
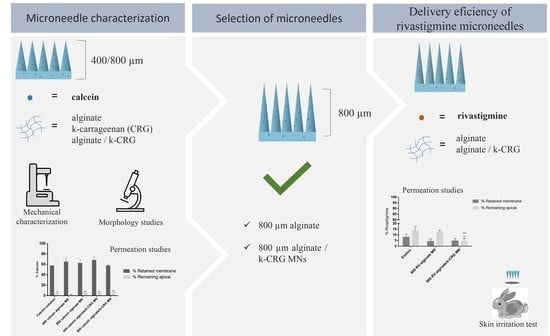
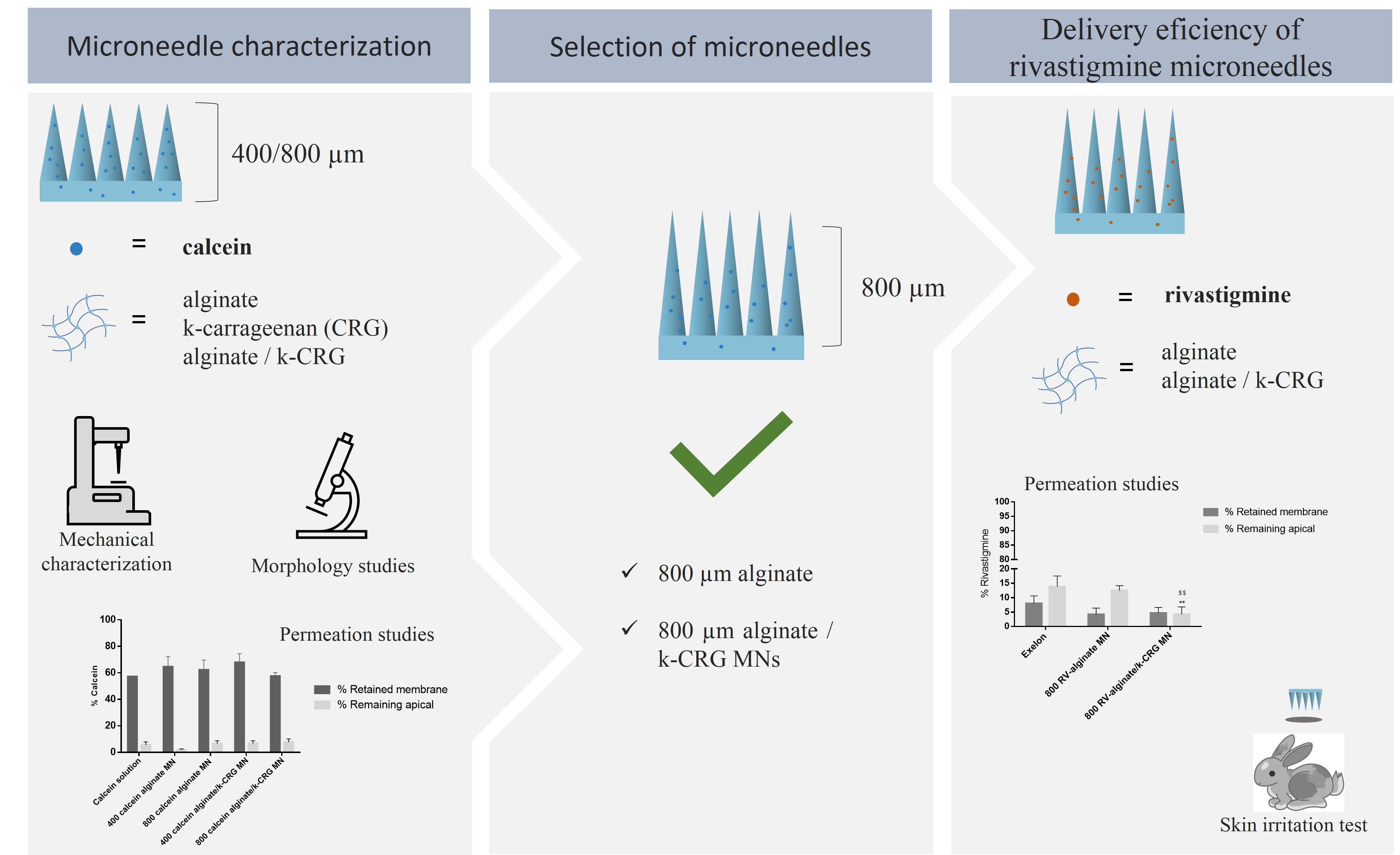
Polymeric Microneedles for Transdermal Delivery of Rivastigmine: Design and Application in Skin Mimetic Model

 ,
,  , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials and Instrumentation
2.2. Hydrogel Preparation
2.2.1. Preparation of the Alginate and k-Carrageenan Hydrogels
2.2.2. Preparation of the Drug-Loaded Hydrogels
2.3. Preparation and Optimisation of the Microneedles’ Fabrication Process
2.4. Characterisation of the Microneedle Devices
2.4.1. Topography Analysis—Scanning Electron Microscopy
2.4.2. Texture Analysis
2.5. Skin Permeation Studies
2.5.1. Quantification of Drug Permeation
2.5.2. Quantification of Drug Remaining in the Apical Compartment
2.5.3. Quantification of the Drug Retained in the Skin
2.5.4. Histology of the Skin
2.6. Skin Irritation Test
2.7. Statistical Analysis
3. Results and Discussion
3.1. Optimisation of Microneedle’s Production
3.1.1. Morphological Analysis
3.1.2. Texture Analysis
3.1.3. Permeation Assay
3.1.4. MNs Interaction with the Skin Assessed by Microscopy
3.2. Application of the Optimised Microneedles for Rivastigmine Transdermal Delivery
3.2.1. Morphological and Mechanical Characterisation
3.2.2. Skin Permeation Assay
3.2.3. Skin Irritation Test
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Duong, S.; Patel, T.; Chang, F. Dementia: What pharmacists need to know. Can. Pharm. J. 2017, 150, 118–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dening, T.; Sandilyan, M.B. Dementia: Definitions and types. Nurs. Stand. 2015, 29, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Birks, J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst. Rev. 2006, 1, Cd005593. [Google Scholar] [CrossRef]
- European Medicines Agency. Rivastigmine 1 A Pharma. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/rivastigmine-1-pharma (accessed on 27 October 2021).
- Sadowsky, C.; Perez, J.A.D.; Bouchard, R.W.; Goodman, I.; Tekin, S. Switching from Oral Cholinesterase Inhibitors to the Rivastigmine Transdermal Patch. CNS Neurosci. Ther. 2010, 16, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Sadowsky, C.H.; Micca, J.L.; Grossberg, G.T.; Velting, D.M. Rivastigmine from capsules to patch: Therapeutic advances in the management of Alzheimer’s disease and Parkinson’s disease dementia. Prim. Care Companion CNS Disord. 2014, 16, 27263. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Disease. Exelon® Patch (Rivastigmine Transdermal System) (n.d.). Exelon® Patch. Available online: https://www.exelonpatch.com/index.jsp (accessed on 27 October 2021).
- European Medicines Agency. Exelon. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/exelon (accessed on 27 October 2021).
- Small, G.; Dubois, B. A review of compliance to treatment in Alzheimer’s disease: Potential benefits of a transdermal patch. Curr. Med. Res. Opin. 2007, 23, 2705–2713. [Google Scholar] [CrossRef]
- Kurz, A.; Farlow, M.; Lefèvre, G. Pharmacokinetics of a novel transdermal rivastigmine patch for the treatment of Alzheimer’s disease: A review. Int. J. Clin. Pract. 2009, 63, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Chauhan, M.K.; Sharma, P.K. Optimization and characterization of rivastigmine nanolipid carrier loaded transdermal patches for the treatment of dementia. Chem. Phys. Lipids 2019, 224, 104794. [Google Scholar] [CrossRef]
- Cummings, J.L.; Farlow, M.R.; Meng, X.; Tekin, S.; Olin, J.T. Rivastigmine Transdermal Patch Skin Tolerability. Clin. Drug Investig. 2010, 30, 41–49. [Google Scholar] [CrossRef]
- Hanson, L.R.; Frey, W.H. Intranasal delivery bypasses the blood-brain barrier to target therapeutic agents to the central nervous system and treat neurodegenerative disease. BMC Neurosci. 2008, 9, S5. [Google Scholar] [CrossRef] [Green Version]
- Musumeci, T.; Pellitteri, R.; Spatuzza, M.; Puglisi, G. Nose-to-brain delivery: Evaluation of polymeric nanoparticles on olfactory ensheathing cells uptake. J. Pharm. Sci. 2014, 103, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Fazil, M.; Md, S.; Haque, S.; Kumar, M.; Baboota, S.; Sahni, J.K.; Ali, J. Development and evaluation of rivastigmine loaded chitosan nanoparticles for brain targeting. Eur. J. Pharm. Sci. 2012, 47, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Khunt, D.; Bhatt, H.; Misra, M.; Padh, H. Application of quality by design approach for intranasal delivery of rivastigmine loaded solid lipid nanoparticles: Effect on formulation and characterization parameters. Eur. J. Pharm. Sci. 2015, 78, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Vintiloiu, A.; Lafleur, M.; Bastiat, G.; Leroux, J.C. In situ-forming oleogel implant for rivastigmine delivery. Pharm. Res. 2008, 25, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gothwal, A.; Nakhate, K.T.; Alexander, A.; Ajazuddin; Gupta, U. Boosted Memory and Improved Brain Bioavailability of Rivastigmine: Targeting Effort to the Brain Using Covalently Tethered Lower Generation PAMAM Dendrimers with Lactoferrin. Mol. Pharm. 2018, 15, 4538–4549. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.F.; Elmeshad, A.N.; Salem, N.A. Potential therapeutic effect of nanobased formulation of rivastigmine on rat model of Alzheimer’s disease. Int. J. Nanomed. 2013, 8, 393–406. [Google Scholar] [CrossRef]
- Ravi, G.; Vishal Gupta, N.; Balamuralidhara, V. Rivastigmine Tartrate Solid Lipid Nanoparticles Loaded Transdermal Film: An in Vivo Study. Res. J. Pharm. Technol. 2018, 11, 227–230. [Google Scholar] [CrossRef]
- Cai, Y.; Tian, Q.; Liu, C.; Fang, L. Development of long-acting rivastigmine drug-in-adhesive patch utilizing ion-pair strategy and characterization of controlled release mechanism. Eur. J. Pharm. Sci. 2021, 161, 105774. [Google Scholar] [CrossRef]
- Yu, Z.-W.; Liang, Y.; Liang, W.-Q. Low-frequency sonophoresis enhances rivastigmine permeation in vitro and in vivo. Pharmazie 2015, 70, 379–380. [Google Scholar] [CrossRef]
- Waghule, T.; Singhvi, G.; Dubey, S.K.; Pandey, M.M.; Gupta, G.; Singh, M.; Dua, K. Microneedles: A smart approach and increasing potential for transdermal drug delivery system. Biomed. Pharmacother. 2019, 109, 1249–1258. [Google Scholar] [CrossRef]
- Chen, M.; Quan, G.; Sun, Y.; Yang, D.; Pan, X.; Wu, C. Nanoparticles-encapsulated polymeric microneedles for transdermal drug delivery. J. Control. Release 2020, 325, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Moniz, T.; Costa Lima, S.A.; Reis, S. Marine polymeric microneedles for transdermal drug delivery. Carbohydr. Polym. 2021, 266, 118098. [Google Scholar] [CrossRef] [PubMed]
- Alkilani, A.Z.; McCrudden, M.T.C.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the Stratum Corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, R.; Le, H.; Kiritsy, P.; Chuong, M.C. Formulation of Rivastigmine, a Liquid Drug Substance, for Use in a Simulating Study of Hollow Microstructured Transdermal Delivery System. J. Pharmacol. Pharm. Res. 2020, 3, 1–6. [Google Scholar] [CrossRef]
- Singh, P.; Carrier, A.; Chen, Y.; Lin, S.; Wang, J.; Cui, S.; Zhang, X. Polymeric microneedles for controlled transdermal drug delivery. J. Control. Release 2019, 315, 97–113. [Google Scholar] [CrossRef]
- Lee, J.W.; Han, M.R.; Park, J.H. Polymer microneedles for transdermal drug delivery. J. Drug Target 2013, 21, 211–223. [Google Scholar] [CrossRef]
- Barbosa, A.I.; Coutinho, A.J.; Costa Lima, S.A.; Reis, S. Marine Polysaccharides in Pharmaceutical Applications: Fucoidan and Chitosan as Key Players in the Drug Delivery Match Field. Mar. Drugs 2019, 17, 654. [Google Scholar] [CrossRef] [Green Version]
- Aravamudhan, A.; Ramos, D.M.; Nada, A.A.; Kumbar, S.G. Natural Polymers: Polysaccharides and Their Derivatives for Biomedical Applications. In Natural and Synthetic Biomedical Polymers; Kumbar, S.G., Laurencin, C.T., Deng, M., Eds.; Elsevier: Oxford, UK, 2014; pp. 67–89. [Google Scholar] [CrossRef]
- Chen, M.-C.; Ling, M.-H.; Lai, K.-Y.; Pramudityo, E. Chitosan Microneedle Patches for Sustained Transdermal Delivery of Macromolecules. Biomacromolecules 2012, 13, 4022–4031. [Google Scholar] [CrossRef]
- Dick, I.P.; Scott, R.C. Pig ear skin as an in-vitro model for human skin permeability. J. Pharm. Pharmacol. 1992, 44, 640–645. [Google Scholar] [CrossRef]
- Moniz, T.; Costa Lima, S.A.; Reis, S. Application of the human stratum corneum lipid-based mimetic model in assessment of drug-loaded nanoparticles for skin administration. Int. J. Pharm. 2020, 591, 119960. [Google Scholar] [CrossRef]
- Shakel, Z.; Nunes, C.; Costa Lima, S.A.; Reis, S. Development of a novel human stratum corneum model, as a tool in the optimization of drug formulations. Int. J. Pharm. 2019, 569, 118571. [Google Scholar] [CrossRef] [PubMed]
- ISO 10993-10:2010; Biological Evaluation of Medical Devices—Part 10: Tests for Irritation and Skin Sensitization. International Organization for Standardization: Geneva, Switzerland, 2010. Available online: https://www.iso.org/standard/40884.html (accessed on 27 October 2021).
- ISO 10993-2:2006; Biological Evaluation of Medical Devices—Part 2: Animal Welfare Requirements. International Organization for Standardization: Geneva, Switzerland, 2006. Available online: https://www.iso.org/standard/36405.html (accessed on 27 October 2021).
- Dathathri, E.; Lal, S.; Mittal, M.; Thakur, G.; De, S. Fabrication of low-cost composite polymer-based micro needle patch for transdermal drug delivery. Appl. Nanosci. 2020, 10, 371–377. [Google Scholar] [CrossRef]
- González-Vázquez, P.; Larrañeta, E.; McCrudden, M.T.C.; Jarrahian, C.; Rein-Weston, A.; Quintanar-Solares, M.; Zehrung, D.; McCarthy, H.; Courtenay, A.J.; Donnelly, R.F. Transdermal delivery of gentamicin using dissolving microneedle arrays for potential treatment of neonatal sepsis. J. Control. Release 2017, 265, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Sabri, A.H.; Kim, Y.; Marlow, M.; Scurr, D.J.; Segal, J.; Banga, A.K.; Kagan, L.; Lee, J.B. Intradermal and transdermal drug delivery using microneedles—Abrication, performance evaluation and application to lymphatic delivery. Adv. Drug Deliv. Rev. 2020, 153, 195–215. [Google Scholar] [CrossRef]
- Yang, S.; Feng, Y.; Zhang, L.; Chen, N.; Yuan, W.; Jin, T. A scalable fabrication process of polymer microneedles. Int. J. Nanomed. 2012, 7, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Jiang, G.; Zhang, Y.; Liu, D.; Xu, B.; Zhou, J. Polymer microneedles fabricated from alginate and hyaluronate for transdermal delivery of insulin. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 80, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; Singh, T.R.; Alkilani, A.Z.; McCrudden, M.T.; O’Neill, S.; O’Mahony, C.; Armstrong, K.; McLoone, N.; Kole, P.; Woolfson, A.D. Hydrogel-forming microneedle arrays exhibit antimicrobial properties: Potential for enhanced patient safety. Int. J. Pharm. 2013, 451, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Ohta, J.; Imada, K.; Akamatsu, S.; Tsuchida, N.; Inoue, G.; Inoue, N.; Takada, K. Dissolving microneedles to obtain rapid local anesthetic effect of lidocaine at skin tissue. J. Drug Target 2013, 21, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, P.; Kirkby, M.; Hutton, A.R.J.; Shabani, M.; Yiu, C.K.Y.; Baghbantaraghdari, Z.; Jamaledin, R.; Carlotti, M.; Mazzolai, B.; Mattoli, V.; et al. Engineering Microneedle Patches for Improved Penetration: Analysis, Skin Models and Factors Affecting Needle Insertion. Nano-Micro Lett. 2021, 13, 93. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef]
- Oh, J.H.; Park, H.H.; Do, K.Y.; Han, M.; Hyun, D.H.; Kim, C.G.; Kim, C.H.; Lee, S.S.; Hwang, S.J.; Shin, S.C.; et al. Influence of the delivery systems using a microneedle array on the permeation of a hydrophilic molecule, calcein. Eur. J. Pharm. Biopharm. 2008, 69, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Saju, A.; Cheerla, K.D.; Gade, S.K.; Garg, P.; Venuganti, V.V.K. Corneal delivery of besifloxacin using rapidly dissolving polymeric microneedles. Drug. Deliv. Transl. Res. 2018, 8, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Pattarabhiran, S.P.; Saju, A.; Sonawane, K.R.; Manimaran, R.; Bhatnagar, S.; Roy, G.; Kulkarni, R.B.; Venuganti, V.V.K. Dissolvable Microneedle-Mediated Transcutaneous Delivery of Tetanus Toxoid Elicits Effective Immune Response. AAPS PharmSciTech 2019, 20, 257. [Google Scholar] [CrossRef]
- Salatin, S.; Barar, J.; Barzegar-Jalali, M.; Adibkia, K.; Jelvehgari, M. Thermosensitive in situ nanocomposite of rivastigmine hydrogen tartrate as an intranasal delivery system: Development, characterization, ex vivo permeation and cellular studies. Colloids Surf. B: Biointerfaces 2017, 159, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Xing, M.; Yang, G.; Zhang, S.; Gao, Y. Acid-base combination principles for preparation of anti-acne dissolving microneedles loaded with azelaic acid and matrine. Eur. J. Pharm. Sci. 2021, 165, 105935. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method 1 | Method 2 | Method 3 | Method 4 | ||
|---|---|---|---|---|---|
| Number of layers |  2 layers |  2 layers |  2 layers |  4 layers | |
| Time | 3 days | 3 days | 3 days | 3 days | |
| Conditions per day | Day 1 | 50 mg; 3500 rpm; 30 °C; 1 h | 100 mg; 2500 rpm; 30 °C; 30 min | 50 mg; 500 rpm; 15 °C; 15 min | 25+25 mg; 3500 rpm; 30 °C; 1 h |
| Day 2 | 150 mg; 3500 rpm; 30 °C; 1 h | 50 mg; 500 rpm; 15 °C; 15 min | 100 mg; 500 rpm; 15 °C; 15 min | 50 mg; 3500 rpm; 30 °C; 1 h | |
| Day 3 | Incubation; 100 rpm; 25 °C; 3 h | Incubation; 150 rpm; 25 °C; 3 h | Incubation; 150 to 250 rpm; 25 °C; 2 h | 50 mg; 3500 rpm; 30 °C; 1 h | |
| Centrifugation; 500 rpm; 10 °C; 1 h | |||||
| Incubation; 150 rpm; 25 °C; 3 h | Incubation; 150 rpm; 25 °C; 3 h | ||||
| Observations | Visible Polymer loss. Possible overfilling of the micromould | Polymer loss detected after first-layer centrifugation | After detachment, no picks were visible | No significant polymer losses. Needles visible to the naked eye | |
| Type of MN | Force (N) 1 | Force/Needle |
|---|---|---|
| 400 µm alginate MN | 1.02 ± 0.20 | 0.51 |
| 800 µm alginate MN | 2.02 ± 0.29 **** | 1.01 |
| 400 µm Calcein-alginate MN | 1.30 ± 0.25 # | 0.65 |
| 800 µm Calcein-alginate MN | 1.65 ± 0.32 ***, ### | 0.83 |
| 400 µm alginate/k-CRG MN | 0.52 ± 0.12 | 0.26 |
| 800 µm alginate/k-CRG MN | 0.98 ± 0.22 **** | 0.49 |
| 400 µm Calcein-alginate/k-CRG MN | 0.45 ± 0.07 | 0.23 |
| 800 µm Calcein-alginate/k-CRG MN | 0.92 ± 0.16 **** | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guimarães, T.M.T.; Moniz, T.; Nunes, C.; Zaharieva, M.M.; Kaleva, M.; Yoncheva, K.; Najdenski, H.; Costa Lima, S.A.; Reis, S. Polymeric Microneedles for Transdermal Delivery of Rivastigmine: Design and Application in Skin Mimetic Model. Pharmaceutics 2022, 14, 752. https://doi.org/10.3390/pharmaceutics14040752
Guimarães TMT, Moniz T, Nunes C, Zaharieva MM, Kaleva M, Yoncheva K, Najdenski H, Costa Lima SA, Reis S. Polymeric Microneedles for Transdermal Delivery of Rivastigmine: Design and Application in Skin Mimetic Model. Pharmaceutics. 2022; 14(4):752. https://doi.org/10.3390/pharmaceutics14040752
Chicago/Turabian StyleGuimarães, Tânia M. T., Tânia Moniz, Cláudia Nunes, Maya Margaritova Zaharieva, Mila Kaleva, Krassimira Yoncheva, Hristo Najdenski, Sofia A. Costa Lima, and Salette Reis. 2022. "Polymeric Microneedles for Transdermal Delivery of Rivastigmine: Design and Application in Skin Mimetic Model" Pharmaceutics 14, no. 4: 752. https://doi.org/10.3390/pharmaceutics14040752