

Banked Primary Progenitor Cells for Allogeneic Intervertebral Disc (IVD) Therapy: Preclinical Qualification and Functional Optimization within a Cell Spheroid Formulation Process

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents and Consumables
2.2. Instruments and Equipment
2.3. Cell Sourcing and Cell Culture Media Composition
2.4. FE002-Disc Cellular Active Substance Preclinical Characterization Assays
2.4.1. Proteomic Composition Screening in Multiplex Analyses
2.4.2. Cell Surface Marker Characterization by Flow Cytometry
2.4.3. Phenotypic Stability Assessment in Chemical Induction Assays
2.4.4. β-Galactosidase Staining for In Vitro Cell Senescence Assessment
2.4.5. Telomerase Activity Quantification for In Vitro Tumorigenicity Assessment
2.4.6. Soft Agarose Colony Formation Assay for In Vitro Semi-Quantitative Tumorigenicity Assessment
2.4.7. Timecourse of HIF-1 Induction with Western Blotting Readout
2.4.8. Inflammatory Challenge Assays
2.5. FE002-Disc Cell Spheroid Manufacture Optimization and Functional Controls
2.5.1. Cell Spheroid Manufacture under Hypoxia
2.5.2. Cell Spheroid Cryopreservation and Lyophilization
2.5.3. DMMB Quantification for Assessment of ECM Deposition
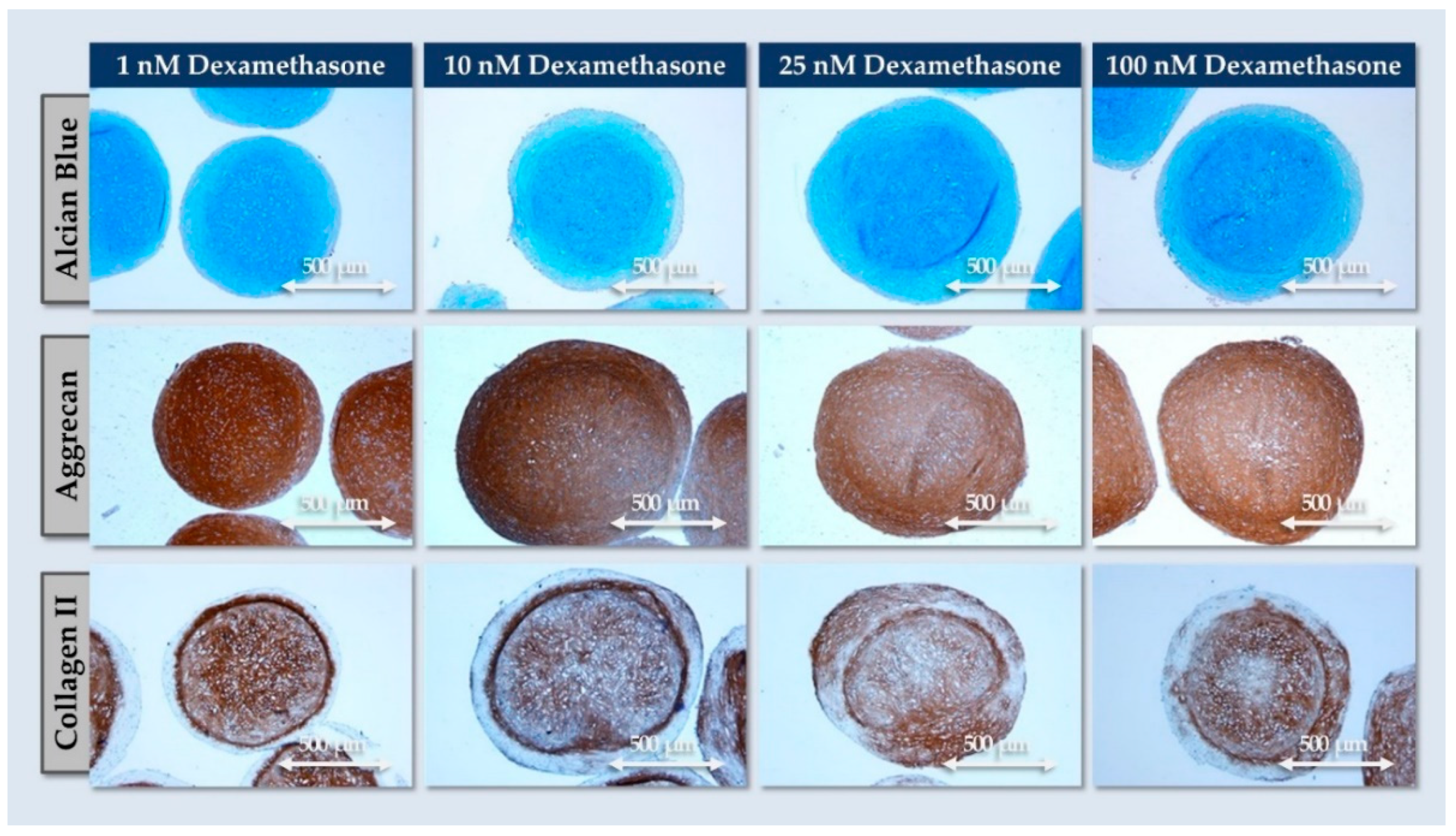
2.5.4. Western Blotting and Immunohistology for Specific ECM Component Visualization
2.6. Statistical Analysis and Data Presentation
3. Results
3.1. Identity and Compositional Attributes of the FE002-Disc Progenitor Cell Source
3.2. In Vitro Lifespan of FE002-Disc Progenitor Cells: Quality-Guided Selection of Appropriate Passage Levels
3.3. FE002-Disc Progenitor Cell Resilience in Hypoxic and Inflammatory Environments
3.4. FE002-Disc Progenitor Cell Source In Vitro Safety Characterization
3.5. FE002-Disc Cell Spheroid Formulation Process and Function-Guided Optimization
3.6. FE002-Disc Progenitor Cell Spheroid Stability in Cryopreservation and Lyopreservation
4. Discussion
4.1. Cell Therapies as Promising Contenders for IVD Pathology Management
- Safety attributes: absence of allergic or immunogenic reactions in the host, absence of tumorigenicity,
- Chondrogenic/discogenic potential: synthesis and deposition of GAGs and collagen II in the implantation environment,
- Cell sourcing: choice of discogenic cells (e.g., IVD cells, chondrocytes) with potent regeneration capacities and with environment modulatory attributes,
- Cellular resilience following implantation: in situ resistance to harsh environmental constraints in vivo,
- Supply chain considerations: allogeneic versus autologous starting biological materials,
- Adaptability to GMP manufacturing processes: possibility to prepare and formulate therapeutic cells in a clinically deliverable product.
4.2. Adequation of FE002-Disc Progenitor Cells with Cell Therapy Development Schemes
4.3. Importance of Therapeutic Cell Resilience in Hypoxic and Inflammatory Environments
4.4. Clinical Advancements of Chondrogenic Cells for IVD Therapy
4.5. Cell Formulation Optimization for Injectable IVD Treatments
4.6. Study Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AB | Alcian blue |
| ACAN | aggrecan |
| AF | annulus fibrosus |
| ASC | adipose-derived stem cells |
| ATMP | advanced therapy medicinal product |
| BCA | bicinchoninic acid |
| BMSC | bone marrow stromal cells |
| CD | cluster of differentiation |
| CH | Helvetic Confederation |
| CHUV | Centre hospitalier universitaire vaudois |
| CMtc | complete growth medium |
| COL | collagen |
| COMP | cartilage oligomeric matrix protein |
| CT | cycle threshold |
| DDD | degenerative disc disease |
| DMEM | Dulbecco’s modified Eagle medium |
| DMMB | dimethylmethylene blue assay |
| DMSO | dimethyl sulfoxide |
| DNA | deoxyribonucleic acid |
| EC | European Commission |
| ECL | electrochemiluminescence |
| ECM | extracellular matrix |
| FACS | fluorescence activated cell sorting |
| FBS | fetal bovine serum |
| FDA | US Food and Drug Administration |
| FGF | fibroblast growth factor |
| FITC | fluorescein isothiocyanate |
| GAG | glycosaminoglycan |
| GMP | good manufacturing practices |
| h | hour |
| HA | hyaluronic acid |
| HGF | hepatocyte growth factor |
| HIF-1 | hypoxia-inducible factor |
| HLA | human leukocyte antigen |
| HMGB1 | high mobility group protein B1 |
| HPL | human platelet lysate |
| HRP | horseradish peroxidase |
| IBMX | 3-isobutyl-1-methylxanthine |
| IL | interleukin |
| IPS | induced pluripotent stem cells |
| ITS | insulin, transferrin, selenous acid |
| IVD | intervertebral disc |
| IVDD | intervertebral disc disease |
| LBP | low back pain |
| M-CSF | macrophage colony-stimulating factor |
| min | minute |
| MMPs | matrix metalloproteinases |
| MoA | mechanism of action |
| MSC | mesenchymal stem cells |
| NA | non-applicable |
| NP | nucleus pulposus |
| NSAIDs | non-steroidal anti-inflammatory drugs |
| ODI | Oswestry disability index |
| PBS | phosphate-buffered saline |
| PDT | population doubling time |
| PDV | population doubling value |
| PE | phycoerythrin |
| PMSF | phenylmethylsulfonyl fluoride |
| PRP | platelet rich plasma |
| qPCR | quantitative polymerase chain reaction |
| TGF | transforming growth factor |
| TIMPs | tissue inhibitor of metalloproteinases |
| TNF | tumor necrosis factor |
| sEGFR | soluble epidermal growth factor receptor |
| sTNFRI | soluble tumor necrosis factor receptor I |
| UK | United Kingdom |
| USA | United States of America |
| USD | US dollar |
| VAS | visual analog scale |
| VASPI | visual analog scale pain intensity |
| VitCp | vitamin C 2-phosphate sesquimagnesium salt hydrate |
References
- Mohd Isa, I.L.; Teoh, S.L.; Mohd Nor, N.H.; Mokhtar, S.A. Discogenic low back pain: Anatomy, pathophysiology and treatments of intervertebral disc degeneration. Int. J. Mol. Sci. 2022, 24, 208. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ham, C.H.; Kwon, W.K. Current knowledge and future therapeutic prospects in symptomatic intervertebral disc degeneration. Yonsei Med. J. 2022, 63, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Soufi, K.H.; Castillo, J.A.; Rogdriguez, F.Y.; DeMesa, C.J.; Ebinu, J.O. Potential role for stem cell regenerative therapy as a treatment for degenerative disc disease and low back pain: A systematic review. Int. J. Mol. Sci. 2023, 24, 8893. [Google Scholar] [CrossRef] [PubMed]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M. Prevalence of chronic low back pain: Systematic review. Revista Saude Publ. 2015, 49, 1. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Zundert, J.V.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef]
- Dagenais, S.; Caro, J.; Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef]
- Binch, A.L.A.; Fitzgerald, J.C.; Growney, E.A.; Barry, F. Cell-based strategies for IVD repair: Clinical progress and translational obstacles. Nat. Rev. Rheumatol. 2021, 17, 158–175. [Google Scholar] [CrossRef]
- Freemont, A.J. The cellular pathobiology of the degenerate intervertebral disc and discogenic back pain. Rheumatology 2009, 48, 5–10. [Google Scholar] [CrossRef]
- Smith, L.J.; Silverman, L.; Sakai, D.; Le Maitre, C.L.; Mauck, R.L.; Malhotra, N.R.; Lotz, J.C.; Buckley, C.T. Advancing cell therapies for intervertebral disc regeneration from the lab to the clinic: Recommendations of the ORS spine section. JOR Spine 2018, 1, e1036. [Google Scholar] [CrossRef]
- Sharifi, S.; Bulstra, S.K.; Grijpma, D.W.; Kuijer, R. Treatment of the degenerated intervertebral disc; closure, repair and regeneration of the annulus fibrosus. J. Tissue Eng. Regen. Med. 2015, 9, 1120–1132. [Google Scholar] [CrossRef] [PubMed]
- Vo, N.V.; Hartman, R.A.; Yurube, T.; Jacobs, L.J.; Sowa, G.A.; Kang, J.D. Expression and regulation of metalloproteinases and their inhibitors in intervertebral disc aging and degeneration. Spine J. 2013, 13, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Nicol, V.; Verdaguer, C.; Daste, C.; Bisseriex, H.; Lapeyre, É.; Lefèvre-Colau, M.M.; Rannou, F.; Rören, A.; Facione, J.; Nguyen, C. Chronic low back pain: A narrative review of recent international guidelines for diagnosis and conservative treatment. J. Clin. Med. 2023, 12, 1685. [Google Scholar] [CrossRef] [PubMed]
- Pennicooke, B.; Moriguchi, Y.; Hussain, I.; Bonssar, L.; Härtl, R. Biological treatment approaches for degenerative disc disease: A review of clinical trials and future directions. Cureus 2016, 8, e892. [Google Scholar] [CrossRef]
- Fritzell, P.; Hägg, O.; Wessberg, P.; Nordwall, A.; Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001, 26, 2521–2534. [Google Scholar] [CrossRef]
- Mowbray, J.; Shen, B.; Diwan, A.D. Intradiscal therapeutics for degenerative disc disease. In Handbook of Spine Technology; Springer International Publishing: Cham, Switzerland, 2021; pp. 1091–1110. [Google Scholar]
- Clinical Trial N°NCT01124006. A Multicenter, Randomized, Double-Blind, Placebo Controlled, Clinical Trial to Evaluate the Safety, Tolerability and Preliminary Effectiveness of 2 Doses of Intradiscal rhGDF-5 (Single Administration) for the Treatment of Early Stage Lumbar Disc Degeneration. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT01124006 (accessed on 7 May 2024).
- Clinical Trial N°NCT03122119. Effectiveness of Ultrasound Guided Platelet Rich Plasma Injections in the Sacroiliac Joint. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT03122119 (accessed on 7 May 2024).
- Zhang, J.; Liu, D.; Gong, Q.; Chen, J.; Wan, L. Intradiscal autologous platelet-rich plasma injection for discogenic low back pain: A clinical trial. BioMed Res. Int. 2022, 2022, 9563693. [Google Scholar] [CrossRef]
- Clinical Trial N°NCT03955315. Study to Evaluate the Safety and Preliminary Efficacy of IDCT, a Treatment for Symptomatic Lumbar Disc Degeneration. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT03955315 (accessed on 7 May 2024).
- Tschugg, A.; Michnacs, F.; Strowitzki, M.; Meisel, H.J.; Thomé, C. A prospective multicenter phase I/II clinical trial to evaluate safety and efficacy of NOVOCART Disc plus autologous disc chondrocyte transplantation in the treatment of nucleotomized and degenerative lumbar disc to avoid secondary disease: Study protocol for a randomized controlled trial. Trials 2016, 17, 108. [Google Scholar] [CrossRef]
- Amirdelfan, K.; Bae, H.; McJunkin, T.; DePalma, M.; Kim, K.; Beckworth, W.J.; Ghiselli, G.; Bainbridge, J.S.; Dryer, R.; Deer, T.R.; et al. Allogeneic mesenchymal precursor cells treatment for chronic low back pain associated with degenerative disc disease: A prospective randomized, placebo-controlled 36-month study of safety and efficacy. Spine J. 2021, 21, 212–230. [Google Scholar] [CrossRef]
- Gjefsen, E.; Bråten, L.C.H.; Goll, G.L.; Wigemyr, M.; Bolstad, N.; Valberg, M.; Schistad, E.I.; Marchand, G.H.; Granviken, F.; Selmer, K.K.; et al. The effect of infliximab in patients with chronic low back pain and Modic changes (the BackToBasic study): Study protocol of a randomized, double blind, placebo-controlled, multicenter trial. BMC Musculoskel. Dis. 2020, 21, 698. [Google Scholar] [CrossRef]
- Han, F.; Tu, Z.; Zhu, Z.; Liu, D.; Meng, Q.; Yu, Q.; Wang, Y.; Chen, J.; Liu, T.; Han, F.; et al. Targeting endogenous reactive oxygen species removal and regulating regenerative microenvironment at annulus fibrosus defects promote tissue repair. ACS Nano 2023, 17, 7645–7661. [Google Scholar] [CrossRef]
- Wei, Z.; Ye, H.; Li, Y.; Li, X.; Liu, Y.; Chen, Y.; Yu, J.; Wang, J.; Ye, X. Mechanically tough, adhesive, self-healing hydrogel promotes annulus fibrosus repair via autologous cell recruitment and microenvironment regulation. Acta Biomater. 2024, 178, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Herger, N.; Bermudez-Lekerika, P.; Farshad, M.; Albers, C.E.; Distler, O.; Gantenbein, B.; Dudli, S. Should degenerated intervertebral discs of patients with modic type 1 changes be treated with mesenchymal stem cells? Int. J. Mol. Sci. 2022, 23, 2721. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Andersson, G.B. Stem cell therapy for intervertebral disc regeneration: Obstacles and solutions. Nat. Rev. Rheumatol. 2015, 11, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Schol, J. Cell therapy for intervertebral disc repair: Clinical perspective. J. Orthop. Transl. 2017, 9, 8–18. [Google Scholar] [CrossRef]
- Meisel, H.J.; Siodla, V.; Ganey, T.; Minkus, Y.; Hutton, W.C.; Alasevic, O.J. Clinical experience in cell-based therapeutics: Disc chondrocyte transplantation. A treatment for degenerated or damaged intervertebral disc. Biomol. Eng. 2007, 24, 5–21. [Google Scholar] [CrossRef]
- Meisel, H.J.; Ganey, T.; Hutton, W.C.; Libera, J.; Minkus, Y.; Alasevic, O. Clinical experience in cell-based therapeutics: Intervention and outcome. Eur. Spine J. 2006, 15, S397–S405. [Google Scholar] [CrossRef]
- Krut, Z.; Pelled, G.; Gazit, D.; Gazit, Z. Stem cells and exosomes: New therapies for intervertebral disc degeneration. Cells 2021, 10, 2241. [Google Scholar] [CrossRef]
- Li, Z.; Wu, Y.; Tan, G.; Xu, Z.; Xue, H. Exosomes and exosomal miRNAs: A new therapy for intervertebral disc degeneration. Front. Pharmacol. 2022, 13, 992476. [Google Scholar] [CrossRef]
- Laurent, A.; Hirt-Burri, N.; Scaletta, C.; Michetti, M.; de Buys Roessingh, A.S.; Raffoul, W.; Applegate, L.A. Holistic approach of Swiss fetal progenitor cell banking: Optimizing safe and sustainable substrates for regenerative medicine and biotechnology. Front. Bioeng. Biotechnol. 2020, 8, 557758. [Google Scholar] [CrossRef]
- Philippe, V.; Jeannerat, A.; Peneveyre, C.; Jaccoud, S.; Scaletta, C.; Hirt-Burri, N.; Abdel-Sayed, P.; Raffoul, W.; Darwiche, S.; Applegate, L.A.; et al. Autologous and allogeneic cytotherapies for large knee (osteo)chondral defects: Manufacturing process benchmarking and parallel functional qualification. Pharmaceutics 2023, 15, 2333. [Google Scholar] [CrossRef]
- Darwiche, S.; Scaletta, C.; Raffoul, W.; Pioletti, D.P.; Applegate, L.A. Epiphyseal chondroprogenitors provide a stable cell source for cartilage cell therapy. Cell Med. 2012, 4, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Shang, Y.; Yu, J.; Zeng, X.; Lin, J.; Tu, M.; Cheang, L.H.; Zhang, J. Regenerative potential of human nucleus pulposus resident stem/progenitor cells declines with ageing and intervertebral disc degeneration. Int. J. Mol. Med. 2018, 42, 2193–2202. [Google Scholar] [CrossRef] [PubMed]
- Mabotuwana, N.S.; Rech, L.; Lim, J.; Hardy, S.A.; Murtha, L.A.; Rainer, P.P.; Boyle, A.J. Paracrine factors released by stem cells of mesenchymal origin and their effects in cardiovascular disease: A systematic review of pre-clinical studies. Stem Cell Rev. Rep. 2022, 18, 2606–2628. [Google Scholar] [CrossRef] [PubMed]
- Hung, G.; Ashvetiya, T.; Leszczynska, A.; Yang, W.; Hwang, C.W.; Gerstenblith, G.; Barth, A.S.; Johnston, P.V. Paracrine-mediated rejuvenation of aged mesenchymal stem cells is associated with downregulation of the autophagy-lysosomal pathway. Npj Aging 2022, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Jarrige, M.; Frank, E.; Herardot, E.; Martineau, S.; Darle, A.; Benabides, M.; Domingues, S.; Chose, O.; Habeler, W.; Lorant, J.; et al. The future of regenerative medicine: Cell therapy using pluripotent stem cells and acellular therapies based on extracellular vesicles. Cells 2021, 10, 240. [Google Scholar] [CrossRef]
- Wang, C.; Yu, X.; Yan, Y.; Yang, W.; Zhang, S.; Xiang, Y.; Zhang, J.; Wang, W. Tumor necrosis factor-α: A key contributor to intervertebral disc degeneration. Acta Biochim. Biophys. Sin. 2017, 49, 1–13. [Google Scholar] [CrossRef]
- Croft, A.S.; Guerrero, J.; Oswald, K.A.C.; Häckel, S.; Albers, C.E.; Gantenbein, B. Effect of different cryopreservation media on human nucleus pulposus cells’ viability and trilineage potential. JOR Spine 2021, 4, e1140. [Google Scholar] [CrossRef]
- Evenbratt, H.; Andreasson, L.; Bicknell, V.; Brittberg, M.; Mobini, R.; Simonsson, S. Insights into the present and future of cartilage regeneration and joint repair. Cell Regen. 2022, 11, 3. [Google Scholar] [CrossRef]
- Feng, G.; Li, L.; Liu, H.; Song, Y.; Huang, F.; Tu, C.; Shen, B.; Gong, Q.; Li, T.; Liu, L.; et al. Hypoxia differentially regulates human nucleus pulposus and annulus fibrosus cell extracellular matrix production in 3D scaffolds. Osteoarthr. Cart. 2013, 21, 582–588. [Google Scholar] [CrossRef]
- Bitterli, T.; Schmid, D.; Ettinger, L.; Krupkova, O.; Bach, F.C.; Tryfonidou, M.A.; Meij, B.P.; Pozzi, A.; Steffen, F.; Wuertz-Kozak, K.; et al. Targeted screening of inflammatory mediators in spontaneous degenerative disc disease in dogs reveals an upregulation of the tumor necrosis superfamily. JOR Spine 2023, 7, e1292. [Google Scholar] [CrossRef]
- Fan, C.; Wang, W.; Yu, Z.; Wang, J.; Xu, W.; Ji, Z.; He, W.; Hua, D.; Wang, W.; Yao, L.; et al. M1 macrophage-derived exosomes promote intervertebral disc degeneration by enhancing nucleus pulposus cell senescence through LCN2/NF-κB signaling axis. J. Nanobiotechnol. 2024, 22, 301. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Li, H.; Guo, S.; Wang, C.; Long, L.; Wang, X.; Shi, H.; Zhang, K.; Chen, H.; Li, S. The mechanisms and functions of TNF-α in intervertebral disc degeneration. Exp. Gerontol. 2023, 174, 112119. [Google Scholar] [CrossRef] [PubMed]
- Díaz, L.; Zambrano, E.; Flores, M.E.; Contreras, M.; Crispín, J.C.; Alemán, G.; Bravo, C.; Armenta, A.; Valdés, V.J.; Tovar, A.; et al. Ethical considerations in animal research: The principle of 3R’s. Rev. Investig. Clin. 2020, 73, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Jeannerat, A.; Meuli, J.; Peneveyre, C.; Jaccoud, S.; Chemali, M.; Thomas, A.; Liao, Z.; Abdel-Sayed, P.; Scaletta, C.; Hirt-Burri, N.; et al. Bio-enhanced neoligaments graft bearing FE002 primary progenitor tenocytes: Allogeneic tissue engineering & surgical proofs-of-concept for hand ligament regenerative medicine. Pharmaceutics 2023, 15, 1873. [Google Scholar] [CrossRef] [PubMed]
- Mumme, M.; Barbero, A.; Miot, S.; Wixmerten, A.; Feliciano, S.; Wolf, F.; Asnaghi, A.M.; Baumhoer, D.; Bieri, O.; Kretzcchmar, M.; et al. Nasal chondrocyte-based engineered autologous cartilage tissue for repair of articular cartilage defects: An observational first-in-human trial. Lancet 2016, 388, 1985–1994. [Google Scholar] [CrossRef]
- Almqvist, K.F.; Dhollander, A.A.; Verdonk, P.C.; Forsyth, R.; Verdonk, R.; Verbruggen, G. Treatment of cartilage defects in the knee using alginate beads containing human mature allogenic chondrocytes. Am. J. Sports Med. 2009, 37, 1920–1929. [Google Scholar] [CrossRef]
- Kutaish, H.; Tscholl, P.M.; Cosset, E.; Bengtsson, L.; Braunersreuther, V.; Mor, F.M.; Laedermann, J.; Furfaro, I.; Stafylakis, D.; Hannouche, D.; et al. Articular cartilage repair after implantation of hyaline cartilage beads engineered from adult dedifferentiated chondrocytes: Cartibeads preclinical efficacy study in a large animal model. Am. J. Sports Med. 2023, 51, 237–249. [Google Scholar] [CrossRef]
- Gay, M.H.; Mehrkens, A.; Rittmann, M.; Haug, M.; Barbero, A.; Martin, I.; Schaeren, S. Nose to back: Compatibility of nasal chondrocytes with environmental conditions mimicking a degenerated intervertebral disc. Eur. Cells Mater. 2019, 37, 214–232. [Google Scholar] [CrossRef]
- Gryadunova, A.; Kasamkattil, J.; Gay, M.H.P.; Dasen, B.; Pelttari, K.; Mironov, V.; Martin, I.; Schären, S.; Barbero, A.; Krupkova, O.; et al. Nose to spine: Spheroids generated by human nasal chondrocytes for scaffold-free nucleus pulposus augmentation. Acta Biomater. 2021, 134, 240–251. [Google Scholar] [CrossRef]
- Kasamkattil, J.; Gryadunova, A.; Martin, I.; Barbero, A.; Schären, S.; Krupkova, O.; Mehrkens, A. Spheroid-based tissue engineering strategies for regeneration of the intervertebral disc. Int. J. Mol. Sci. 2022, 23, 2530. [Google Scholar] [CrossRef]
- Kasamkattil, J.; Gryadunova, A.; Schmid, R.; Gay-Dujak, M.H.P.; Dasen, B.; Hilpert, M.; Pelttari, K.; Martin, I.; Schären, S.; Barbero, A.; et al. Human 3D nucleus pulposus microtissue model to evaluate the potential of pre-conditioned nasal chondrocytes for the repair of degenerated intervertebral disc. Front. Bioeng. Biotechnol. 2023, 11, 1119009. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, E.E.; Wilson, N.; Barcellona, M.N.; Ní Néill, T.; Bagnall, J.; Brama, P.A.J.; Cunniffe, G.M.; Darwish, S.L.; Butler, J.S.; Buckley, C.T. Preclinical to clinical translation for intervertebral disc repair: Effects of species-specific scale, metabolism, and matrix synthesis rates on cell-based regeneration. JOR Spine 2023, 6, e1279. [Google Scholar] [CrossRef] [PubMed]
- Martinez, I.; Elvenes, J.; Olsen, R.; Bertheussen, K.; Johansen, O. Redifferentiation of in vitro expanded adult articular chondrocytes by combining the hanging-drop cultivation method with hypoxic environment. Cell Transplant. 2008, 17, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Chijimatsu, R.; Kobayashi, M.; Ebina, K.; Iwahashi, T.; Okuno, Y.; Hirao, M.; Fukuhara, A.; Nakamura, N.; Yoshikawa, H. Impact of dexamethasone concentration on cartilage tissue formation from human synovial derived stem cells in vitro. Cytotechnology 2018, 70, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Demoor, M.; Ollitrault, D.; Gomez-Leduc, T.; Bouyoucef, M.; Hervieu, M.; Fabre, H.; Lafont, J.; Denoix, J.M.; Audigié, F.; Mallein-Gerin, F.; et al. Cartilage tissue engineering: Molecular control of chondrocyte differentiation for proper cartilage matrix reconstruction. Biochim. Biophys. Acta 2014, 1840, 2414–2440. [Google Scholar] [CrossRef]
- Branly, T.; Contentin, R.; Desancé, M.; Jacquel, T.; Bertoni, L.; Jacquet, S.; Mallein-Gerin, F.; Denoix, J.M.; Audigié, F.; Demoor, M.; et al. Improvement of the chondrocyte-specific phenotype upon equine bone marrow mesenchymal stem cell differentiation: Influence of culture time, transforming growth factors and type i collagen siRNAs on the differentiation index. Int. J. Mol. Sci. 2018, 19, 435. [Google Scholar] [CrossRef]
- Gómez-Leduc, T.; Desancé, M.; Hervieu, M.; Legendre, F.; Ollitrault, D.; de Vienne, C.; Herlicoviez, M.; Galéra, P.; Demoor, M. Hypoxia is a critical parameter for chondrogenic differentiation of human umbilical cord blood mesenchymal stem cells in type I/III collagen sponges. Int. J. Mol. Sci. 2017, 18, 1933. [Google Scholar] [CrossRef]
- Enochson, L.; Brittberg, M.; Lindahl, A. Optimization of a chondrogenic medium through the use of factorial design of experiments. BioRes. Open Access 2012, 1, 306–313. [Google Scholar] [CrossRef]
- Kipnes, J.; Carlberg, A.L.; Loredo, G.A.; Lawler, J.; Tuan, R.S.; Hall, D.J. Effect of cartilage oligomeric matrix protein on mesenchymal chondrogenesis in vitro. Osteoarthr. Cart. 2003, 11, 442–454. [Google Scholar] [CrossRef]
- Shi, P.; Chee, A.; Liu, W.; Chou, P.H.; Zhu, J.; An, H.S. Therapeutic effects of cell therapy with neonatal human dermal fibroblasts and rabbit dermal fibroblasts on disc degeneration and inflammation. Spine J. 2019, 19, 171–181. [Google Scholar] [CrossRef]
- Farhang, N.; Silverman, L.; Bowles, R.D. Improving cell therapy survival and anabolism in harsh musculoskeletal disease environments. Tissue Eng. Part B Rev. 2020, 26, 348–366. [Google Scholar] [CrossRef] [PubMed]
- Tschugg, A.; Diepers, M.; Simone, S.; Michnacs, F.; Quirbach, S.; Strowitzki, M.; Meisel, H.J.; Thomé, C. A prospective randomized multicenter phase I/II clinical trial to evaluate safety and efficacy of NOVOCART disk plus autologous disk chondrocyte transplantation in the treatment of nucleotomized and degenerative lumbar disks to avoid secondary disease: Safety results of Phase I—A short report. Neurosurg. Rev. 2017, 40, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hiraishi, S.; Schol, J.; Sakai, D.; Nukaga, T.; Erickson, I.; Silverman, L.; Foley, K.; Watanabe, M. Discogenic cell transplantation directly from a cryopreserved state in an induced intervertebral disc degeneration canine model. JOR Spine 2018, 1, e1013. [Google Scholar] [CrossRef] [PubMed]
- Silverman, L.I.; Heaton, W.; Farhang, N.; Saxon, L.H.; Dulatova, G.; Rodriguez-Granrose, D.; Flanagan, F.; Foley, K.T. Perspectives on the treatment of lumbar disc degeneration: The value proposition for a cell-based therapy, immunomodulatory properties of discogenic cells and the associated clinical evaluation strategy. Front. Surg. 2020, 7, 554382. [Google Scholar] [CrossRef]
- Silverman, L.I.; Flanagan, F.; Rodriguez-Granrose, D.; Simpson, K.; Saxon, L.H.; Foley, K.T. Identifying and managing sources of variability in cell therapy manufacturing and clinical trials. Regen. Eng. Transl. Med. 2019, 5, 354–361. [Google Scholar] [CrossRef]
- Rodriguez-Granrose, D.; Zurawski, J.; Heaton, W.; Tandeski, T.; Dulatov, G.; Highsmith, A.A.; Conen, M.; Clark, G.; Jones, A.; Loftus, H.; et al. Transition from static culture to stirred tank bioreactor for the allogeneic production of therapeutic discogenic cell spheres. Stem Cell Res. Ther. 2021, 12, 455. [Google Scholar] [CrossRef]
- Chae, S.; Hong, J.; Hwangbo, H.; Kim, G. The utility of biomedical scaffolds laden with spheroids in various tissue engineering applications. Theranostics 2021, 11, 6818–6832. [Google Scholar] [CrossRef]
- Silverman, L.I.; Dulatova, G.; Tandeski, T.; Erickson, I.E.; Lundell, B.; Toplon, D.; Wolff, T.; Howard, A.; Chintalacharuvu, S.; Foley, K.T. In vitro and in vivo evaluation of discogenic cells, an investigational cell therapy for disc degeneration. Spine J. 2020, 20, 138–149. [Google Scholar] [CrossRef]
- Yoon, K.H.; Yoo, J.D.; Choi, C.H.; Lee, J.; Lee, J.Y.; Kim, S.G.; Park, J.Y. Costal chondrocyte-derived pellet-type autologous chondrocyte implantation versus microfracture for repair of articular cartilage defects: A prospective randomized trial. Cartilage 2021, 13, 1092S–1104S. [Google Scholar] [CrossRef]
- Yoon, K.H.; Park, J.Y.; Lee, J.Y.; Lee, E.; Lee, J.; Kim, S.G. Costal chondrocyte-derived pellet-type autologous chondrocyte implantation for treatment of articular cartilage defect. Am. J. Sports Med. 2020, 48, 1236–1245. [Google Scholar] [CrossRef]
- Teixeira, G.Q.; Riegger, J.; Gonçalves, R.M.; Risbud, M.V. Editorial: Intervertebral disc degeneration and osteoarthritis: Mechanisms of disease and functional repair. Front. Bioeng. Biotechnol. 2023, 11, 1252703. [Google Scholar] [CrossRef] [PubMed]
- Tonomura, H.; Nagae, M.; Takatori, R.; Ishibashi, H.; Itsuji, T.; Takahashi, K. The potential role of hepatocyte growth factor in degenerative disorders of the synovial joint and spine. Int. J. Mol. Sci. 2020, 21, 8717. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Wang, H.C.; Li, H.; Tao, Y.Q.; Liang, C.Z.; Li, F.C.; Chen, G.; Chen, Q.X. Nucleus pulposus mesenchymal stem cells in acidic conditions mimicking degenerative intervertebral discs give better performance than adipose tissue-derived mesenchymal stem cells. Cells Tissues Org. 2014, 199, 342–352. [Google Scholar] [CrossRef]
- Scotti, C.; Osmokrovic, A.; Wolf, F.; Miot, S.; Peretti, G.M.; Barbero, A.; Martin, I. Response of human engineered cartilage based on articular or nasal chondrocytes to interleukin-1β and low oxygen. Tissue Eng. Part A 2012, 18, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Jeannerat, A.; Peneveyre, C.; Armand, F.; Chiappe, D.; Hamelin, R.; Scaletta, C.; Hirt-Burri, N.; de Buys Roessingh, A.; Raffoul, W.; Applegate, L.A.; et al. Hypoxic incubation conditions for optimized manufacture of tenocyte-based active pharmaceutical ingredients of homologous standardized transplant products in tendon regenerative medicine. Cells 2021, 10, 2872. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trial N°NCT02412735. Placebo-Controlled Study to Evaluate Rexlemestrocel-L Alone or Combined with Hyaluronic Acid in Participants with Chronic Low Back Pain (MSB-DR003). Available online: https://clinicaltrials.gov/study/NCT02412735 (accessed on 11 July 2024).
- Beall, D.P.; Davis, T.; DePalma, M.J.; Amirdelfan, K.; Yoon, E.S.; Wilson, G.L.; Bishop, R.; Tally, W.C.; Gershon, S.L.; Lorio, M.P.; et al. Viable disc tissue allograft supplementation; One- and two-level treatment of degenerated intervertebral discs in patients with chronic discogenic low back pain: One year results of the VAST randomized controlled trial. Pain Phys. 2021, 24, 465–477. [Google Scholar]
- Lorio, M.P.; Tate, J.L.; Myers, T.J.; Block, J.E.; Beall, D.P. Perspective on intradiscal therapies for lumbar discogenic pain: State of the science, knowledge gaps, and imperatives for clinical adoption. J. Pain Res. 2024, 17, 1171–1182. [Google Scholar] [CrossRef]
- Noriega, D.C.; Ardura, F.; Hernández-Ramajo, R.; Martín-Ferrero, M.Á.; Sánchez-Lite, I.; Toribio, B.; Alberca, M.; García, V.; Moraleda, J.M.; González-Vallinas, M.; et al. Treatment of degenerative disc disease with allogeneic mesenchymal stem cells: Long-term follow-up results. Transplantation 2021, 105, e25–e27. [Google Scholar] [CrossRef]
- Clinical Trial N°NCT04530071. Evaluation of Safety, Tolerability, and Efficacy of CordSTEM-DD in Patients with Chronic Low Back Pain. Available online: https://www.clinicaltrials.gov/study/NCT04530071 (accessed on 11 June 2024).
- Noriega, D.C.; Ardura, F.; Hernández-Ramajo, R.; Martín-Ferrero, M.Á.; Sánchez-Lite, I.; Toribio, B.; Alberca, M.; García, V.; Moraleda, J.M.; Sánchez, A.; et al. Intervertebral disc repair by allogeneic mesenchymal bone marrow cells: A randomized controlled trial. Transplantation 2017, 101, 1945–1951. [Google Scholar] [CrossRef]
- Elabd, C.; Centeno, C.J.; Schultz, J.R.; Lutz, G.; Ichim, T.; Silva, F.J. Intra-discal injection of autologous, hypoxic cultured bone marrow-derived mesenchymal stem cells in five patients with chronic lower back pain: A long-term safety and feasibility study. J. Transl. Med. 2016, 14, 253. [Google Scholar] [CrossRef]
- Horizon 2020 Project. Regenerative Therapy of Intervertebral Disc: A Double Blind Phase 2b Trial of Intradiscal Injection of Mesenchymal Stromal Cells in Degenerative Disc Disease of the Lomber SPINE Unresponsive to Conventional Therapy. Available online: https://cordis.europa.eu/project/id/732163/results (accessed on 11 June 2024).
- Yan, X.; Zhou, L.; Wu, Z.; Wang, X.; Chen, X.; Yang, F.; Guo, Y.; Wu, M.; Chen, Y.; Li, W.; et al. High throughput scaffold-based 3D micro-tumor array for efficient drug screening and chemosensitivity testing. Biomaterials 2019, 198, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Flampouri, E.; Imar, S.; OConnell, K.; Singh, B. Spheroid-3D and monolayer-2D intestinal electrochemical biosensor for toxicity/viability testing: Applications in drug screening, food safety, and environmental pollutant analysis. ACS Sens. 2019, 4, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Eschen, C.; Kaps, C.; Widuchowski, W.; Fickert, S.; Zinser, W.; Niemeyer, P.; Roël, G. Clinical outcome is significantly better with spheroid-based autologous chondrocyte implantation manufactured with more stringent cell culture criteria. Osteoarthr. Cart. Open 2020, 2, 100033. [Google Scholar] [CrossRef] [PubMed]
- Ikawa, T.; Yano, K.; Watanabe, N.; Masamune, K.; Yamato, M. Non-clinical assessment design of autologous chondrocyte implantation products. Regen. Ther. 2015, 1, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Bukovac, P.K.; Hauser, M.; Lottaz, D.; Marti, A.; Schmitt, I.; Schochat, T. The regulation of cell therapy and gene therapy products in Switzerland. Adv. Exp. Med. Biol. 2023, 1430, 41–58. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Song, S.Y.; Kim, E. Advanced therapy medicinal products for autologous chondrocytes and comparison of regulatory systems in target countries. Regen. Ther. 2022, 20, 126–137. [Google Scholar] [CrossRef]
- Nordberg, R.C.; Otarola, G.A.; Wang, D.; Hu, J.C.; Athanasiou, K.A. Navigating regulatory pathways for translation of biologic cartilage repair products. Sci. Transl. Med. 2022, 14, eabp8163. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Circularity | Feret’s Diameter (mm) | Roundness | |||
|---|---|---|---|---|---|---|
| Dexamethasone Concentration (nM) | 10 nM | 100 nM | 10 nM | 100 nM | 10 nM | 100 nM |
| D7 Timepoint | 0.47 ± 0.12 | 0.56 ± 0.10 | 0.98 ± 0.05 | 0.97 ± 0.02 | 0.95 ± 0.02 | 0.96 ± 0.01 |
| D14 Timepoint | 0.42 ± 0.16 | 0.46 ± 0.08 | 1.09 ± 0.02 | 1.08 ± 0.05 | 0.96 ± 0.02 | 0.97 ± 0.02 |
| D21 Timepoint | 0.51 ± 0.08 | 0.54 ± 0.08 | 1.19 ± 0.02 | 1.24 ± 0.10 | 0.96 ± 0.01 | 0.88 ± 0.05 |
| Clinical Trial 1 | Spheroids/Cell Type | Therapeutic Indications |
|---|---|---|
| NCT04262167 | Autologous lung stem cells | Idiopathic pulmonary fibrosis |
| NCT04945018 | Allogenic IPS cardiomyocytes | Heart failure |
| NCT05011474 | Autologous matrillin-3 pre-treated ASCs | Disc degeneration |
| NCT05712148 | MSCs | Retinitis pigmentosa |
| NCT04818203 | Autologous dermal fibroblasts | Periorbital wrinkles |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeannerat, A.; Peneveyre, C.; Jaccoud, S.; Philippe, V.; Scaletta, C.; Hirt-Burri, N.; Abdel-Sayed, P.; Martin, R.; Applegate, L.A.; Pioletti, D.P.; et al. Banked Primary Progenitor Cells for Allogeneic Intervertebral Disc (IVD) Therapy: Preclinical Qualification and Functional Optimization within a Cell Spheroid Formulation Process. Pharmaceutics 2024, 16, 1274. https://doi.org/10.3390/pharmaceutics16101274
Jeannerat A, Peneveyre C, Jaccoud S, Philippe V, Scaletta C, Hirt-Burri N, Abdel-Sayed P, Martin R, Applegate LA, Pioletti DP, et al. Banked Primary Progenitor Cells for Allogeneic Intervertebral Disc (IVD) Therapy: Preclinical Qualification and Functional Optimization within a Cell Spheroid Formulation Process. Pharmaceutics. 2024; 16(10):1274. https://doi.org/10.3390/pharmaceutics16101274
Chicago/Turabian StyleJeannerat, Annick, Cédric Peneveyre, Sandra Jaccoud, Virginie Philippe, Corinne Scaletta, Nathalie Hirt-Burri, Philippe Abdel-Sayed, Robin Martin, Lee Ann Applegate, Dominique P. Pioletti, and et al. 2024. "Banked Primary Progenitor Cells for Allogeneic Intervertebral Disc (IVD) Therapy: Preclinical Qualification and Functional Optimization within a Cell Spheroid Formulation Process" Pharmaceutics 16, no. 10: 1274. https://doi.org/10.3390/pharmaceutics16101274