulations-plus.com/software/gastroplus/ (accessed on 26 June 2019).
- Certara USA Inc. Simcyp Simulator—Certara. Brochure. 2019. Available online: https://www.certara.com/software/physiologically-based-pharmacokinetic-modeling-and-simulation/simcyp-simulator/?ap%5B0%5D=PKPD&ap%5B1%5D=PBPK (accessed on 26 June 2019).
- Lukacova, V.; Chaudhuri, S.R. Simulating Delivery of Pulmonary (and Intranasal) Aerosolised Drugs. OnDrugDelivery. 2010. Available online: http://staging.ondrugdelivery.com/wp-content/uploads/2018/11/Nov2010.pdf#page=26 (accessed on 26 June 2019).
- Kaviratna, A.; Tian, G.; Liu, X.; Delvadia, R.; Lee, S.; Guo, C. Evaluation of Bio-relevant Mouth-Throat Models for Characterization of Metered Dose Inhalers. AAPS PharmSciTech 2019, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Inhalation Technology Focus Group/International; Pharmaceutical Aerosol Consortium on Regulation; Sience Tests and Methods Technical Team; Nagao, L.M. Recommendations to the food and drug administration: Metered dose inhaler test and methods in the chemistry, manufacturing, and controls draft guidances for metered inhalers and dry powder inhalers. Drug Inf. J. 2002, 36, 549–556. [Google Scholar]
- Chen, Y.; Young, P.M.; Murphy, S.; Fletcher, D.F.; Long, E.; Lewis, D.; Church, T.; Traini, D. High-Speed Laser Image Analysis of Plume Angles for Pressurised Metered Dose Inhalers: The Effect of Nozzle Geometry. AAPS PharmSciTech 2017, 18, 782–789. [Google Scholar] [CrossRef]
- Daley-Yates, P.T.; Parkins, D.A. Establishing bioequivalence for inhaled drugs; weighing the evidence. Expert Opin. Drug Deliv. 2011, 8, 1297–1308. [Google Scholar] [CrossRef]
- Barros, A.S.; Costa, A.; Sarmento, B. Building three-dimensional lung models for studying pharmacokinetics of inhaled drugs. Adv. Drug Deliv. Rev. 2020. [Google Scholar] [CrossRef]
- Newman, S.P.; Wilding, I.R. Gamma scintigraphy: An in vivo technique for assessing the equivalence of inhaled products. Int. J. Pharm. 1998, 170, 1–9. [Google Scholar] [CrossRef]
- Mobley, C.; Hochhaus, G. Methods used to assess pulmonary deposition and absorption of drugs. Drug Discov. Today 2001, 6, 367–375. [Google Scholar] [CrossRef]
- Huang, F.; Zhu, Q.; Zhou, X.; Gou, D.; Yu, J.; Li, R.; Tong, Z.; Yang, R. Role of CFD based in silico modelling in establishing an in vitro-in vivo correlation of aerosol deposition in the respiratory tract. Adv. Drug Deliv. Rev. 2021, 170, 369–385. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Gelb, A.F.; Moridzadeh, R.; Singh, D.H.; Fraser, C.; George, S.C. In moderate-to-severe asthma patients monitoring exhaled nitric oxide during exacerbation is not a good predictor of spirometric response to oral corticosteroid. J. Allergy Clin. Immunol. 2012, 129, 1491–1498. [Google Scholar] [CrossRef]
- De Backer, J.; Vos, W.; Vinchurkar, S.; Van Holsbeke, C.; Poli, G.; Claes, R.; Salgado, R.; De Backer, W. The Effects of Extrafine Beclometasone/Formoterol (BDP/F) on Lung Function, Dyspnea, Hyperinflation, and Airway Geometry in COPD Patients: Novel Insight Using Functional Respiratory Imaging. J. Aerosol Med. Pulm. Drug Deliv. 2014, 28, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Gieschke, R.; Steimer, J.L. Pharmacometrics: Modelling and simulation tools to improve decision making in clinical drug development. Eur. J. Drug Metab. Pharmacokinet. 2000, 25, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Kandala, B.; Hochhaus, G. Pharmacometrics in Pulmonary Diseases. In Applied Pharmacometrics; Schmidt, S., Derendorf, H., Eds.; AAPS Advances in the Pharmaceutical Sciences Series; Springer: New York, NY, USA, 2014; pp. 349–382. ISBN 978-1-4939-1304-6. [Google Scholar]
- Bäckman, P.; Arora, S.; Couet, W.; Forbes, B.; de Kruijf, W.; Paudel, A. Advances in experimental and mechanistic computational models to understand pulmonary exposure to inhaled drugs. Eur. J. Pharm. Sci. 2018, 113, 41–52. [Google Scholar] [CrossRef]
- Borghardt, J.M.; Weber, B.; Staab, A.; Kloft, C. Pharmacometric Models for Characterizing the Pharmacokinetics of Orally Inhaled Drugs. AAPS J. 2015, 17, 853–870. [Google Scholar] [CrossRef]
- Amidon, G.L.; Lennernäs, H.; Shah, V.P.; Crison, J.R. A Theoretical Basis for a Biopharmaceutic Drug Classification: The Correlation of in Vitro Drug Product Dissolution and in Vivo Bioavailability. Pharm. Res. Off. J. Am. Assoc. Pharm. Sci. 1995, 12, 413–420. [Google Scholar] [CrossRef]
- European Medicines Agency. ICH M9 Guideline on Biopharmaceutics Classification System-Based Biowaivers ICH M9 on Biopharmaceutics Classification System-Based Biowaivers. 2020. Available online: https://www.ema.europa.eu/en/ich-m9-biopharmaceutics-classification-system-based-biowaivers (accessed on 8 September 2020).
- U.S. Food and Drug Administration. Guidance for Industry. Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System. 2017. Available online: https://www.gmp-compliance.org/files/guidemgr/UCM070246.pdf (accessed on 8 September 2020).
- Hastedt, J.E. Biopharmaceutical Classification of Inhaled Medicines: Development of an iBCS. In Proceedings of the 4th FDA/PQRI Conference, Rockville, MD, USA, 9–11 April 2019; Available online: https://pqri.org/wp-content/uploads/2019/03/1-Development-of-an-iBCS-JHastedt-Final.pdf (accessed on 26 June 2021).
- Eixarch, H.; Haltner-Ukomadu, E.; Beisswenger, C.; Bock, U. Drug Delivery to the Lung: Permeability and Physicochemical Characteristics of Drugs as the Basis for a Pulmonary Biopharmaceutical Classification System (pBCS). J. Epithel. Biol. Pharmacol. 2010, 3, 1–14. [Google Scholar]
- Gray, V. Meeting Report: AAPS Workshop on Inhalation Product Biopharmaceutical Classification System Development: Challenges and Opportunities. Dissolution Technol. 2015, 22, 52–55. [Google Scholar] [CrossRef]
- Polli, J.E.; Abrahamsson, B.S.I.; Yu, L.X.; Amidon, G.L.; Baldoni, J.M.; Cook, J.A.; Fackler, P.; Hartauer, K.; Johnston, G.; Krill, S.L.; et al. Summary workshop report: Bioequivalence, biopharmaceutics classification system, and beyond. AAPS J. 2008, 10, 373–379. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hickey, A.J. Emerging trends in inhaled drug delivery. Adv. Drug Deliv. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sou, T.; Bergström, C.A.S. Contemporary Formulation Development for Inhaled Pharmaceuticals. J. Pharm. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, A.; Fotaki, N. In Vitro Dissolution for Inhalation Products. In In Vitro Drug Release Testing of Special Dosage Forms; Wiley: Hoboken, NJ, USA, 2019; pp. 119–153. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Objective | Grants and Contracts Related to BE of OIDPs Awarded or Completed during 2020 | Institution; Grant or Contract |
|---|---|---|
| Research topic 1: Drug–Device Combination Products | ||
| Evaluation of the impact of differences in the user interface between complex generic drug–device combination products and their RLDs on therapeutic equivalence | Development of Computational Models to Predict Delivery of Inhalation Drug Powders: From Deagglomeration in Devices to Deposition in Airways | University of Sydney; Grant (1U01FD006525) |
| Patient’s Perception of DPI Airflow Resistance | Imperial College of Science and Technology, London; Contract (HHSF223201710072C) | |
| Comprehensive Evaluation of Formulation Effects on MDI Performance | University of Florida; Grant (5U01FD004943) | |
| Investigating the Impact of SMI In Vitro Characteristics on Human Airway Deposition: A Combined In Vitro/In Silico Approach | FDA | |
| Research topic 2: Inhalation and Nasal Products | ||
| Identify which factors can significantly impact how drugs are aerosolized, distributed regionally and absorbed once deposited in the lung | A Cluster-Based Assessment of Drug Delivery in Asthmatic Small Airways | University of Iowa; Grant (1U01FD005837) |
| CFD and DEM Approach for Predictions of DPI Drug Delivery (U01) | Princeton University; Grant (1U01FD006514) | |
| Development of Computational Models to Predict Delivery of Inhalation Drug Powders: From Deagglomeration in Devices to Deposition in Airways | University of Sydney; Grant (1U01FD006525) | |
| Systematic evaluation of the ex-throat plume properties of MDI formulations | University of Florida; Contract (75F40119C10154C) | |
| Patient’s Perception of DPI Airflow Resistance | Imperial College of Science and Technology, London; Contract (HHSF223201710072C) | |
| Modifications and Improvements to Hybrid CFD-PBPK Models for Predication of Nasal Corticosteroid Deposition, Absorption, and Bioavailability | Applied Research Associates; Contract (75F40119C10079) | |
| Investigating the Microstructure of DPIs Using Orthogonal Analytical Approaches | University of Bath; Contract (HHSF223201710116C) | |
| Evaluating Batch to Batch Variability and Its Origins in DPIs | The University of Texas at Austin; Contract (HHSF223201810169C) | |
| Comprehensive Evaluation of Formulation Effects on MDI Performance | University of Florida; Grant (5U01FD004943) | |
| Assessment of Variability and Dose Sensitivity of FEV1 in Comparative Clinical Endpoint BE Studies of OIDPs | FDA | |
| CFD Models of Droplet Formulation from MDI | ||
| CFD Models of SMIs | ||
| In Vitro Performance Testing of SMIs | ||
| OIDP Data Collection and Analysis from Drug Product Submissions | ||
| Physiological Mouth-Throat Models for Inhalation Products | ||
| Product Quality and Performance Evaluation of Tiotropium Bromide Inhalation Powder Drug Products | ||
| The Use of Lung-on-a-Chip to Obtain Physiologically Relevant Parameters for OIDPs | ||
| Research topic 3: Locally Acting Physiologically Based Pharmacokinetic Modeling | ||
| Development and advance in mechanistic-based modeling, such as PBPK modeling and CFD, in order to better inform the role that product properties play in local bioavailability | A Cluster-Based Assessment of Drug Delivery in Asthmatic Small Airways | University of Iowa; Grant (1U01FD005837) |
| Modeling Complex Particle Interactions in DPI Based Drug Delivery | Princeton University; Grant (1U01FD006514) | |
| Development of Computational Models to Predict Delivery of Inhalation Drug Powders: From Deagglomeration in Devices to Deposition in Airways | University of Sydney; Grant (1U01FD006525) | |
| A Multiscale Computational Framework for Bioequivalence of OIDs | CFD Research Corporation (CFDRC); Contract (HHSF223201810182C) | |
| CFD Models of Droplet Formulation from MDI | FDA | |
| CFD Models of SMIs | ||
| Impact of SMI In Vitro Characteristics on Human Airway Deposition: A Combined In Vitro/In Silico Approach | ||
| Laser Diffraction of Soft Mist Inhalers | ||
| Research topic 4: Quantitative Clinical Pharmacology | ||
| Development of clinically relevant BE criteria, design of efficient BE studies and research of alternative BE approaches. Quantitative clinical pharmacology is a quantitative platform that describes drug disposition, drug action and associated variability in humans. | Batch to Batch Variability: Exploring Solutions for Generic BE pathway | University of Maryland; Contract (75F40119C10068) |
| Assessment of Variability and Dose Sensitivity of FEV1 in Comparative Clinical Endpoint BE Studies of OIDPs | FDA | |
| Method | Key Factors for Bioequivalence | Limitations | Current State |
|---|---|---|---|
| In vitro methods | |||
| Dissolution test [17,69,70,71,72,73,74,75] |
|
| Need more consensus and investigations on some topics |
| Mouth-throat models [16,78,79,80,81,82,83] |
|
|
|
| Quantitative plume geometry analysis [84,85] | Allows better analytical analysis of the plume geometry | Large batches for the analysis of each of the removable parts |
|
| 3D-printed lung models [86,87,88,89,90,91,92] | Realistic in vitro deposition pattern analysis |
|
|
| In vivo methods | |||
| Imaging of deposition patterns [93,94,95,96,97,98] | Realistic and reliable comparisons between formulations |
|
|
| Biomarkers: exhaled nitric oxide (eNO) [99,100] | Alternative biomarker for current endpoint studies |
| Not recommended for use by the FDA [5,58] |
| Functional respiratory imaging (FRI) [101,102,103,104,105] | Novel biomarkers for anti-inflammatory drugs |
| Commercially available |
| In silico methods | |||
| Computational fluid dynamics (CFD) [106,107,108,109,110] | Allows simulating the flow of the device and its behavior |
| Commercially available software |
| Pharmacometrics: PBPK and empirical methods [111,112,113] | Predict the PK behavior of a formulation |
| There is software available with a modality for inhalation drugs |
| Others | |||
| Inhalation Biopharmaceutical Classification System (iBCS) [2,40] |
| Depends on the advances in the development of dissolution tests | Still in development |
| Class | Solubility | Permeability | IVIVC in giBCS for Oral Drugs | IVIVC in iBCS for OIDPs |
|---|---|---|---|---|
| I | high | high | Complete and fast absorption | Lung dose deposited is equal to the dose available for absorption Short absorption time |
| II | low | high | Absorption is limited to the dissolution rate | Lung dose deposited is higher than the dose available for absorption Long mean time for absorption |
| III | high | low | Absorption rate is limited to the intestinal permeability | Lung dose deposited is similar to the dose available for absorption Long mean time for absorption |
| IV | low | low | Poorly absorbed | Lung dose deposited is higher than the dose available for absorption Very long mean time for absorption |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallegos-Catalán, J.; Warnken, Z.; Bahamondez-Canas, T.F.; Moraga-Espinoza, D. Innovating on Inhaled Bioequivalence: A Critical Analysis of the Current Limitations, Potential Solutions and Stakeholders of the Process. Pharmaceutics 2021, 13, 1051. https://doi.org/10.3390/pharmaceutics13071051
Gallegos-Catalán J, Warnken Z, Bahamondez-Canas TF, Moraga-Espinoza D. Innovating on Inhaled Bioequivalence: A Critical Analysis of the Current Limitations, Potential Solutions and Stakeholders of the Process. Pharmaceutics. 2021; 13(7):1051. https://doi.org/10.3390/pharmaceutics13071051
Chicago/Turabian StyleGallegos-Catalán, Jonattan, Zachary Warnken, Tania F. Bahamondez-Canas, and Daniel Moraga-Espinoza. 2021. "Innovating on Inhaled Bioequivalence: A Critical Analysis of the Current Limitations, Potential Solutions and Stakeholders of the Process" Pharmaceutics 13, no. 7: 1051. https://doi.org/10.3390/pharmaceutics13071051
APA StyleGallegos-Catalán, J., Warnken, Z., Bahamondez-Canas, T. F., & Moraga-Espinoza, D. (2021). Innovating on Inhaled Bioequivalence: A Critical Analysis of the Current Limitations, Potential Solutions and Stakeholders of the Process. Pharmaceutics, 13(7), 1051. https://doi.org/10.3390/pharmaceutics13071051