

Molded Round Window Niche Implant as a Dexamethasone Delivery System in a Cochlear Implant-Trauma Animal Model


 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
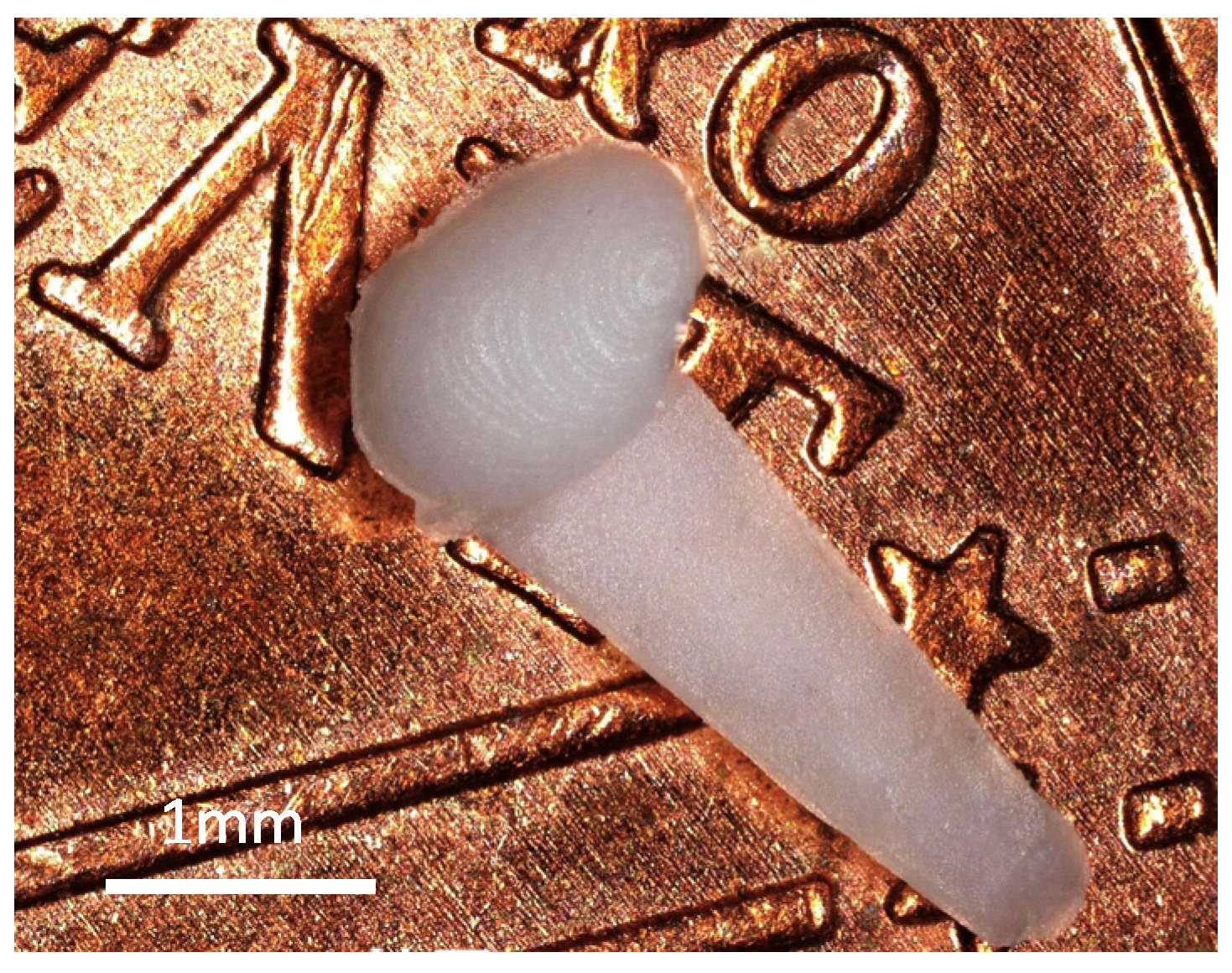
2.1. RNI Preparation
2.2. In Vitro Drug Release Test
2.3. Animals
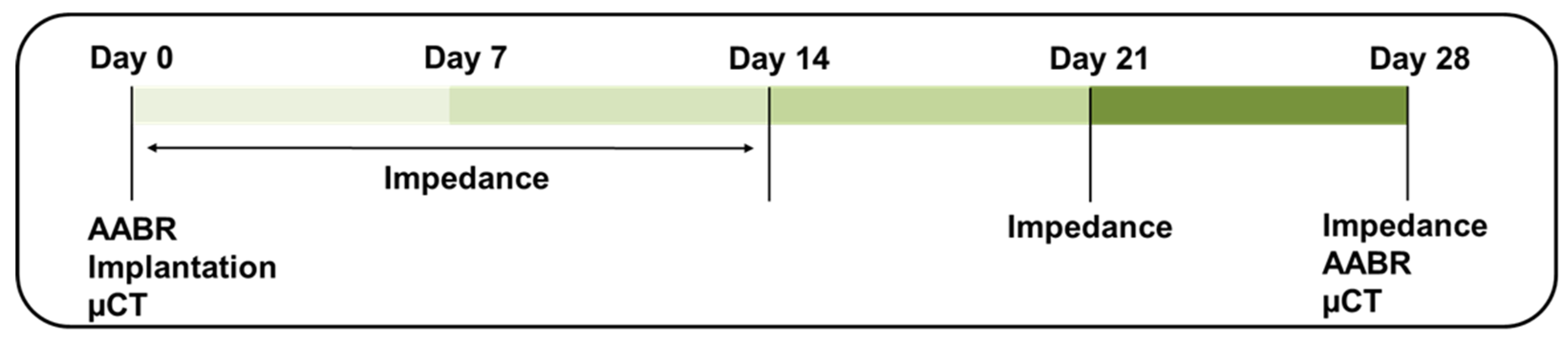
2.4. Experimental Timeline
2.5. Surgery
2.6. Acoustically Evoked Auditory Brainstem Response (AABR) Measurement
2.7. Impedance Measurement
2.8. µCT Scan
2.9. Histology
2.10. Statistical Analysis
3. Results
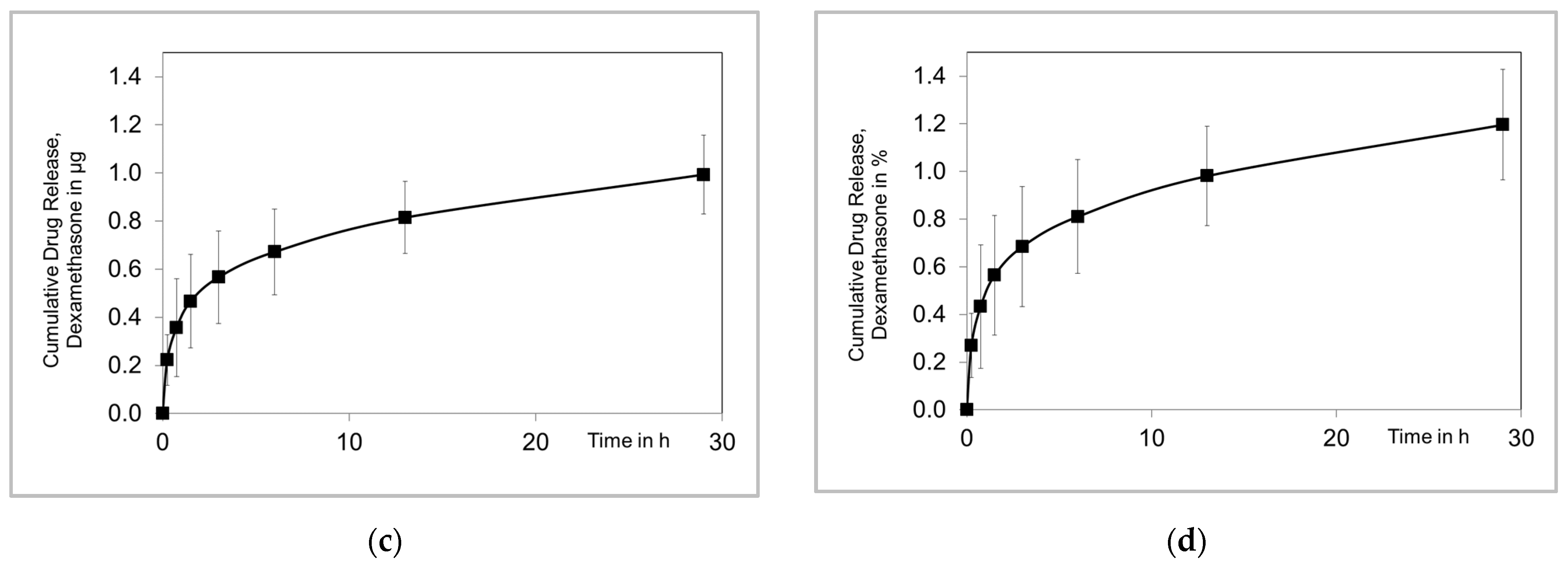
3.1. Drug Release
3.2. Hearing Threshold
3.3. Impedances
3.4. Histology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bas, E.; Dinh, C.T.; Ojo, R.; Eshraghi, A.A.; Van De Water, T.R. Loss of Residual Hearing Initiated by Cochlear Implantation: Role of Inflammation-Initiated Cell Death Pathways, Wound Healing and Fibrosis Pathways, and Potential Otoprotective Therapies. In Free Radicals in ENT Pathology; Miller, J., Le Prell, C.G., Rybak, L., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 395–421. [Google Scholar]
- Anagiotos, A.; Hamdan, N.; Lang-Roth, R.; Gostian, A.O.; Lüers, J.C.; Hüttenbrink, K.B.; Beutner, D. Young age is a positive prognostic factor for residual hearing preservation in conventional cochlear implantation. Otol. Neurotol. 2015, 36, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Gotamco, G.L.; Sun, C.H.; Chou, Y.F.; Hsu, C.J.; Wu, H.P. Effect of Round Window Opening Size on Residual Hearing Preservation in Cochlear Implantation. Otolaryngol. Head Neck Surg. 2020, 163, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Kontorinis, G.; Lenarz, T.; Stöver, T.; Paasche, G. Impact of the insertion speed of cochlear implant electrodes on the insertion forces. Otol. Neurotol. 2011, 32, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Snels, C.; IntHout, J.; Mylanus, E.; Huinck, W.; Dhooge, I. Hearing Preservation in Cochlear Implant Surgery: A Meta-Analysis. Otol. Neurotol. 2019, 40, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Khater, A.; El-Anwar, M.W. Methods of Hearing Preservation during Cochlear Implantation. Int. Arch. Otorhinolaryngol. 2017, 21, 297–301. [Google Scholar] [CrossRef]
- Choi, C.H.; Oghalai, J.S. Predicting the effect of post-implant cochlear fibrosis on residual hearing. Hear. Res. 2005, 205, 193–200. [Google Scholar] [CrossRef]
- Seyyedi, M.; Nadol, J.B., Jr. Intracochlear inflammatory response to cochlear implant electrodes in humans. Otol. Neurotol. 2014, 35, 1545–1551. [Google Scholar] [CrossRef]
- Simoni, E.; Borile, G.; Martini, A.; Cazzador, D.; Astolfi, L. Immune response after cochlear implantation. Front. Neurol. 2020, 11, 505916. [Google Scholar] [CrossRef]
- Xin, Y.; Yuan, Y.-S.; Chi, F.-L.; Wang, J.; Yang, J.-M. Foreign body reaction after Cochlear implantation: A case report. Chin. Med. J. 2015, 128, 2124–2125. [Google Scholar] [CrossRef]
- Foggia, M.J.; Quevedo, R.V.; Hansen, M.R. Intracochlear fibrosis and the foreign body response to cochlear implant biomaterials. Laryngoscope Investig. Otolaryngol. 2019, 4, 678–683. [Google Scholar] [CrossRef]
- Shaul, C.; Bester, C.W.; Weder, S.; Choi, J.; Eastwood, H.; Padmavathi, K.V.; Collins, A.; O’Leary, S.J. Electrical Impedance as a Biomarker for Inner Ear Pathology Following Lateral Wall and Peri-modiolar Cochlear Implantation. Otol. Neurotol. 2019, 40, e518–e526. [Google Scholar] [CrossRef] [PubMed]
- Tykocinski, M.; Cohen, L.T.; Cowan, R.S. Measurement and Analysis of Access Resistance and Polarization Impedance in Cochlear Implant Recipients. Otol. Neurotol. 2005, 26, 948–956. [Google Scholar] [CrossRef] [PubMed]
- Gotamco, G.L.; Chou, Y.F.; Sun, C.H.; Hsu, C.J.; Chen, P.R.; Wu, H.P. Comparison of Hearing Preservation Outcomes Using Extended Versus Single-Dose Steroid Therapy in Cochlear Implantation. Otol. Neurotol. 2020, 41, e449–e457. [Google Scholar] [CrossRef] [PubMed]
- James, D.P.; Eastwood, H.; Richardson, R.T.; O’Leary, S.J. Effects of Round Window Dexamethasone on Residual Hearing in a Guinea Pig Model of Cochlear Implantation. Audiol. Neurotol. 2007, 13, 86–96. [Google Scholar] [CrossRef]
- Parys, Q.-A.; Van Bulck, P.; Loos, E.; Verhaert, N. Inner Ear Pharmacotherapy for Residual Hearing Preservation in Cochlear Implant Surgery: A Systematic Review. Biomolecules 2022, 12, 529. [Google Scholar] [CrossRef]
- Barnes, P.J. How corticosteroids control inflammation: Quintiles prize lecture 2005. Br. J. Pharmacol. 2006, 148, 245–254. [Google Scholar] [CrossRef]
- Fuentes, I.A.C.; Pierre, P.V.; Berglin, C.E. Improving clinical outcomes in cochlear implantation using glucocorticoid therapy: A review. Ear Hear. 2020, 41, 17–24. [Google Scholar] [CrossRef]
- Dinh, C.; Haake, S.; Chen, S.; Hoang, K.; Nong, E.; Eshraghi, A.; Balkany, T.; Van De Water, T. Dexamethasone protects organ of corti explants against tumor necrosis factor-alpha–induced loss of auditory hair cells and alters the expression levels of apoptosis-related genes. Neuroscience 2008, 157, 405–413. [Google Scholar] [CrossRef]
- Dinh, C.; Hoang, K.; Haake, S.; Chen, S.; Angeli, S.; Nong, E.; Eshraghi, A.A.; Balkany, T.J.; Van De Water, T.R. Biopolymer-released dexamethasone prevents tumor necrosis factor α-induced loss of auditory hair cells in vitro: Implications toward the development of a drug-eluting cochlear implant electrode array. Otol. Neurotol. 2008, 29, 1012–1019. [Google Scholar] [CrossRef]
- Derdzakyan, N.A.; Lava, C.X.; Hakimi, A.A.; Johns, J.D.; Kim, H.J.; Hoa, M. Variability in Perioperative Steroid Therapy Regimen for Cochlear Implantation as It Relates to Hearing Preservation. Otol. Neurotol. 2024, 45, e28–e35. [Google Scholar] [CrossRef]
- Czock, D.; Keller, F.; Rasche, F.M.; Häussler, U. Pharmacokinetics and pharmacodynamics of systemically administered glucocorticoids. Clin. Pharmacokinet. 2005, 44, 61–98. [Google Scholar] [CrossRef] [PubMed]
- Oray, M.; Abu Samra, K.; Ebrahimiadib, N.; Meese, H.; Foster, C.S. Long-term side effects of glucocorticoids. Expert Opin. Drug Saf. 2016, 15, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Lyu, A.-R.; Kim, D.H.; Lee, S.H.; Shin, D.-S.; Shin, S.-A.; Park, Y.-H. Effects of dexamethasone on intracochlear inflammation and residual hearing after cochleostomy: A comparison of administration routes. PLoS ONE 2018, 13, e0195230. [Google Scholar] [CrossRef] [PubMed]
- Moatti, A.; Silkstone, D.; Martin, T.; Abbey, K.; Hutson, K.A.; Fitzpatrick, D.C.; Zdanski, C.J.; Cheng, A.G.; Ligler, F.S.; Greenbaum, A. Assessment of drug permeability through an ex vivo porcine round window membrane model. Iscience 2023, 26, 106789. [Google Scholar] [CrossRef] [PubMed]
- Makimoto, K.; Takeda, T.; Silverstein, H. Chemical composition in various compartments of inner ear fluid. Arch. Otorhinolaryngol. 1978, 220, 259–264. [Google Scholar] [CrossRef]
- Liao, A.-H.; Shih, C.-P.; Li, M.-W.; Lin, Y.-C.; Chuang, H.-C.; Wang, C.-H. Development of thermosensitive poloxamer 407-based microbubble gel with ultrasound mediation for inner ear drug delivery. Drug Deliv. 2021, 28, 1256–1271. [Google Scholar] [CrossRef]
- Borden, R.C.; Saunders, J.E.; Berryhill, W.E.; Krempl, G.A.; Thompson, D.M.; Queimado, L. Hyaluronic acid hydrogel sustains the delivery of dexamethasone across the round window membrane. Audiol. Neurotol. 2010, 16, 1–11. [Google Scholar] [CrossRef]
- Sun, C.; Wang, X.; Zheng, Z.; Chen, D.; Wang, X.; Shi, F.; Yu, D.; Wu, H. A single dose of dexamethasone encapsulated in polyethylene glycol-coated polylactic acid nanoparticles attenuates cisplatin-induced hearing loss following round window membrane administration. Int. J. Nanomed. 2015, 10, 3567–3579. [Google Scholar]
- Cai, H.; Wen, X.; Wen, L.; Tirelli, N.; Zhang, X.; Zhang, Y.; Su, H.; Yang, F.; Chen, G. Enhanced local bioavailability of single or compound drugs delivery to the inner ear through application of PLGA nanoparticles via round window administration. Int. J. Nanomed. 2014, 9, 5591–5601. [Google Scholar] [CrossRef]
- Zou, J. Controlled release of dexamethasone from fibrin sealant for intratympanic administration in inner ear therapy. J. Otol. 2024, 19, 55–58. [Google Scholar] [CrossRef]
- Dhanasingh, A.; Hochmair, I. Drug delivery in cochlear implantation. Acta Oto-Laryngol. 2021, 141 (Suppl. 1), 135–156. [Google Scholar] [CrossRef] [PubMed]
- Fleet, A.; Nikookam, Y.; Radotra, A.; Gowrishankar, S.; Metcalfe, C.; Muzaffar, J.; Smith, M.E.; Monksfield, P.; Bance, M. Outcomes following cochlear implantation with eluting electrodes: A systematic review. Laryngoscope Investig. Otolaryngol. 2024, 9, e1263. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, S.; Li, Y.; Cui, B.; Liu, Y.; Deng, J.; Lou, J.; Yuan, J.; Si, Y.; Zhang, Z. Round window niche veil is visible on high-resolution computed tomography and a predictor of local drug efficacy to inner ear. Laryngoscope 2024, 134, 1396–1402. [Google Scholar] [CrossRef] [PubMed]
- Alzamil, K.S.; Linthicum Jr, F.H. Extraneous round window membranes and plugs: Possible effect on intratympanic therapy. Ann. Otol. Rhinol. Laryngol. 2000, 109, 30–32. [Google Scholar] [CrossRef]
- Silverstein, H.; Rowan, P.T.; Olds, M.J.; Rosenberg, S.I. Inner ear perfusion and the role of round window patency. Otol. Neurotol. 1997, 18, 586–589. [Google Scholar]
- Szeto, B.; Chiang, H.; Valentini, C.; Yu, M.; Kysar, J.W.; Lalwani, A.K. Inner ear delivery: Challenges and opportunities. Laryngoscope Investig. Otolaryngol. 2020, 5, 122–131. [Google Scholar] [CrossRef]
- Salt, A.N.; Hirose, K. Communication pathways to and from the inner ear and their contributions to drug delivery. Hear. Res. 2018, 362, 25–37. [Google Scholar] [CrossRef]
- Wei, C.; Gao, Z.; Knabel, M.; Ulbricht, M.; Senekowitsch, S.; Erfurt, P.; Maggi, N.; Zwick, B.; Eickner, T.; Matin-Mann, F. Development of a drug delivering round window niche implant for cochlear pharmacotherapy. Drug Deliv. 2024, 31, 2392755. [Google Scholar] [CrossRef]
- Matin, F.; Gao, Z.; Repp, F.; John, S.; Lenarz, T.; Scheper, V. Determination of the round window niche anatomy using cone beam computed tomography imaging as preparatory work for individualized drug-releasing implants. J. Imaging 2021, 7, 79. [Google Scholar] [CrossRef]
- Mau, R.; Eickner, T.; Jüttner, G.; Gao, Z.; Wei, C.; Fiedler, N.; Senz, V.; Lenarz, T.; Grabow, N.; Scheper, V. Micro Injection Molding of Drug-Loaded Round Window Niche Implants for an Animal Model Using 3D-Printed Molds. Pharmaceutics 2023, 15, 1584. [Google Scholar] [CrossRef]
- Farahmand Ghavi, F.; Mirzadeh, H.; Imani, M.; Jolly, C.; Farhadi, M. Corticosteroid-releasing cochlear implant: A novel hybrid of biomaterial and drug delivery system. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 94, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Bohl, A.; Rohm, H.W.; Ceschi, P.; Paasche, G.; Hahn, A.; Barcikowski, S.; Lenarz, T.; Stöver, T.; Pau, H.-W.; Schmitz, K.-P. Development of a specially tailored local drug delivery system for the prevention of fibrosis after insertion of cochlear implants into the inner ear. J. Mater. Sci. Mater. Med. 2012, 23, 2151–2162. [Google Scholar] [CrossRef] [PubMed]
- Malfeld, K.; Baumhoff, P.; Volk, H.A.; Lenarz, T.; Scheper, V. Local Long-Term Inner Ear Drug Delivery in Normal Hearing Guinea Pig—An Animal Model to Develop Preventive Treatment for Noise-Induced Hearing Loss. Biomolecules 2022, 12, 1427. [Google Scholar] [CrossRef] [PubMed]
- Behrends, W.; Wulf, K.; Raggl, S.; Fröhlich, M.; Eickner, T.; Dohr, D.; Esser, K.-H.; Lenarz, T.; Scheper, V.; Paasche, G. Dual Drug Delivery in Cochlear Implants: In Vivo Study of Dexamethasone Combined with Diclofenac or Immunophilin Inhibitor MM284 in Guinea Pigs. Pharmaceutics 2023, 15, 726. [Google Scholar] [CrossRef]
- Wilk, M.; Hessler, R.; Mugridge, K.; Jolly, C.; Fehr, M.; Lenarz, T.; Scheper, V. Impedance changes and fibrous tissue growth after cochlear implantation are correlated and can be reduced using a dexamethasone eluting electrode. PLoS ONE 2016, 11, e0147552. [Google Scholar] [CrossRef]
- Lexow, G.J.; Schurzig, D.; Gellrich, N.-C.; Lenarz, T.; Majdani, O.; Rau, T.S. Visualization, measurement and modelling of the cochlea using rotating midmodiolar slice planes. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1855–1869. [Google Scholar] [CrossRef]
- Nusil. MED-4244. 2018. Available online: https://nusil.avantorsciences.com/nusil/en/product/MED-4244/low-consistency-silicone-elastomer (accessed on 1 January 2021).
- Sigma-Aldrich. Safety Data Sheet. 2024. Available online: https://www.sigmaaldrich.com/DE/en/sds/sigma/d2915?userType=anonymous (accessed on 1 January 2021).
- Liebau, A.; Schilp, S.; Mugridge, K.; Schön, I.; Kather, M.; Kammerer, B.; Tillein, J.; Braun, S.; Plontke, S.K. Long-term in vivo release profile of dexamethasone-loaded silicone rods implanted into the cochlea of guinea pigs. Front. Neurol. 2020, 10, 1377. [Google Scholar] [CrossRef]
- Rongthong, T.; Qnouch, A.; Maue Gehrke, M.; Paccou, L.; Oliveira, P.; Danede, F.; Verin, J.; Vincent, C.; Willart, J.-F.; Siepmann, F. Silicone matrices for controlled dexamethasone release: Toward a better understanding of the underlying mass transport mechanisms. Regen. Biomater. 2023, 10, rbad008. [Google Scholar] [CrossRef]
- Rongthong, T.; Qnouch, A.; Gehrke, M.M.; Danede, F.; Willart, J.-F.; De Oliveira, P.; Paccou, L.; Tourrel, G.; Stahl, P.; Verin, J. Long term behavior of dexamethasone-loaded cochlear implants: In vitro & in vivo. Int. J. Pharm. X 2022, 4, 100141. [Google Scholar]
- Matin-Mann, F.; Gao, Z.; Schwieger, J.; Ulbricht, M.; Domsta, V.; Senekowitsch, S.; Weitschies, W.; Seidlitz, A.; Doll, K.; Stiesch, M. Individualized, additively manufactured drug-releasing external ear canal implant for prevention of postoperative restenosis: Development, in vitro testing, and proof of concept in an individual curative trial. Pharmaceutics 2022, 14, 1242. [Google Scholar] [CrossRef]
- Sircoglou, J.; Gehrke, M.; Tardivel, M.; Siepmann, F.; Siepmann, J.; Vincent, C. Trans-oval-window implants, a new approach for drug delivery to the inner ear: Extended dexamethasone release from silicone-based implants. Otol. Neurotol. 2015, 36, 1572–1579. [Google Scholar] [CrossRef] [PubMed]
- Qnouch, A.; Solarczyk, V.; Verin, J.; Tourrel, G.; Stahl, P.; Danede, F.; Willart, J.-F.; Lemesre, P.-E.; Vincent, C.; Siepmann, J. Dexamethasone-loaded cochlear implants: How to provide a desired “burst release”. Int. J. Pharm. X 2021, 3, 100088. [Google Scholar] [CrossRef] [PubMed]
- Peppas, N.A.; Narasimhan, B. Mathematical models in drug delivery: How modeling has shaped the way we design new drug delivery systems. J. Control. Release 2014, 190, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Langer, R.S.; Peppas, N.A. Present and future applications of biomaterials in controlled drug delivery systems. Biomaterials 1981, 2, 201–214. [Google Scholar] [CrossRef]
- Hahn, H.; Kammerer, B.; DiMauro, A.; Salt, A.N.; Plontke, S.K. Cochlear microdialysis for quantification of dexamethasone and fluorescein entry into scala tympani during round window administration. Hear. Res. 2006, 212, 236–244. [Google Scholar] [CrossRef]
- Du, X.; Chen, K.; Kuriyavar, S.; Kopke, R.D.; Grady, B.P.; Bourne, D.H.; Li, W.; Dormer, K.J. Magnetic targeted delivery of dexamethasone acetate across the round window membrane in guinea pigs. Otol. Neurotol. 2013, 34, 41–47. [Google Scholar] [CrossRef]
- Li, X.; Chen, W.-J.; Xu, J.; Yi, H.-J.; Ye, J.-Y. Clinical analysis of intratympanic injection of dexamethasone for treating sudden deafness. Int. J. Gen. Med. 2021, 14, 2575–2579. [Google Scholar] [CrossRef]
- Wang, X.; Dellamary, L.; Fernandez, R.; Ye, Q.; LeBel, C.; Piu, F. Principles of inner ear sustained release following intratympanic administration. Laryngoscope 2011, 121, 385–391. [Google Scholar] [CrossRef]
- Honeder, C.; Ahmadi, N.; Kramer, A.-M.; Zhu, C.; Saidov, N.; Arnoldner, C. Cochlear implantation in the guinea pig. JoVE (J. Vis. Exp.) 2018, 136, e56829. [Google Scholar]
- Plontke, S.K.; Biegner, T.; Kammerer, B.; Delabar, U.; Salt, A.N. Dexamethasone concentration gradients along scala tympani after application to the round window membrane. Otol. Neurotol. 2008, 29, 401–406. [Google Scholar] [CrossRef]
- Salt, A.N.; Plontke, S.K. Pharmacokinetic principles in the inner ear: Influence of drug properties on intratympanic applications. Hear. Res. 2018, 368, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Forouzandeh, F.; Borkholder, D.A. Microtechnologies for inner ear drug delivery. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, R.K.; Xu, J. A multichannel scala tympani electrode array incorporating a drug delivery system for chronic intracochlear infusion. Hear. Res. 2002, 172, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Sumner, L.; Mestel, J.; Reichenbach, T. Steady streaming as a method for drug delivery to the inner ear. Sci. Rep. 2021, 11, 57. [Google Scholar] [CrossRef]
- Geerardyn, A.; Zhu, M.; Wu, P.; O’Malley, J.T.; Nadol Jr, J.B.; Liberman, M.C.; Nakajima, H.H.; Verhaert, N.; Quesnel, A.M. Three-dimensional quantification of fibrosis and ossification after cochlear implantation via virtual re-sectioning: Potential implications for residual hearing. Hear. Res. 2023, 428, 108681. [Google Scholar] [CrossRef]
- Tanaka, C.; Nguyen-Huynh, A.; Loera, K.; Stark, G.; Reiss, L. Factors associated with hearing loss in a normal-hearing guinea pig model of hybrid cochlear implants. Hear. Res. 2014, 316, 82–93. [Google Scholar] [CrossRef]
- Clark, G.M.; Shute, S.; Shepherd, R.; Carter, T. Cochlear implantation: Osteoneogenesis, electrode-tissue impedance, and residual hearing. Ann. Otol. Rhinol. Laryngol. Suppl. 1995, 166, 40–42. [Google Scholar]
- Duan, Y.; Clark, G.; Cowan, R. A study of intra-cochlear electrodes and tissue interface by electrochemical impedance methods in vivo. Biomaterials 2004, 25, 3813–3828. [Google Scholar] [CrossRef]
- Scheper, V.; Hoffmann, A.; Gepp, M.M.; Schulz, A.; Hamm, A.; Pannier, C.; Hubka, P.; Lenarz, T.; Schwieger, J. Stem cell based drug delivery for protection of auditory neurons in a guinea pig model of cochlear implantation. Front. Cell. Neurosci. 2019, 13, 177. [Google Scholar] [CrossRef]
- Burghard, A.; Lenarz, T.; Kral, A.; Paasche, G. Insertion site and sealing technique affect residual hearing and tissue formation after cochlear implantation. Hear. Res. 2014, 312, 21–27. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ranking Score | Fibrotic Growth |
|---|---|
| 0 | none |
| 1 | 1 to 2 cell layers |
| 2 | thick cell layers |
| 3 | scala tympani filled up completely |
| RNI | 1 | 2 | 3 |
|---|---|---|---|
| Mass (mg) | 0.83 | 0.81 | 0.86 |
| Calculated DEX amount (mg) | 0.083 | 0.081 | 0.086 |
| 1 kHz | 2 kHz | 4 kHz | 8 kHz | 16 kHz | 32 kHz | 40 kHz | |
|---|---|---|---|---|---|---|---|
| CI | 4.17 ± 4.9 | 6.67 ± 10.8 | 17.5 ± 14.75 | 24.17 ± 23.33 | 33.33 ± 20.9 | 40 ± 14.14 | 41.67 ± 12.52 |
| CI + RNI | 3 ± 9.08 | 15 ± 10.61 | 16 ± 16.36 | 25 ± 18.71 | 31 ± 10.84 | 10 ± 18.71 | 19 ± 13.87 |
| CI | CI + RNI | |
|---|---|---|
| Contact K1 | 3.3 ± 4 | 1.6 ± 1.8 |
| Contact K2 | 0 ± 0.2 | 1.8 ± 1.3 |
| Contact K3 | 3.4 ± 5.8 | 3.3 ± 4.4 |
| Contact K4 | 3 ± 2.5 | 0.3 ± 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, C.; Gao, Z.; Mau, R.; Eickner, T.; Jüttner, G.; Fiedler, N.; Seitz, H.; Lenarz, T.; Scheper, V. Molded Round Window Niche Implant as a Dexamethasone Delivery System in a Cochlear Implant-Trauma Animal Model. Pharmaceutics 2024, 16, 1236. https://doi.org/10.3390/pharmaceutics16091236
Wei C, Gao Z, Mau R, Eickner T, Jüttner G, Fiedler N, Seitz H, Lenarz T, Scheper V. Molded Round Window Niche Implant as a Dexamethasone Delivery System in a Cochlear Implant-Trauma Animal Model. Pharmaceutics. 2024; 16(9):1236. https://doi.org/10.3390/pharmaceutics16091236
Chicago/Turabian StyleWei, Chunjiang, Ziwen Gao, Robert Mau, Thomas Eickner, Gabor Jüttner, Nicklas Fiedler, Hermann Seitz, Thomas Lenarz, and Verena Scheper. 2024. "Molded Round Window Niche Implant as a Dexamethasone Delivery System in a Cochlear Implant-Trauma Animal Model" Pharmaceutics 16, no. 9: 1236. https://doi.org/10.3390/pharmaceutics16091236
APA StyleWei, C., Gao, Z., Mau, R., Eickner, T., Jüttner, G., Fiedler, N., Seitz, H., Lenarz, T., & Scheper, V. (2024). Molded Round Window Niche Implant as a Dexamethasone Delivery System in a Cochlear Implant-Trauma Animal Model. Pharmaceutics, 16(9), 1236. https://doi.org/10.3390/pharmaceutics16091236