
First-Year Real-Life Experience with Intravitreal Faricimab for Refractory Neovascular Age-Related Macular Degeneration



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Performing the Intravitreal Injections
2.3. Inclusion and Exclusion Criteria
- Eyes with refractory nAMD (as defined above).
- A minimum follow-up of 52 weeks.
- History of treatments with photodynamic therapy (PDT).
- Coexisting vitreoretinal pathology.
- Naïve patients.
2.4. Outcome Measures
- Best-corrected visual acuity (BCVA) assessed in decimals and converted to logMAR.
- Central macular thickness (CMT) as assessed with the Spectralis SD-OCT device (Heidelberg Engineering, Heidelberg, Germany) and defined as mean retinal thickness (µm) between internal limiting membrane (ILM) and Bruch’s membrane (BM) in the central 1 mm of the fovea.
- Subfoveal choroidal thickness (SFCT) measured by enhanced-depth imaging OCT (EDI-OCT) and defined as the vertical distance between the hyperreflective line of BM and the hyperreflective line of the inner surface of the sclera [23]. EDI-OCT images were taken by different technicians and analyzed in a masked manner.
- Changes in retinal fluid distribution.
- Total number of IVF injections performed at 52 W.
- Impact of various baseline SD-OCT biomarkers on total number of IVF injections.
2.5. Analysis of Baseline SD-OCT Biomarkers
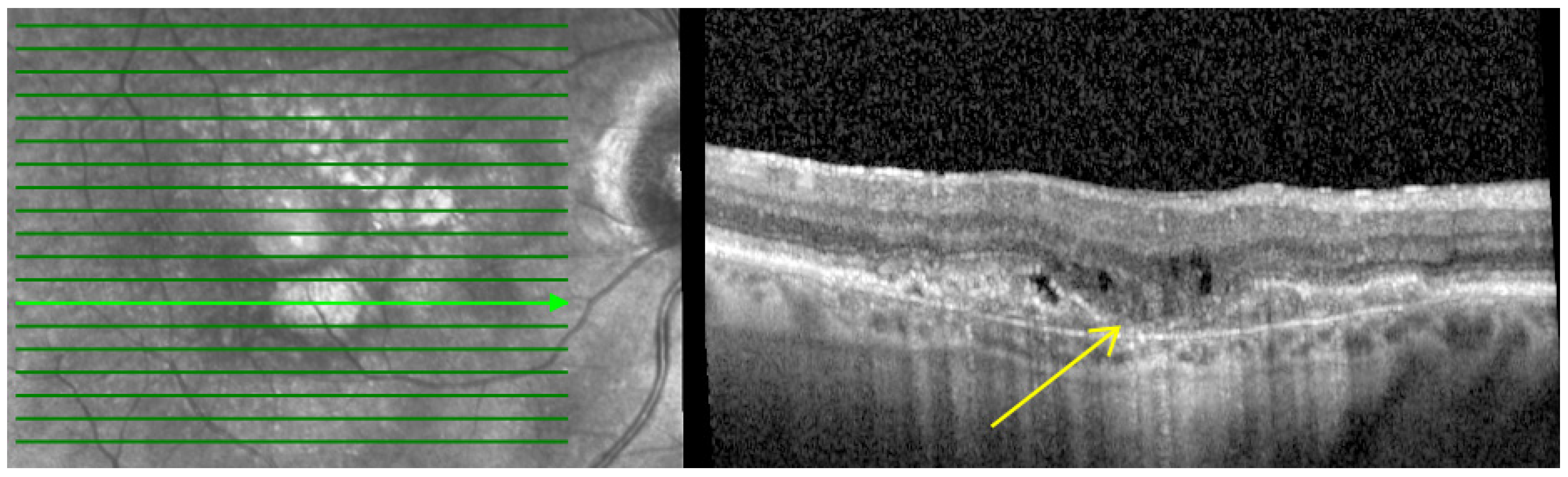
- Macular atrophy (MA): Characterized by in-lesion photoreceptor death and visual impairment and typically follows progressive atrophy and thinning of the retinal pigment epithelium (RPE) and choriocapillaris. The loss of photoreceptors can be detected by the thinning of the Henle fiber layer. This could be detected by OCT by features such as loss of the ellipsoid layer and outer limiting membrane as well as thinning of the outer nuclear layer, which together with the Henle fiber layer and photoreceptors appear as a single hyporeflective band on OCT images as shown in Figure 1 [24,25,26].
- 2.
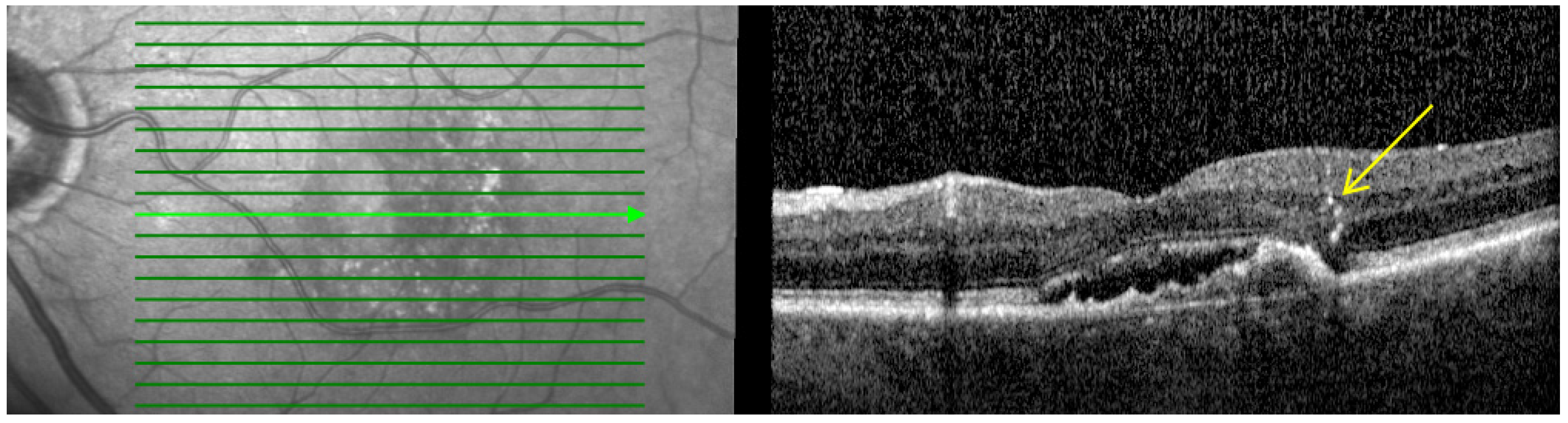
- Hyperreflective dots (HRDs): Defined as small, well-circumscribed lesions with a reflectivity equal to or greater than the RPE as shown in Figure 2. These lesions often occur over drusen and are associated with delays in visual acuity. It is hypothesized that reduced oxygen supply promotes anterior migration of RPE cells, which manifests as HRDs. On the other hand, HRDs in nAMD are also thought to be microglia, common immune cells in the inner retina that migrate from the inner retina to the outer retina when activated in an environment associated with degeneration [27,28].
- 3.
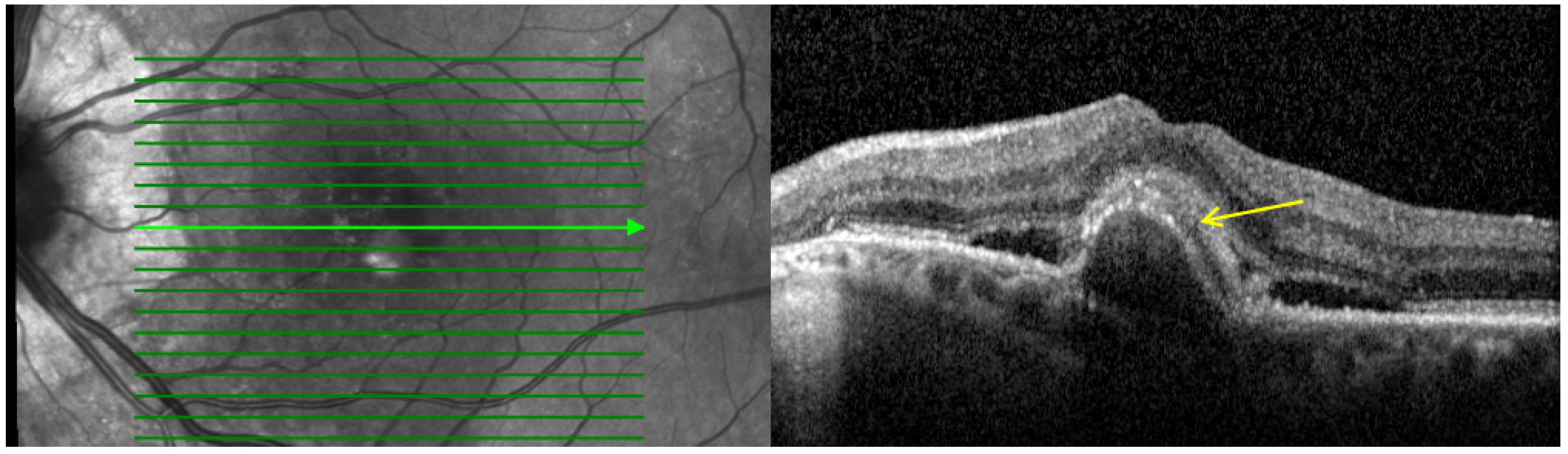
- Subretinal hyperreflective material (SHRM): Defined as a hyperreflective material located between the neurosensory retina and RPE as shown in Figure 3. In eyes with nAMD, SHRM is common and often persists after anti-VEGF treatment. SHRM is thought to have a negative impact on visual acuity and is likely to be composed of fluid, fibrin, blood, scar tissue, and MNV [29,30,31].
- 4.
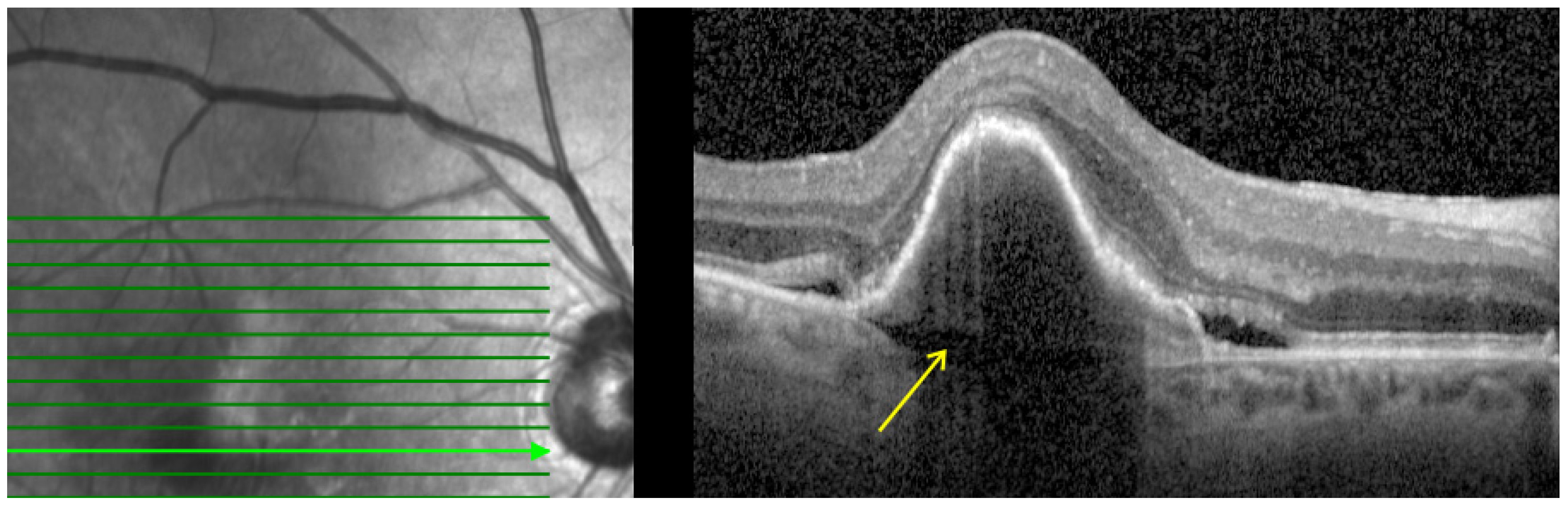
- Prechoroidal cleft (PCC): Defined as hyporeflective space between the RPE fibrovascular tissue and Bruch membrane as shown in Figure 4. PCCs are closely associated with a poor visual prognosis and increased risk of submacular hemorrhage or RPE tear [15]. The origin of the cleft has been attributed to a possible accumulation of the fluid generated by the fibrovascular tissue. However, its correlation with lesion activity and treatment remains unknown [32].
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global Prevalence of Age-Related Macular Degeneration and Disease Burden Projection for 2020 and 2040: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Abdin, A.D.; Eppinger, A.; Aljundi, W.; Abu-Dail, Y.; Munteanu, C.; Weinstein, I.; Seitz, B. Vision-Related Quality of Life among Patients with Different Types of Age-Related Macular Degeneration. Klin. Monbl. Augenheilkd. 2023, 241, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L., III; Wilkinson, C.P.; Bird, A.; Chakravarthy, U.; Chew, E.; Csaky, K.; Sadda, S.R.; Beckman Initiative for Macular Research Classification Committee. Clinical Classification of Age-Related Macular Degeneration. Ophthalmology 2013, 120, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Chappelow, A.V.; Kaiser, P.K. Neovascular Age-Related Macular Degeneration: Potential Therapies. Drugs 2008, 68, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kumar, N.; Parachuri, N.; Bandello, F.; Kuppermann, B.D.; Loewenstein, A. Faricimab: Two in the Bush Is Proving Better than One in the Hand? Ocul. Immunol. Inflamm. 2022, 30, 1961–1963. [Google Scholar] [CrossRef] [PubMed]
- Ferro Desideri, L.; Traverso, C.E.; Nicolò, M.; Munk, M.R. Faricimab for the Treatment of Diabetic Macular Edema and Neovascular Age-Related Macular Degeneration. Pharmaceutics 2023, 15, 1413. [Google Scholar] [CrossRef]
- Amoaku, W.M.; Chakravarthy, U.; Gale, R.; Gavin, M.; Ghanchi, F.; Gibson, J.; Harding, S.; Johnston, R.L.; Kelly, S.; Lotery, A. Defining Response to Anti-VEGF Therapies in Neovascular AMD. Eye 2015, 29, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Shirley, M. Faricimab: First Approval. Drugs 2022, 82, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Khanani, A.M.; Ruiz, C.Q.; Basu, K.; Ferrone, P.J.; Brittain, C.; Figueroa, M.S.; Lin, H.; Holz, F.G.; Patel, V. Efficacy, Durability, and Safety of Intravitreal Faricimab up to Every 16 Weeks for Neovascular Age-Related Macular Degeneration (TENAYA and LUCERNE): Two Randomised, Double-Masked, Phase 3, Non-Inferiority Trials. Lancet 2022, 399, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kumar, N.; Kuppermann, B.D.; Bandello, F.; Loewenstein, A. Faricimab: Expanding Horizon beyond VEGF. Eye 2020, 34, 802–804. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.A.; Finn, A.P.; Sternberg, P., Jr. Spotlight on Faricimab in the Treatment of Wet Age-Related Macular Degeneration: Design, Development and Place in Therapy. Drug Des. Devel. Ther. 2022, 16, 3395–3400. [Google Scholar] [CrossRef] [PubMed]
- Joussen, A.M.; Ricci, F.; Paris, L.P.; Korn, C.; Quezada-Ruiz, C.; Zarbin, M. Angiopoietin/Tie2 Signalling and Its Role in Retinal and Choroidal Vascular Diseases: A Review of Preclinical Data. Eye 2021, 35, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Hussain, R.M.; Neiweem, A.E.; Kansara, V.; Harris, A.; Ciulla, T.A. Tie-2/Angiopoietin Pathway Modulation as a Therapeutic Strategy for Retinal Disease. Expert Opin. Investig. Drugs 2019, 28, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Metrangolo, C.; Donati, S.; Mazzola, M.; Fontanel, L.; Messina, W.; D’alterio, G.; Rubino, M.; Radice, P.; Premi, E.; Azzolini, C. OCT Biomarkers in Neovascular Age-Related Macular Degeneration: A Narrative Review. J. Ophthalmol. 2021, 2021, 9994098. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.W.; Kim, C.G.; Lee, D.W. Long-Term Course and Visual Outcomes of Prechoroidal Cleft in Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. Retina 2021, 41, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
- Pokroy, R.; Mimouni, M.; Barayev, E.; Segev, F.; Geffen, N.; Nemet, A.Y.; Segal, O. Prognostic Value of Subretinal Hyperreflective Material in Neovascular Age-Related Macular Degeneration Treated with Bevacizumab. Retina 2018, 38, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, Z.F.; Haddad, Z.A.; Schakal, A.; Jaafar, R.F.; Saab, M.; Baha’N, N. Intravitreal Bevacizumab for Treatment of Neovascular Age-Related Macular Degeneration: A One-Year Prospective Study. Am. J. Ophthalmol. 2008, 145, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Abdin, A.D.; Suffo, S.; Bischoff-Jung, M.; Daas, L.; Pattmöller, M.; Seitz, B. Advantages of a Designated IVI Center for a German University Eye Hospital. Ophthalmologe 2020, 117, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Jaissle, G.B.; Szurman, P.; Bartz-Schmidt, K.U. Empfehlung Für Die Durchführung von Intravitrealen Injektionen. Klin. Monbl. Augenheilkd. 2005, 222, 390–395. [Google Scholar] [CrossRef]
- Mccannel, C.A. Meta-Analysis of Endophthalmitis after Intravitreal Injection of Anti–Vascular Endothelial Growth Factor Agents: Causative Organisms and Possible Prevention Strategies. Retina 2011, 31, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; Bakri, S.J.; Blumenkranz, M.S.; Brucker, A.J.; Cunningham, E.T., Jr.; D’Amico, D.J.; Dugel, P.U.; Flynn, H.W., Jr.; Freund, K.B.; Haller, J.A. Intravitreal Injection Technique and Monitoring: Updated Guidelines of an Expert Panel. Retina 2014, 34, S1–S18. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, E.B.; Meyer, C.H.; Grumann, A., Jr.; Shiroma, H.; Aguni, J.S.; Farah, M.E. Tunneled Scleral Incision to Prevent Vitreal Reflux after Intravitreal Injection. Am. J. Ophthalmol. 2007, 143, 1035–1037. [Google Scholar] [CrossRef] [PubMed]
- Aljundi, W.; Gradinger, F.; Langenbucher, A.; Sideroudi, H.; Seitz, B.; Abdin, A.D. Choroidal Thickness as a Possible Predictor of Non-Response to Intravitreal Bevacizumab for Macular Edema after Retinal Vein Occlusion. Sci. Rep. 2023, 13, 451. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Outer Retinal Atrophy after Regression of Subretinal Drusenoid Deposits as a Newly Recognized Form of Late Age-Related Macular Degeneration. Retina 2013, 33, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, M.V.; Rabiolo, A.; Sacconi, R.; Lamanna, F.; Querques, L.; Bandello, F.; Querques, G. Retinal Vascular Alterations in Reticular Pseudodrusen with and without Outer Retinal Atrophy Assessed by Optical Coherence Tomography Angiography. Br. J. Ophthalmol. 2018, 102, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Foss, A.; Rotsos, T.; Empeslidis, T.; Chong, V. Development of Macular Atrophy in Patients with Wet Age-Related Macular Degeneration Receiving Anti-VEGF Treatment. Ophthalmologica 2022, 245, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Hsia, Y.; Yang, C.-H.; Hsieh, Y.-T.; Yang, C.-M.; Ho, T.-C.; Lai, T.-T. Hyperreflective Foci in Predicting the Treatment Outcome of Antivascular Endothelial Growth Factor in Neovascular Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Duic, C.; Pfau, K.; Keenan, T.D.L.; Wiley, H.; Thavikulwat, A.; Chew, E.Y.; Cukras, C. Hyperreflective Foci in Age-Related Macular Degeneration Are Associated with Disease Severity and Functional Impairment. Ophthalmol. Retina 2023, 7, 307–317. [Google Scholar] [CrossRef]
- Willoughby, A.S.; Ying, G.; Toth, C.A.; Maguire, M.G.; Burns, R.E.; Grunwald, J.E.; Daniel, E.; Jaffe, G.J.; Williams, D.F.; Beardsley, S. Subretinal Hyperreflective Material in the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology 2015, 122, 1846–1853. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.B.; Stinnett, S.; Han, J.I.L.; Jaffe, G.J. Correlation of Subretinal Hyperreflective Material Morphology and Visual Acuity in Neovascular Age-Related Macular Degeneration. Retina 2020, 40, 845–856. [Google Scholar] [CrossRef]
- Pece, A.; Fossataro, F.; Maione, G.; Liuzzi, R. Structural and Clinical Changes in Previously Treated Type 1 Macular Neovascularization in Non-Responder AMD Eyes Switched to Brolucizumab. Eur. J. Ophthalmol. 2024, 34, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, M.; Monteduro, D.; Parrulli, S.; Ristoldo, F.; Corvi, F.; Zicarelli, F.; Staurenghi, G.; Invernizzi, A. Prechoroidal Cleft Thickness Correlates with Disease Activity in Neovascular Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, V.M.; Chan, C.C. The Role of Anti-Inflammatory Agents in Age-Related Macular Degeneration (AMD) Treatment. Eye 2011, 25, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Apte, R.S. Regulation of Angiogenesis by Macrophages. Retin. Degener. Dis. Adv. Exp. Med. Biol. 2010, 664, 15–19. [Google Scholar]
- Penfold, P.L.; Wong, J.G.; Gyory, J.; Billson, F.A. Effects of Triamcinolone Acetonide on Microglial Morphology and Quantitative Expression of MHC-II in Exudative Age-related Macular Degeneration. Clin. Exp. Ophthalmol. 2001, 29, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Brown, K.E.; Milam, A.H. Activated Microglia in Human Retinitis Pigmentosa, Late-Onset Retinal Degeneration, and Age-Related Macular Degeneration. Exp. Eye Res. 2003, 76, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Busbee, B.G.; Ho, A.C.; Brown, D.M.; Heier, J.S.; Suñer, I.J.; Li, Z.; Rubio, R.G.; Lai, P.; Group, H.S. Twelve-Month Efficacy and Safety of 0.5 Mg or 2.0 Mg Ranibizumab in Patients with Subfoveal Neovascular Age-Related Macular Degeneration. Ophthalmology 2013, 120, 1046–1056. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Zhao, J.; Sun, X. Resistance to Anti-VEGF Therapy in Neovascular Age-Related Macular Degeneration: A Comprehensive Review. Drug Des. Devel. Ther. 2016, 10, 1857–1867. [Google Scholar]
- Tenbrock, L.; Wolf, J.; Boneva, S.; Schlecht, A.; Agostini, H.; Wieghofer, P.; Schlunck, G.; Lange, C. Subretinal Fibrosis in Neovascular Age-Related Macular Degeneration: Current Concepts, Therapeutic Avenues, and Future Perspectives. Cell Tissue Res. 2022, 387, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Xu, H. Parainflammation, Chronic Inflammation, and Age-Related Macular Degeneration. J. Leukoc. Biol. 2015, 98, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Daniel, E.; Toth, C.A.; Grunwald, J.E.; Jaffe, G.J.; Martin, D.F.; Fine, S.L.; Huang, J.; Ying, G.; Hagstrom, S.A.; Winter, K. Risk of Scar in the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology 2014, 121, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Takeda, A.; Hasegawa, E.; Jo, Y.-J.; Arima, M.; Oshima, Y.; Ryoji, Y.; Nakazawa, T.; Yuzawa, M.; Nakashizuka, H. Interleukin-6 Plays a Crucial Role in the Development of Subretinal Fibrosis in a Mouse Model. Immunol. Med. 2018, 41, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Schrimpf, C.; Duffield, J.S. Mechanisms of Fibrosis: The Role of the Pericyte. Curr. Opin. Nephrol. Hypertens. 2011, 20, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Linder, M.; Foxton, R.; Uhles, S.; Revelant, F.; Lazendic, M.; Canonica, J.; Garrido, M.G.; Westenskow, P. Simultaneous Ang-2/VEGF-A Inhibition Prevents Subretinal Fibrosis Progression in Preclinical Mouse Models of Choroidal Neovascularization (CNV). Investig. Ophthalmol. Vis. Sci. 2021, 62, 349. [Google Scholar]
- Grimaldi, G.; Cancian, G.; Rizzato, A.; Casanova, A.; Perruchoud-Ader, K.; Clerici, M.; Consigli, A.; Menghini, M. Intravitreal Faricimab for Neovascular Age-Related Macular Degeneration Previously Treated with Traditional Anti-VEGF Compounds: A Real-World Prospective Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023. ahead of print. [Google Scholar] [CrossRef]
- Pandit, S.A.; Momenaei, B.; Wakabayashi, T.; Mansour, H.A.; Vemula, S.; Durrani, A.F.; Pashaee, B.; Kazan, A.S.; Ho, A.C.; Klufas, M. Clinical Outcomes of Faricimab in Patients with Previously Treated Neovascular Age-Related Macular Degeneration. Ophthalmol. Retina 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.; Kolli, H.; Ajith Kumar, N.; Azzopardi, M.; Logeswaran, A.; Buensalido, J.; Mushtaq, B.; Chavan, R.; Chong, Y.J. Real-World Data on Faricimab Switching in Treatment-Refractory Neovascular Age-Related Macular Degeneration. Life 2024, 14, 193. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Itagaki, K.; Hashiya, N.; Wakugawa, S.; Tanaka, K.; Nakayama, M.; Yamamoto, A.; Mukai, R.; Honjyo, J.; Maruko, I. Six-Month Outcomes of Switching from Aflibercept to Faricimab in Refractory Cases of Neovascular Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2024, 262, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Sadda, S.R.; Guymer, R.; Monés, J.M.; Tufail, A.; Jaffe, G.J. Anti–Vascular Endothelial Growth Factor Use and Atrophy in Neovascular Age-Related Macular Degeneration: Systematic Literature Review and Expert Opinion. Ophthalmology 2020, 127, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Eng, V.A.; Rayess, N.; Nguyen, H.V.; Leng, T. Complete RPE and Outer Retinal Atrophy in Patients Receiving Anti-VEGF Treatment for Neovascular Age-Related Macular Degeneration. PLoS ONE 2020, 15, e0232353. [Google Scholar] [CrossRef] [PubMed]
- Mitamura, Y.; Mitamura-Aizawa, S.; Katome, T.; Naito, T.; Hagiwara, A.; Kumagai, K.; Yamamoto, S. Photoreceptor Impairment and Restoration on Optical Coherence Tomographic Image. J. Ophthalmol. 2013, 2013, 518170. [Google Scholar] [CrossRef] [PubMed]
- Nawash, B.; Ong, J.; Driban, M.; Hwang, J.; Chen, J.; Selvam, A.; Mohan, S.; Chhablani, J. Prognostic Optical Coherence Tomography Biomarkers in Neovascular Age-Related Macular Degeneration. J. Clin. Med. 2023, 12, 3049. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.M.; Kwon, H.J.; Yi, J.H.; Lee, C.S.; Lee, S.C. Subfoveal Choroidal Thickness as a Potential Predictor of Visual Outcome and Treatment Response after Intravitreal Ranibizumab Injections for Typical Exudative Age-Related Macular Degeneration. Am. J. Ophthalmol. 2014, 157, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Beraldo, D.P.; Rezende, M.P.; Alexander, J.G.; Polido, J.; Belfort, R., Jr.; Cabral, T. Correlations between Subfoveal Choroidal Thickness, Macular Thickness, and Visual Outcome in Neovascular Age-Related Macular Degeneration Using Swept Source OCT: Insights from Intravitreal Aflibercept Treatment. Int. J. Retin. Vitr. 2023, 9, 70. [Google Scholar] [CrossRef] [PubMed]
- Abdin, A.D.; Hanifa, O.; Aljundi, W.; Munteanu, C.; Seitz, B.; Suffo, S. Long-Term Choroidal Thickness Changes Based on the Subtype of Macular Neovascularization in Neovascular Age-Related Macular Degeneration (5-Year Follow-Up). Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 262, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Mitchell, P.; Finger, R.P.; Eldem, B.; Talks, S.J.; Hirst, C.; Paladini, L.; Barratt, J.; Wong, T.Y.; Loewenstein, A. Nonadherence or Nonpersistence to Intravitreal Injection Therapy for Neovascular Age-Related Macular Degeneration: A Mixed-Methods Systematic Review. Ophthalmology 2021, 128, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Fragiotta, S.; Rossi, T.; Cutini, A.; Grenga, P.L.; Vingolo, E.M. Predictive Factors for Development of Neovascular Age-Related Macular Degeneration: A Spectral-Domain Optical Coherence Tomography Study. Retina 2018, 38, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Schreur, V.; Altay, L.; van Asten, F.; Groenewoud, J.M.M.; Fauser, S.; Klevering, B.J.; Hoyng, C.B.; de Jong, E.K. Hyperreflective Foci on Optical Coherence Tomography Associate with Treatment Outcome for Anti-VEGF in Patients with Diabetic Macular Edema. PLoS ONE 2018, 13, e0206482. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Zuccaro, B.; Zucchiatti, I.; Parravano, M.; Querques, L.; Costanzo, E.; Sacconi, R.; Prascina, F.; Scarinci, F.; Bandello, F. Optical Coherence Tomography Parameters as Predictors of Treatment Response to Eplerenone in Central Serous Chorioretinopathy. J. Clin. Med. 2019, 8, 1271. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Chen, N.; Zhang, S.; Fang, Y.; Zheng, Z.; Wu, S.; Ye, X.; Chen, Y.; Chen, Y.; Shen, L. Association between Inflammatory Cytokines in the Aqueous Humor and Hyperreflective Foci on Optical Coherence Tomography in Patients with Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. Front. Med. 2022, 9, 973025. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age in years | 82 ± 5 |
| Gender (Male:Female) | 55%:45% |
| Previous total intravitreal injections | 44 ± 21 |
| Previous intravitreal bevacizumab | 12 ± 10 |
| Previous intravitreal ranibizumab | 11 ± 9 |
| Previous intravitreal aflibercept | 21 ± 16 |
| Previous injections in previous year before switching to IVF | 8.6 ± 1.2 |
| BCVA (logMAR) | 0.73 ± 0.18 |
| CMT (µm) | 368 ± 34 |
| SFCT (µm) | 171 ± 64 |
| Type of MNV (1:2:3) | 72%:22%:6% |
| 0 W | 4 W | 8 W | 12 W | 16 W |
| 0.73 ± 0.18 | 0.74 ± 0.16 (p = 0.30) | 0.73 ± 0.16 (p = 0.89) | 0.74 ± 0.18 (p = 0.36) | 0.74 ± 0.21 (p = 0.57) |
| 20 W | 24 W | 28 W | 32 W | 36 W |
| 0.72 ± 0.21 (p = 0.77) | 0.69 ± 0.21 (p = 0.14) | 0.68 ± 0.20 (p = 0.14) | 0.66 ± 0.20 (p = 0.07) | 0.65 ± 0.22 (p = 0.07) |
| 40 W | 44 W | 48 W | 52 W | ∆BCVA |
| 0.67 ± 0.23 (p = 0.24) | 0.66 ± 0.24 (p = 0.11) | 0.66 ± 0.26 (p = 0.15) | 0.68 ± 0.20 (p = 0.06) | −0.04 ± 0.14 |
| 0 W | 4 W | 8 W | 12 W | 16 W |
| 368 ± 34 | 371 ± 69 (p = 0.86) | 357 ± 76 (p = 0.17) | 333 ± 61 (p = 0.03) | 327 ± 66 (p = 0.01) |
| 20 W | 24 W | 28 W | 32 W | 36 W |
| 314 ± 69 (p < 0.01) | 333 ± 76 (p = 0.01) | 318 ± 68 (p < 0.01) | 325 ± 62 (p = 0.02) | 325 ± 57 (p < 0.01) |
| 40 W | 44 W | 48 W | 52 W | ∆CMT |
| 321 ± 61 (p = 0.02) | 327 ± 59 (p < 0.01) | 305 ± 53 (p < 0.01) | 280 ± 67 (p < 0.01) | −87 ± 95 |
| 0 W | 4 W | 8 W | 12 W | 16 W |
| 171 ± 64 | 171 ± 63 (p = 0.79) | 185 ± 61 (p = 0.23) | 176 ± 62 (p = 0.78) | 170 ± 60 (p = 0.62) |
| 20 W | 24 W | 28 W | 32 W | 36 W |
| 169 ± 59 (p = 0.62) | 173 ± 62 (p = 0.57) | 167 ± 65 (p = 0.89) | 162 ± 59 (p = 0.33) | 168 ± 62 (p = 0.96) |
| 40 W | 44 W | 48 W | 52 W | ∆SFCT |
| 164 ± 62 (p = 0.79) | 171 ± 62 (p = 0.90) | 167 ± 62 (p = 0.73) | 162 ± 58 (p = 0.40) | −5 ± 37 |
| 0 W | 52 W | P1 * | P2 ** | P3 *** | P4 **** | |
|---|---|---|---|---|---|---|
| IRF | 10 (30%) | 6 (18%) | 0.25 | 0.06 (0.32) | 0.52 (−0.11) | 0.10 (0.30) |
| SRF | 22 (66%) | 8 (24%) | <0.01 | 0.07 (0.31) | 0.78 (0.04) | 0.16 (0.26) |
| PED | 30 (90%) | 24 (72%) | 0.54 | 0.24 (−0.20) | 0.84 (0.03) | 0.47 (−0.13) |
| MA | 7 (21%) | 11 (33%) | 0.29 | 0.13 (0.26) | 0.02 (−0.59) | 0.90 (0.02) |
| HRDs | 17 (51%) | 16 (48%) | 0.80 | <0.01 (−0.65) | 0.06 (−0.32) | 0.21 (−0.23) |
| PCCs | 6 (18%) | 6 (18%) | 1.00 | 0.57 (−0.10) | 0.60 (0.09) | 0.11 (0.29) |
| SHRM | 9 (27%) | 6 (18%) | 0.37 | 0.39 (0.15) | 0.14 (−0.26) | 0.45 (−0.14) |
| SFCT | 171 ± 64 | 162 ± 58 | 0.40 | <0.01 (−0.63) | 0.17 (−0.24) | 0.49 (−0.13) |
| Study | Year | n | Follow-Up Time | Main Finding |
|---|---|---|---|---|
| Grimaldi et al. [45] | 2023 | 26 | 30 weeks | IVF improves anatomical outcomes while preserving visual acuity. |
| Pandit et al. [46] | 2023 | 218 | 6 months | |
| Ng et al. [47] | 2024 | 63 | 6 months | |
| Kataoka et al. [48] | 2024 | 130 | 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljundi, W.; Daas, L.; Suffo, S.; Seitz, B.; Abdin, A.D. First-Year Real-Life Experience with Intravitreal Faricimab for Refractory Neovascular Age-Related Macular Degeneration. Pharmaceutics 2024, 16, 470. https://doi.org/10.3390/pharmaceutics16040470
Aljundi W, Daas L, Suffo S, Seitz B, Abdin AD. First-Year Real-Life Experience with Intravitreal Faricimab for Refractory Neovascular Age-Related Macular Degeneration. Pharmaceutics. 2024; 16(4):470. https://doi.org/10.3390/pharmaceutics16040470
Chicago/Turabian StyleAljundi, Wissam, Loay Daas, Shady Suffo, Berthold Seitz, and Alaa Din Abdin. 2024. "First-Year Real-Life Experience with Intravitreal Faricimab for Refractory Neovascular Age-Related Macular Degeneration" Pharmaceutics 16, no. 4: 470. https://doi.org/10.3390/pharmaceutics16040470