

Evaluation of Population Pharmacokinetic Models of Micafungin: Implications for Dosing Regimen Optimization in Critically Ill Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Assessment of Literature Quality
2.4. Comparison of Studies
2.4.1. Assessment of Visual Predictive Distributions
2.4.2. Assessment of the Covariates’ Impact
2.5. Monte Carlo Simulation for the Probability of Target Attainment
3. Results
3.1. Study Identification
3.2. Literature Quality
3.3. Study Comparison

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Study Type | Country /Race | Study Population | No. of Subjects (M/F) | No. of Samples (Per Person) | Age (Years) Mean ± SD Median [Range] | Body Weight (kg) Mean ± SD Median [Range] | Dosing Regimens | Bioanalytical Method [LLOQ, mg/L] |
|---|---|---|---|---|---|---|---|---|---|
| Kenji Tabata et al. (2006) [16] | Phase I, II, III | Japan | Healthy subjects | 82 | 1353 (16.2) | 1353 (16.2) | 62.8 [45.1–80.6] a | 2.5–150 mg 12.5–150 mg 1–6 mg/kg | HPLC-FLD [0.05] |
| Adult patients | 97 | 395 (4.1) | 395 (4.1) | 50.3 [28–76.4] a | |||||
| Pediatric patients | 19 | 77 (4) | 77 (4) | 22.0 ± 14.0 [7–48] | |||||
| Kazuro Ikawa et al. (2009) [17] | Prospective | Japan | Adult hematology patients | 10 (4/6) | 48 (4.8) | 63.5 + 16.2 [30–79] | 55.4 ± 10.3 [46.0–77.4] | 50–300 mg, single dose | HPLC-FLD [0.05] |
| P.B. Smith et al. (2009) [21] | Phase I | America | Critically ill preterm neonates > 48 h | 34 (21/13) | NA (>5) | GTA: 26.65 [23–39] c PCA: 30.45 [26–39] c PTA: 26.7 [2–82] a | 1.185 [0.54–2.2] a | 15 mg qd, 5 days 0.75 mg/kg, 1.5 mg/kg, 3.0 mg/kg, single dose | HPLC-MS/MS [0.05] |
| David Andes et al. (2011) [8] | Phase III | North America, Europe, Brazil, India, Thailand, South Africa, Australia | Invasive candidiasis or candidemia infection | 493 (290/203) | NA | 55 [13–89] b | 68 [28–155] b | 100–150 mg qd, 14–56 days | NA |
| Emilio Maseda et al. (2014) [30] | Prospective | Spain | ICU patients | 10 (8/2) | 280 (28) | 72 ± 8.2 73.5 [54–83] | 69.6 ± 6.3 70.0 [61–80] | 100 mg qd | HPLC-UV [0.2] |
| William W. Hope et al. (2015) [20] | Phase I, II | America | Treatment or prophylaxis against aspergillus spp. or candida spp. | 229 | 1919 (8.4) | 0.3 to <2 years: 1.0 ± 0.4 | 7.9 ± 1.7 | 0.5, 1, 1.5, 2, 3, 4, 4.5 mg/kg qd | HPLC-FLD [0.05] |
| 2–5 years: 3.7 ±1.2 | 15.3 ± 4.4 | ||||||||
| 6–11 years: 9.0 ± 1.5 | 28.9 ±9.0 | ||||||||
| 12–16 years: 14.5 ±1.5 | 54.4 ± 17.3 | ||||||||
| Lisa C. Martial et al. (2017) [11] | Prospective | America | ICU patients | 20 (8/12) | 356 (17.8) | 68 [20–84] | 76.5 [50–134] | 100 mg qd | HPLC-UV [0.01] |
| Vincent Jullien et al. (2017) [12] | Phase III | France | ICU patients | 99 (66/33) | 436 (4.4) | 61.4 [29.9–92.7] | 84.5 [48–141] | 100 mg qd, 14 days | HPLC-FLD [0.2] |
| E. W. Muilwijk et al. (2018) [28] | Phase II | The Netherlands | Adult hematology patients | 20 (12/8) | ~340 (17) | 59.5 [38–68] | 86.6 [53.5–110.1] | 300 mg twice a week or 100 mg qd | HPLC-FLD [0.01] |
| Sharat Chandra et al. (2018) [19] | Phase I | America | HSCT patients | 24 (6/18) | 267 (11.1) | 3.8 [0.6–10.4] | 15.4 [7.7–30.3] | 5 mg/kg, every 4 days | HPLC-UV [0.05] |
| Roeland E. Wasmann et al. (2019) [27] | Phase IV | The Netherlands | Healthy volunteers or obese adults | 24 (12/12) | ~240 (10) | 31 [22–56] d 51 [35–61] e 46 [24–54] f | 70.8 [61.5–81.5] d 156 [112–184] e 141 [126–180] f | Morbidly obese subjects: 100 mg or 200 mg Normal-weight subjects: 100 mg | UPLC-FLD [0.01] |
| Silke Gastine et al. (2019) [31] | Prospective | Germany | Critically ill patients | 36 (24/12) | NA (≥9) | 65 [22–84] | 94.5 [49.9–162] | 100 mg qd | HPLC-FLD [0.1] |
| Zhong Shubai et al. (2019) [29] | Prospective | China | Sepsis patients | 32 (21/11) | 153 (4.8) | 60.1 [23.0–89.0] a | 70.22 a [55.0–90.0] | 100, 150, 200 mg qd | HPLC-UV [0.2] |
| Iasonas Kapralos et al. (2020) [32] | Prospective | Greece | Critically ill patients | 14 (7/7) | 210 (15) | 61 ± 15 [31–83] | 85 ± 22 [55–130] | 100 mg qd | HPLC-FLD [0.059] |
| Saeed Alqahtani et al. (2021a) [33] | Prospective | Saudi Arabia | Noncancer patients | 9 (6/3) | 63 (7) | 51.1 ± 19.1 | 69.8 ± 15.7 | 100–150 mg qd, two doses | HPLC-UV [0.1] |
| Saeed Alqahtani et al. (2021b) [33] | Prospective | Saudi Arabia | Cancer patients | 10 (6/4) | 70 (7) | 47.3 ± 12.3 | 63.4 ± 18.2 | 100 mg qd, two doses | HPLC-UV [0.1] |
| Didi Bury et al. (2022) [18] | Phase IV | The Netherlands | Pediatric patients | 61 (34/27) | ~420 (>5) | 4.0 [1.0–17] | 19.5 [8.60–182] | 9 mg/kg (maximum 300 mg), twice a week | UPLC-FLD [0.01] |
| Study (Year) | Software/ Algorithm | Compartment | Fixed Effect Parameters | Between Subject Variability | Residual Unexplained Variability | Model Evaluation | Model Application | |
|---|---|---|---|---|---|---|---|---|
| Kenji Tabata et al. (2006) [16] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (mL/min) | 13.0 + 0.228 × (BW-2.3) × FIX + 0.0345 × (PLT-21.6) (IF AGE ≥ 16, FIX = 0, IF AGE < 16, FIX = 1) | 23.80% | 11.00% | GOF; VPC | NA |
| V (L) | 11.2 | 23.80% | ||||||
| Vss (L) | 20.6 | 23.80% | ||||||
| Q (mL/min) | 96.5 | 23.80% | ||||||
| Kazuro Ikawa et al. (2009) [17] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.762 | 15.40% | 0.642 mg/L | GOF, bootstrap | Assessment of micafungin regimens based on PTA of fAUC24/MIC against Aspergillus |
| Vd (L) | 9.25 | 24.60% | ||||||
| Vp (L) | 8.86 | 71.80% | ||||||
| Q (L/h) | 7.02 | 0 FIXED | ||||||
| P Brian Smith et al. (2009) [21] | NONMEM FOCE | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.0365 | 48.80% | 29.20% | NA | NA |
| V (L) | 0.507 | 48.80% | ||||||
| Vss (L) | 1.6 | 48.80% | ||||||
| Q (L/h) | 0.0316 | / | ||||||
| David Andes et al. (2011) [8] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.05 × (BW/65)0.258 | 36.00% | 19.30% | GOF | Explore the relationship between clinical outcome and microbiological response. |
| Vd (L) | 10.2 | 28.30% | ||||||
| Vp (L) | 10.3 | 50.50% | ||||||
| Q (L/h) | 6.59 | 84.50% | ||||||
| Emilio Maseda et al. (2014) [30] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.88 × (BW/70)0.75 | 20.20% | 1.30% 0.36 mg/L | GOF, bootstrap, VPC | Evaluate covariate effects; Describe PK in specific populations. |
| 22.1% (IOV) | ||||||||
| Vd (L) | 12.5 | 8.30% | ||||||
| 28.1% (IOV) | ||||||||
| Vp (L) | 10 | 7.50% | ||||||
| 27.4% (IOV) | ||||||||
| Q (L/h) | 5.03 | / | ||||||
| William W. Hope et al. (2015) [20] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.356 × (BW/21.5)0.787 × (AST/50)−0.0601 × (TBIL/12)−0.0492 | 28.90% | 17.69% 35.92%a 0.0666 mg/L | GOF, bootstrap | Evaluate covariate effects; Describe PK in specific populations; Identify therapeutic micafungin regimens. |
| Vd (L) | 1.21 | 98.30% | ||||||
| 4.62 | 16.61% | |||||||
| Q (L/h) | 5.54 | 123.20% | ||||||
| Lisa C. Martial et al. (2017) [11] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.1 | 40.10% | 17% | GOF, bootstrap, pcVPC | Evaluate covariate effects; Optimize dosing regimens. |
| Vd (L) | 17.6 | 73.20% | ||||||
| Vp (L) | 3.63 | 37.0% (IOV) | ||||||
| Q (L/h) | 0.363 | / | ||||||
| Vincent Jullien et al. (2017) [12] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.34 × (BW/84)0.59 × 1.14 (if ALB ≤ 25 g/L) × 0.75 (if SOFA ≥ 10) | 11.40% | 1.44% | GOF, bootstrap, VPC, NPDE | Evaluate covariate effects; Analyze the PK/PD in specific populations; Evaluate the PTA of dosing regimens; Optimize dosing regimens. |
| Vd (L) | 11.8 × (BW/84)0.61 × 1.14 (if ALB ≤ 25 g/L) | 37.81% | ||||||
| Vp (L) | 7.68 × (BW/84)0.67 × 1.14 (if ALB ≤ 25 g/L) | 15.00% | ||||||
| Q(L/h) | 4.67 | 13.90% | ||||||
| EW Muilwijk et al. (2018) [28] | NONMEM FOCE-I | 3 CMT zero-order input first-order elimination | CL (L/h) | 1.01 × (FFM/57.18)0.75 | 21.30% | 7.71% 0.0878 mg/L | GOF, bootstrap, VPC | Evaluate the PK rationale of extending the dosing interval in special populations. |
| 9.78% (IOV) | ||||||||
| V1 (L) | 6.26 × (FFM/57.18)1 | 48.10% | ||||||
| V2 (L) | 6.26 × (FFM/57.18)1 | 48.10% | ||||||
| V3 (L) | 6.26 × (FFM/57.18)1 | 48.10% | ||||||
| 0.809 b | ||||||||
| Q1 (L/h) | 10.3 × (FFM/57.18)0.75 | / | ||||||
| Q2 (L/h) | 2.04 × (FFM/57.18)0.75 | / | ||||||
| Sharat Chandra et al. (2018) [19] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.78 × (BW/70)0.75 | 20.50% | 18% 0.15 mg/L | GOF, pcVPC, bootstrap | Describe PK in specific populations; Evaluated the PK rationale of extending the dosing interval of micafungin. |
| Vd (L) | 13.9 × (BW/70) | 31.20% | ||||||
| Vp (L) | 5.9 × (BW/70) | 0 | ||||||
| Q (L/h) | 1.1 × (BW/70)0.75 | 78.30% | ||||||
| Roeland E. Wasmann et al. (2019) [27] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.690 × (BW/70)0.74 | 8.10% | 5% | GOF, pcVPC, bootstrap | Evaluate covariate effects; Describe PK; Optimize dosing regimens in special populations. |
| Vd (L) | 5.84 × (BW/70)1.17 | 12.80% | ||||||
| Vp (L) | 6.96 × (BW/70)0.71 | / | ||||||
| Q (L/h) | 7.15 | / | ||||||
| Silke Gastine et al. (2019) [31] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.56 × 0.789 (IF TBIL > 4 mg/dL) | 48.90% | 0.26% | GOF, VPC | Evaluate covariate effects; Describe PK in specific populations; Evaluate the efficacy of dosing regimen. |
| Vd (L) | 16.2 × 0.692 (IF SOFA > 10) | 70% | ||||||
| Vp (L) | 13.8 | / | ||||||
| Q (L/h) | 14.4 | / | ||||||
| Iasonas Kapralos et al. (2020) [32] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.31 | 19.00% | 14.90% | GOF, bootstrap, pcVPC | Analyze the PK/PD in specific populations; Optimize dosage regimens. |
| 45% (IOV) | ||||||||
| Vd (L) | 14.2 | 18.00% | ||||||
| 27% (IOV) | ||||||||
| Vp (L) | 12.6 | 51.00% | ||||||
| Q (L/h) | 2.89 | 63.00% | ||||||
| Zhong Shubai et al. (2021) [29] | NONMEM FOCE-I | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.76 × e((ALT/43) × (−0.268)) | 24.10% | 1.06 mg/L | GOF, VPC, bootstrap, NPDE | Evaluate covariate effects; Evaluate the PK rationale for extending the dosing interval. |
| Vd (L) | 6.7 | 52.80% | ||||||
| Vp (L) | 10.2 × e(θ × (−1.08)) (SOFA < 10, θ = 0; SOFA ≥ 10, θ = 1) | 78.87% | ||||||
| Q (L/h) | 4.72 | / | ||||||
| Saeed Alqahtani et al. (2021a) [33] | Monolix SAEM | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.6 | 11.80% | 38.70% 0.42 mg/L | GOF, pcVPC | Describe PK; Analyze the PK/PD in specific populations; Evaluate the PTA of different dosing regimens with or without cancer. |
| Vd (L) | 12 | 7.60% | ||||||
| Vp (L) | 2.77 | 20.40% | ||||||
| Q (L/h) | 0.188 | 32.10% | ||||||
| Saeed Alqahtani et al. (2021b) [33] | Monolix SAEM | 2 CMT zero-order input first-order elimination | CL (L/h) | 1.2 | 34.10% | 45.82% 0.47 mg/L | GOF, pcVPC | Describe PK; Analyze the PK/PD in specific populations; Evaluate the PTA of different dosing regimens with or without cancer. |
| Vd (L) | 10.7 | 7.60% | ||||||
| Vp (L) | 3.5 | 36.80% | ||||||
| Q (L/h) | 0.144 | 32.20% | ||||||
| Didi Bury et al. (2022) [18] | NONMEM FOCE | 2 CMT zero-order input first-order elimination | CL (L/h) | 0.678×(FFM/57.19)0.75 | 24.90% | 9% | GOF, pcVPC | Evaluate the PK rationale for extending the dosing interval in special populations. |
3.4. Visual Predictive Distributions
3.5. Pharmacokinetic Parameters
3.6. Covariate Effect on Pharmacokinetic Parameters
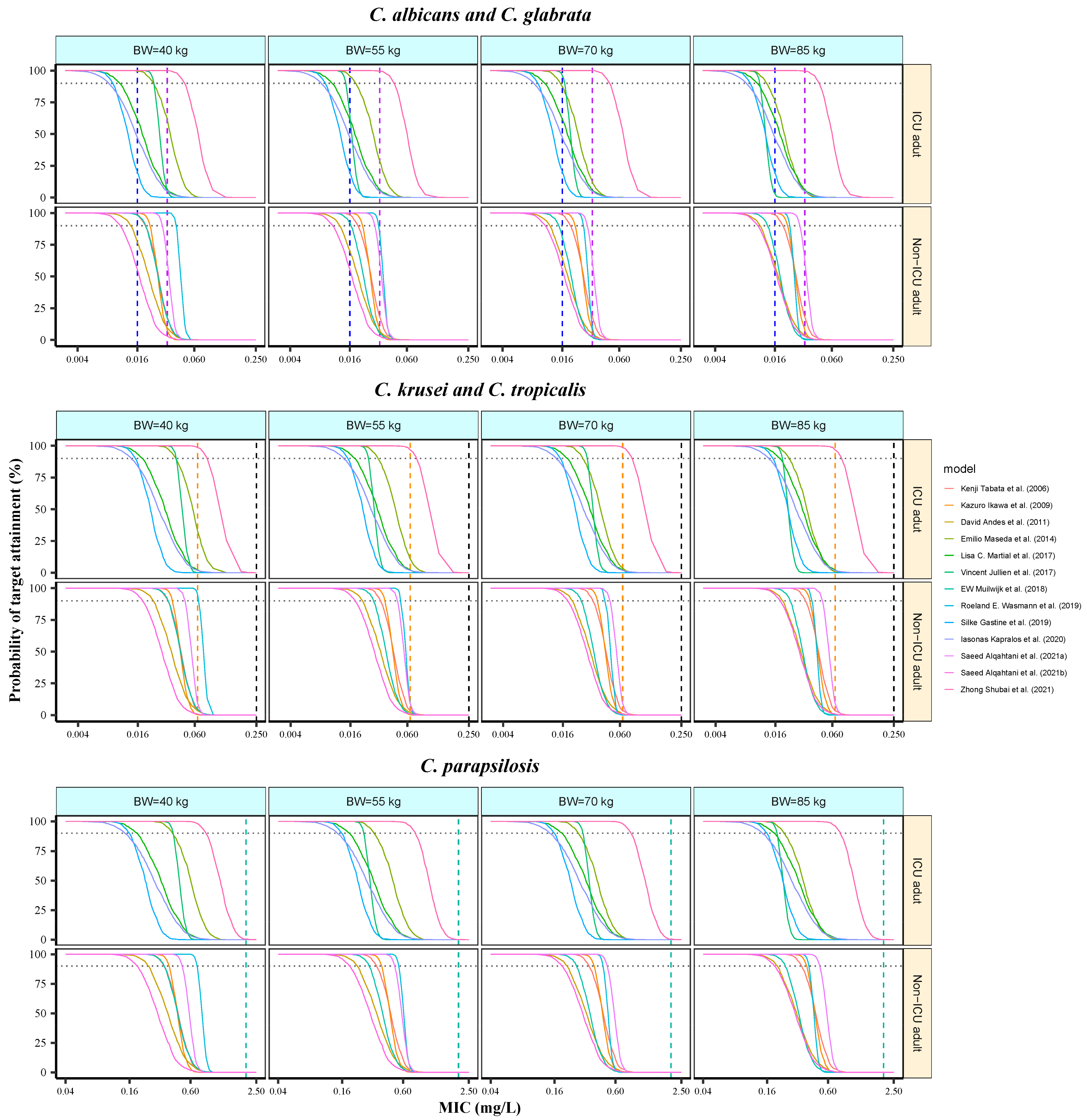
3.7. Analysis of Probability of Target Attainment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hashimoto, S. Micafungin: A sulfated echinocandin. J. Antibiot. 2009, 62, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. Echinocandin antifungal drugs. Lancet 2003, 362, 1142–1151. [Google Scholar] [CrossRef]
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. S7), 19–37. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Leroux, S.; Jacqz-Aigrain, E.; Elie, V.; Legrand, F.; Barin-Le Guellec, C.; Aurich, B.; Biran, V.; Dusang, B.; Goudjil, S.; Coopman, S.; et al. Pharmacokinetics and safety of fluconazole and micafungin in neonates with systemic candidiasis: A randomized, open-label clinical trial. Br. J. Clin. Pharmacol. 2018, 84, 1989–1999. [Google Scholar] [CrossRef] [PubMed]
- Auriti, C.; Falcone, M.; Ronchetti, M.P.; Goffredo, B.M.; Cairoli, S.; Crisafulli, R.; Piersigilli, F.; Corsetti, T.; Dotta, A.; Pai, M.P. High-Dose Micafungin for Preterm Neonates and Infants with Invasive and Central Nervous System Candidiasis. Antimicrob. Agents Chemother. 2016, 60, 7333–7339. [Google Scholar] [CrossRef]
- FDA. Mycamine. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/21506,21754lbl.pdf (accessed on 29 September 2015).
- Andes, D.; Ambrose, P.G.; Hammel, J.P.; Van Wart, S.A.; Iyer, V.; Reynolds, D.K.; Buell, D.N.; Kovanda, L.L.; Bhavnani, S.M. Use of Pharmacokinetic-Pharmacodynamic Analyses to Optimize Therapy with the Systemic Antifungal Micafungin for Invasive Candidiasis or Candidemia. Antimicrob. Agents Chemother. 2011, 55, 2113–2121. [Google Scholar] [CrossRef]
- Andes, D. In vivo pharmacodynamics of antifungal drugs in treatment of candidiasis. Antimicrob. Agents Chemother. 2003, 47, 1179–1186. [Google Scholar] [CrossRef]
- Andes, D.R.; Diekema, D.J.; Pfaller, M.A.; Marchillo, K.; Bohrmueller, J. In vivo pharmacodynamic target investigation for micafungin against Candida albicans and C. glabrata in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 3497–3503. [Google Scholar] [CrossRef]
- Martial, L.C.; Ter Heine, R.; Schouten, J.A.; Hunfeld, N.G.; van Leeuwen, H.J.; Verweij, P.E.; de Lange, D.W.; Pickkers, P.; Brüggemann, R.J. Population Pharmacokinetic Model and Pharmacokinetic Target Attainment of Micafungin in Intensive Care Unit Patients. Clin. Pharmacokinet. 2017, 56, 1197–1206. [Google Scholar] [CrossRef]
- Jullien, V.; Azoulay, E.; Schwebel, C.; Le Saux, T.; Charles, P.E.; Cornet, M.; Souweine, B.; Klouche, K.; Jaber, S.; Trouillet, J.-L.; et al. Population pharmacokinetics of micafungin in ICU patients with sepsis and mechanical ventilation. J. Antimicrob. Chemother. 2017, 72, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Kanji, S.; Hayes, M.; Ling, A.; Shamseer, L.; Chant, C.; Edwards, D.J.; Edwards, S.; Ensom, M.H.; Foster, D.R.; Hardy, B.; et al. Reporting Guidelines for Clinical Pharmacokinetic Studies: The ClinPK Statement. Clin. Pharmacokinet. 2015, 54, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Jamsen, K.M.; McLeay, S.C.; Barras, M.A.; Green, B. Reporting a population pharmacokinetic-pharmacodynamic study: A journal’s perspective. Clin. Pharmacokinet. 2014, 53, 111–122. [Google Scholar] [CrossRef]
- Duffull, S.B.; Wright, D.F. What do we learn from repeated population analyses? Br. J. Clin. Pharmacol. 2015, 79, 40–47. [Google Scholar] [CrossRef]
- Tabata, K.; Katashima, M.; Kawamura, A.; Kaibara, A.; Tanigawara, Y. Population pharmacokinetic analysis of micafungin in Japanese patients with fungal infections. Drug Metab. Pharmacokinet. 2006, 21, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Ikawa, K.; Nomura, K.; Morikawa, N.; Ikeda, K.; Taniwaki, M. Assessment of micafungin regimens by pharmacokinetic-pharmacodynamic analysis: A dosing strategy for Aspergillus infections. J. Antimicrob. Chemother. 2009, 64, 840–844. [Google Scholar] [CrossRef]
- Bury, D.; Wolfs, T.F.W.; Ter Heine, R.; Muilwijk, E.W.; Tissing, W.J.E.; Brüggemann, R.J. Pharmacokinetic evaluation of twice-a-week micafungin for prophylaxis of invasive fungal disease in children with acute lymphoblastic leukaemia: A prospective observational cohort study. J. Antimicrob. Chemother. 2022, 77, 699–703. [Google Scholar] [CrossRef]
- Chandra, S.; Fukuda, T.; Mizuno, K.; Davies, S.M.; Teusink-Cross, A.; Tarin, R.; Marsh, R.A.; Vinks, A.A.; Mehta, P.A. Micafungin antifungal prophylaxis in children undergoing HSCT: Can we give higher doses, less frequently? A pharmacokinetic study. J. Antimicrob. Chemother. 2018, 73, 1651–1658. [Google Scholar] [CrossRef]
- Hope, W.W.; Kaibara, A.; Roy, M.; Arrieta, A.; Azie, N.; Kovanda, L.L.; Benjamin, D.K., Jr. Population Pharmacokinetics of Micafungin and Its Metabolites M1 and M5 in Children and Adolescents. Antimicrob. Agents Chemother. 2015, 59, 905–913. [Google Scholar] [CrossRef]
- Smith, P.B.; Walsh, T.J.; Hope, W.; Arrieta, A.; Takada, A.; Kovanda, L.L.; Kearns, G.L.; Kaufman, D.; Sawamoto, T.; Buell, D.N.; et al. Pharmacokinetics of an elevated dosage of micafungin in premature neonates. Pediatr. Infect. Dis. J. 2009, 28, 412–415. [Google Scholar] [CrossRef]
- Li, Z.R.; Wang, C.Y.; Zhu, X.; Jiao, Z. Population Pharmacokinetics of Levetiracetam: A Systematic Review. Clin. Pharmacokinet. 2021, 60, 305–318. [Google Scholar] [CrossRef]
- Han, N.; Yun, H.Y.; Kim, I.W.; Oh, Y.J.; Kim, Y.S.; Oh, J.M. Population pharmacogenetic pharmacokinetic modeling for flip-flop phenomenon of enteric-coated mycophenolate sodium in kidney transplant recipients. Eur. J. Clin. Pharmacol. 2014, 70, 1211–1219. [Google Scholar] [CrossRef]
- Kesselheim, A.S. The backlash against bioequivalence and the interchangeability of brand-name and generic drugs. CMAJ 2011, 183, 1350–1351. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Castanheira, M.; Messer, S.A.; Rhomberg, P.R.; Jones, R.N. Comparison of EUCAST and CLSI broth microdilution methods for the susceptibility testing of 10 systemically active antifungal agents when tested against Candida spp. Diagn. Microbiol. Infect. Dis. 2014, 79, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Prakash, A.; Meletiadis, J.; Sharma, C.; Chowdhary, A. Comparison of EUCAST and CLSI Reference Microdilution MICs of Eight Antifungal Compounds for Candida auris and Associated Tentative Epidemiological Cutoff Values. Antimicrob. Agents Chemother. 2017, 61, e00485-17. [Google Scholar] [CrossRef] [PubMed]
- Wasmann, R.E.; Smit, C.; ter Heine, R.; Koele, S.E.; van Dongen, E.P.H.; Wiezer, R.M.J.; Burger, D.M.; Knibbe, C.A.J.; Bruggemann, R.J.M. Pharmacokinetics and probability of target attainment for micafungin in normal-weight and morbidly obese adults. J. Antimicrob. Chemother. 2019, 74, 978–985. [Google Scholar] [CrossRef]
- Muilwijk, E.W.; Maertens, J.A.; van der Velden, W.J.F.M.; ter Heine, R.; Colbers, A.; Burger, D.M.; Andes, D.; Theunissen, K.; Blijlevens, N.M.A.; Bruggemann, R.J.M. Pharmacokinetics of extended dose intervals of micafungin in haematology patients: Optimizing antifungal prophylaxis. J. Antimicrob. Chemother. 2018, 73, 3095–3101. [Google Scholar] [CrossRef]
- Zhong, S.; Zhu, X.; Zhao, L.; Song, Y.; Yu, J.; Zheng, Z.; Zang, B. Optimization of Micafungin Dosage for Chinese Patients with Sepsis in the Intensive Care Unit Based on a Population Pharmacokinetic-Pharmacodynamic Analysis. Pharm. Res. 2021, 38, 67–77. [Google Scholar] [CrossRef]
- Maseda, E.; Grau, S.; Villagran, M.J.; Hernandez-Gancedo, C.; Lopez-Tofino, A.; Roberts, J.A.; Aguilar, L.; Luque, S.; Sevillano, D.; Gimenez, M.J.; et al. Micafungin pharmacokinetic/pharmacodynamic adequacy for the treatment of invasive candidiasis in critically ill patients on continuous venovenous haemofiltration. J. Antimicrob. Chemother. 2014, 69, 1624–1632. [Google Scholar] [CrossRef]
- Gastine, S.; Lanckohr, C.; Blessou, M.; Horn, D.; Fobker, M.; Bause, D.; Hempel, G.; Ellger, B. Pharmacokinetics of Micafungin in Critically Ill Patients. Sci. Rep. 2019, 9, 17741. [Google Scholar] [CrossRef]
- Kapralos, I.; Mainas, E.; Neroutsos, E.; Apostolidi, S.; Siopi, M.; Apostolopoulou, O.; Dimopoulos, G.; Sambatakou, H.; Valsami, G.; Meletiadis, J.; et al. Population pharmacokinetics of micafungin over repeated doses in critically ill patients: A need for a loading dose? J. Pharm. Pharmacol. 2020, 72, 1750–1760. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.; Alfarhan, A.; Alsultan, A.; Alsarhani, E.; Alsubaie, A.; Asiri, Y. Assessment of Micafungin Dosage Regimens in Patients with Cancer Using Pharmacokinetic/Pharmacodynamic Modeling and Monte Carlo Simulation. Antibiotics 2021, 10, 1363. [Google Scholar] [CrossRef] [PubMed]
- Seibel, N.L.; Schwartz, C.; Arrieta, A.; Flynn, P.; Shad, A.; Albano, E.; Keirns, J.; Lau, W.M.; Facklam, D.P.; Buell, D.N.; et al. Safety, tolerability, and pharmacokinetics of Micafungin (FK463) in febrile neutropenic pediatric patients. Antimicrob. Agents Chemother. 2005, 49, 3317–3324. [Google Scholar] [CrossRef]
- Maseda, E.; Grau, S.; Luque, S.; Castillo-Mafla, M.P.; Suarez-de-la-Rica, A.; Montero-Feijoo, A.; Salgado, P.; Gimenez, M.J.; Garcia-Bernedo, C.A.; Gilsanz, F.; et al. Population pharmacokinetics/pharmacodynamics of micafungin against Candida species in obese, critically ill, and morbidly obese critically ill patients. Crit. Care 2018, 22, 94. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.G.; Swancutt, M.A.; Gumbo, T. Fractal geometry and the pharmacometrics of micafungin in overweight, obese, and extremely obese people. Antimicrob. Agents Chemother. 2011, 55, 5107–5112. [Google Scholar] [CrossRef]
- Wasmann, R.E.; Muilwijk, E.W.; Burger, D.M.; Verweij, P.E.; Knibbe, C.A.; Bruggemann, R.J. Clinical Pharmacokinetics and Pharmacodynamics of Micafungin. Clin. Pharmacokinet. 2018, 57, 267–286. [Google Scholar] [CrossRef]
- Kishino, S.; Ohno, K.; Shimamura, T.; Furukawatodo, H. Optimal prophylactic dosage and disposition of micafungin in living donor liver recipients. Clin. Transplant. 2004, 18, 676–680. [Google Scholar] [CrossRef]
- Hirata, K.; Aoyama, T.; Matsumoto, Y.; Ogawa, F.; Yamazaki, H.; Kikuti, A.; Yamamoto, Y. Pharmacokinetics of antifungal agent micafungin in critically ill patients receiving continuous hemodialysis filtration. Yakugaku Zasshi J. Pharm. Soc. Jpn. 2007, 127, 897–901. [Google Scholar] [CrossRef]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human serum albumin: From bench to bedside. Mol. Asp. Med. 2012, 33, 209–290. [Google Scholar] [CrossRef]
- Trainor, G.L. The importance of plasma protein binding in drug discovery. Expert Opin. Drug Discov. 2007, 2, 51–64. [Google Scholar] [CrossRef]
- Hebert, M.F.; Smith, H.E.; Marbury, T.C.; Swan, S.K.; Smith, W.B.; Townsend, R.W.; Buell, D.; Keirns, J.; Bekersky, I. Pharmacokinetics of micafungin in healthy volunteers, volunteers with moderate liver disease, and volunteers with renal dysfunction. J. Clin. Pharmacol. 2005, 45, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Benet, L.Z.; Hoener, B.A. Changes in plasma protein binding have little clinical relevance. Clin. Pharmacol. Ther. 2002, 71, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Yang, Y.; Kang, Y.; Zang, B.; Cui, W.; Qin, B.; Qin, Y.; Fang, Q.; Qin, T.; Jiang, D.; et al. Invasive candidiasis in intensive care units in China: A multicentre prospective observational study. J. Antimicrob. Chemother. 2013, 68, 1660–1668. [Google Scholar] [CrossRef] [PubMed]





| Neonates | Infants | Preschool Children | School Children | Adolescents | ICU Adults (SOFA ≥ 10) | ICU Adults (SOFA < 10) | Non-ICU Adults | |
|---|---|---|---|---|---|---|---|---|
| BW-adjusted CL (mL/h/kg) | 23.3 (17.2–32) | 19.3 (16.2–22.9) | 16.3 (13.7–19.4) | 13.9 (11.6–16.7) | 12.8 (10.3–15.6) | 14.7 (10.7–19.7) a | 15.9 (10.7–20.1) a | 11.3 (9.5–15) |
| 15.9 (13–21.1) b | 17.1 (13.4–21.3) b | |||||||
| BW-adjusted Vd (mL/kg) | 323.3 (238.4–445.3) | 185.3 (115.4–258.7) | 160.4 (98.5–219.1) | 142.2 (81.7–196.1) | 105.2 (48–158.6) | 174.2 (133–226.5) a | 174.2 (134.9–243.5) a | 136.1 (96.2–162.3) |
| 183.9 (150.7–239.7) b | 187.4 (149.4–262.9) b | |||||||
| AUC24 (mg·h/L) | 162.5 (116.9–222.2) | 103 (86.9–122.6) | 122.2 (102.6–145.4) | 143.4 (119.7–171.5) | 155.7 (127.8–194.1) | 96.8 (72–132.3) a | 89.7 (70.7–131.7) a | 125.6 (95.3–149.4) |
| 89.8 (67.4–109.5) b | 83.2 (67–106) b |
| 50% | 60% | 70% | 80% | |||||
|---|---|---|---|---|---|---|---|---|
| ICU (mg/d) | Non-ICU (mg/d) | ICU (mg/d) | Non-ICU (mg/d) | ICU (mg/d) | Non-ICU (mg/d) | ICU (mg/d) | Non-ICU (mg/d) | |
| C. albican | 150 | 100 | 150 | 100 | 150 | 150 | 200 | 150 |
| C. glabrata | 250 | 200 | 300 | 250 | 300 | 250 | >300 | 300 |
| C. krusei | >300 | >300 | >300 | >300 | >300 | >300 | >300 | >300 |
| C. tropicalis | 250 | 200 | >300 | 200 | >300 | 300 | >300 | >300 |
| C. parapsilosis | >300 | >300 | >300 | >300 | >300 | >300 | >300 | >300 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Liu, X.; Mao, J.; Liu, D.; Jiao, Z. Evaluation of Population Pharmacokinetic Models of Micafungin: Implications for Dosing Regimen Optimization in Critically Ill Patients. Pharmaceutics 2024, 16, 1145. https://doi.org/10.3390/pharmaceutics16091145
Li X, Liu X, Mao J, Liu D, Jiao Z. Evaluation of Population Pharmacokinetic Models of Micafungin: Implications for Dosing Regimen Optimization in Critically Ill Patients. Pharmaceutics. 2024; 16(9):1145. https://doi.org/10.3390/pharmaceutics16091145
Chicago/Turabian StyleLi, Xiping, Xiaoqin Liu, Juehui Mao, Dong Liu, and Zheng Jiao. 2024. "Evaluation of Population Pharmacokinetic Models of Micafungin: Implications for Dosing Regimen Optimization in Critically Ill Patients" Pharmaceutics 16, no. 9: 1145. https://doi.org/10.3390/pharmaceutics16091145