
Advanced Denoising and Meta-Learning Techniques for Enhancing Smart Health Monitoring Using Wearable Sensors

 ,
,  , , and
, , and 
Abstract
:1. Introduction
- The proposed meta-learning method is appropriate to empower AI, since biomedical wearable sensor data collection is expensive, challenging, or inadequate.
- An advanced multi-level denoising technique has been implemented and demonstrated for smoothing the noise signals and improving the performance of the proposed meta-learning model.
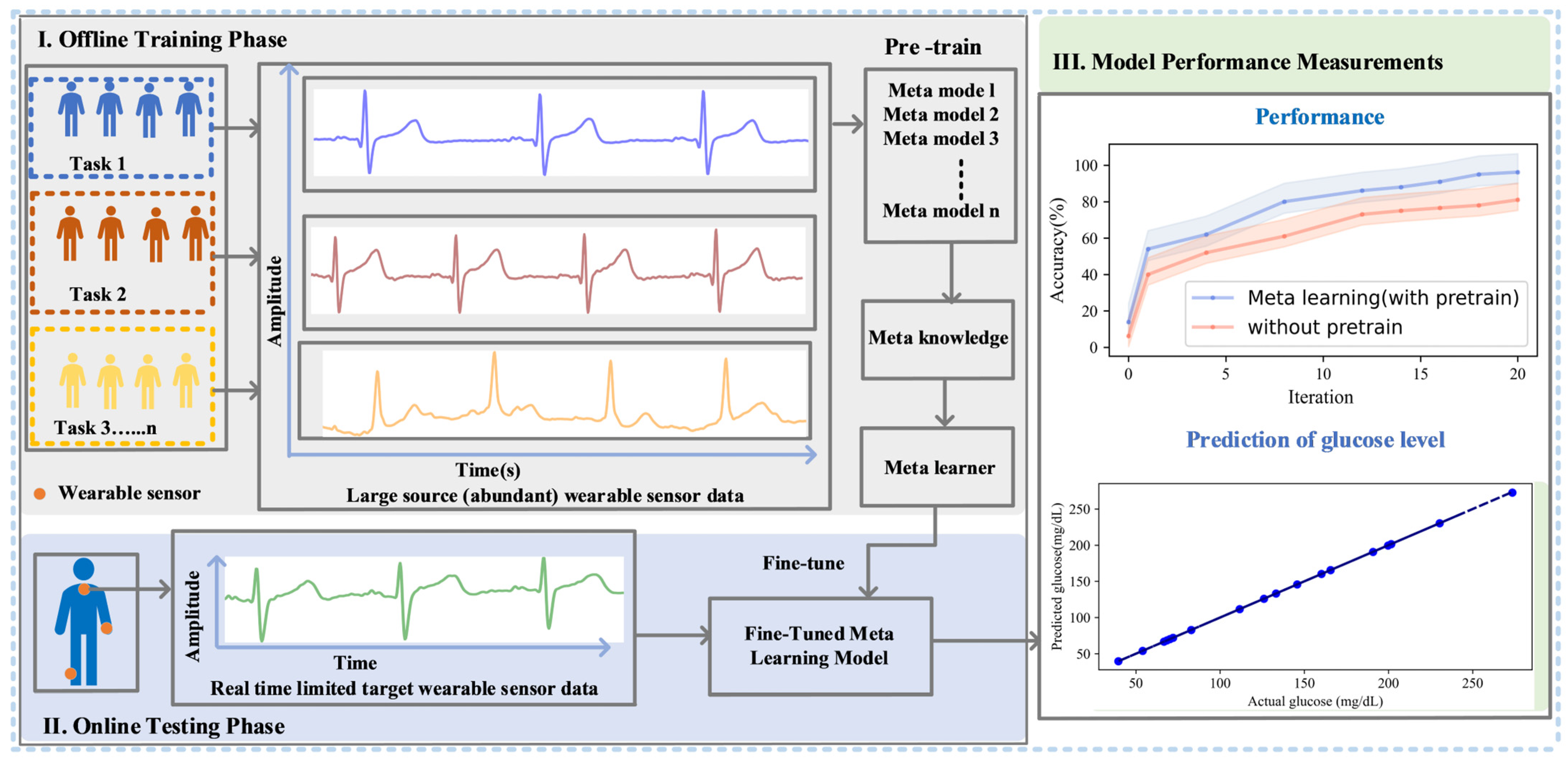
- The proposed meta-learning system significantly improves disease detection accuracy and efficiency while enabling adaptation to new data and learning from limited samples. It streamlines the training of predictive models for health wearables, enhancing efficiency and adaptability to new health tasks or patient conditions by leveraging diverse source datasets.
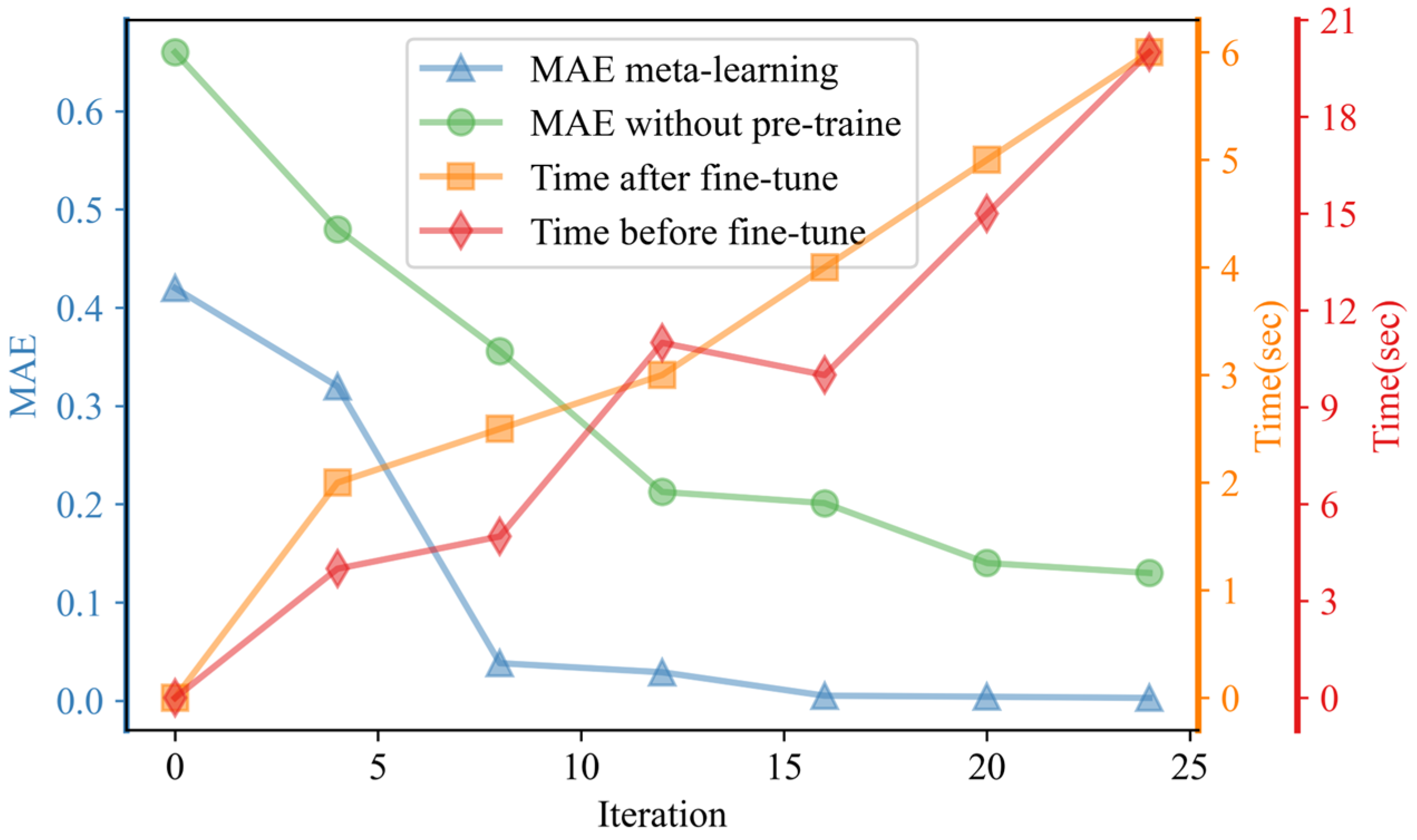
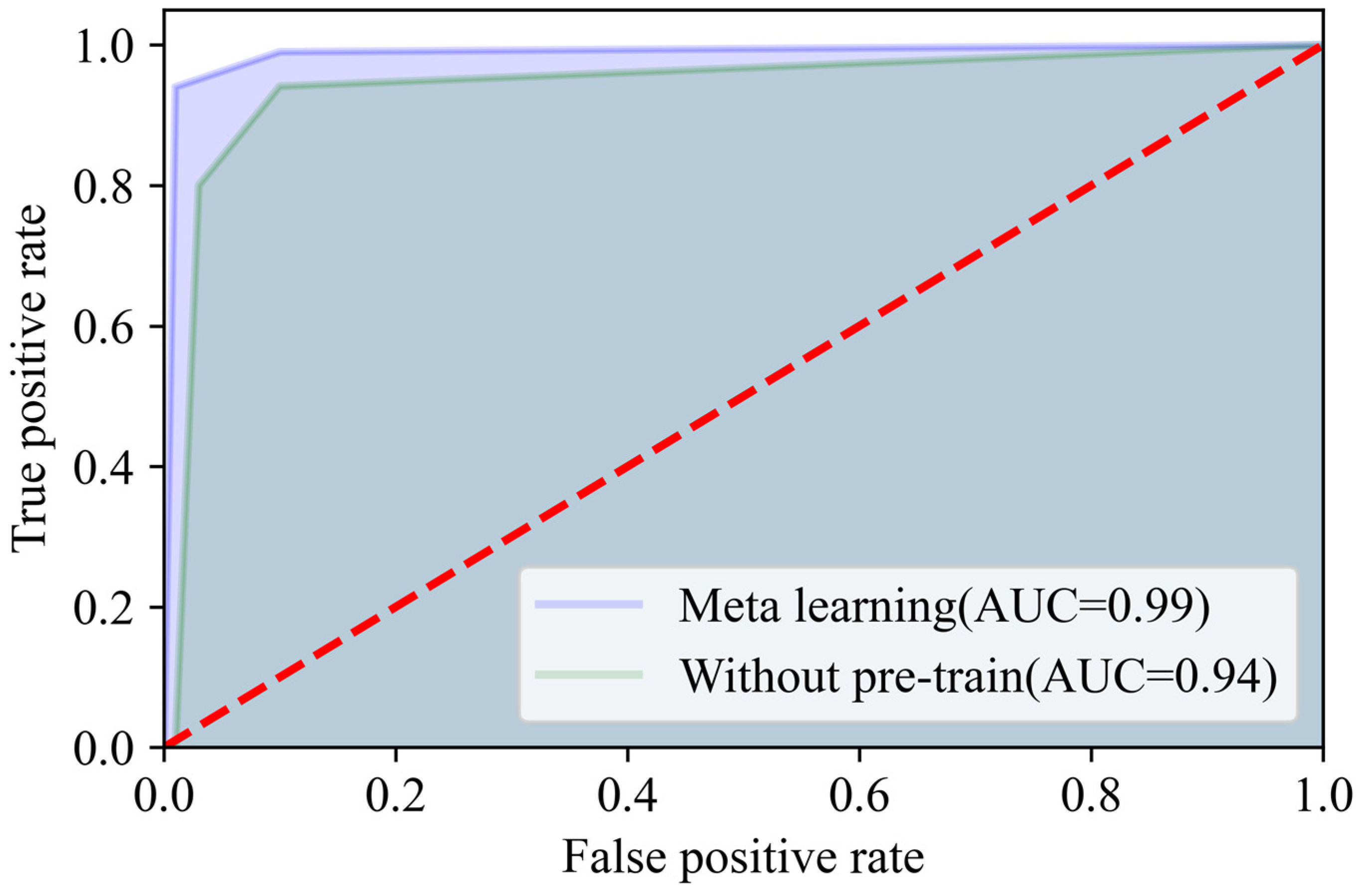
- After conducting comprehensive experiments and comparative analyses, meta-learning demonstrated significant outperformance compared to traditional methods without pre-training. This leads to a marked improvement in diabetes detection performance in healthcare monitoring systems.
2. Methodology
2.1. Data Collection
Signal Processing
2.2. Proposed Discrete Wavelet Transform (DWT)
- Collect the original noisy data.
- Apply the wavelet transform to the data.
- Set the level of decomposition for wavelet decomposition.
- Perform threshold processing.
- Reconstruct the signal.
- Finally, the noise in the signal is reduced.
2.3. Proposed Meta-Learning Model
3. Results and Discussion
4. Performance Comparison Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- De Fazio, R.; Mastronardi, V.M.; De Vittorio, M.; Visconti, P. Wearable Sensors and Smart Devices to Monitor Rehabilitation Parameters and Sports Performance: An Overview. Sensors 2023, 23, 1856. [Google Scholar] [CrossRef] [PubMed]
- Mosenia, A.; Sur-Kolay, S.; Raghunathan, A.; Jha, N.K. Wearable Medical Sensor-Based System Design: A Survey. IEEE Trans. Multi-Scale Comput. Syst. 2017, 3, 124–138. [Google Scholar] [CrossRef]
- Manikandan, M.S.; Soman, K.P. A novel method for detecting R-peaks in electrocardiogram (ECG) signal. Biomed. Signal Process. 2012, 7, 118–128. [Google Scholar] [CrossRef]
- Zhu, T.; Li, K.; Herrero, P.; Georgiou, P. Deep Learning for Diabetes: A Systematic Review. IEEE J. Biomed. Health Inform. 2021, 25, 2744–2757. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Zeb, K.; Al-Rakhami, M.; Derhab, A.; Bukhari, S.A.C. Detection and Prediction of Diabetes Using Data Mining: A Comprehensive Review. IEEE Access 2021, 9, 43711–43735. [Google Scholar] [CrossRef]
- Site, A.; Nurmi, J.; Lohan, E.S. Systematic Review on Machine-Learning Algorithms Used in Wearable-Based eHealth Data Analysis. IEEE Access 2021, 9, 112221–112235. [Google Scholar] [CrossRef]
- Site, A.; Nurmi, J.; Lohan, E.S. Machine-Learning-Based Diabetes Prediction Using Multisensor Data. IEEE Sens. J. 2023, 23, 28370–28377. [Google Scholar] [CrossRef]
- Yan, K.; Zhang, D.; Wu, D.; Wei, H.; Lu, G. Design of a breath analysis system for diabetes screening and blood glucose level prediction. IEEE Trans. Biomed. Eng. 2014, 61, 2787–2795. [Google Scholar] [CrossRef]
- Van Rahmani, A.M.; Yousefpoor, E.; Yousefpoor, M.S.; Mehmood, Z.; Haider, A.; Hosseinzadeh, M.; Ali Naqvi, R. Machine Learning (ML) in Medicine: Review, Applications, and Challenges. Mathematics 2021, 9, 2970. [Google Scholar] [CrossRef]
- Wang, L.; Mu, Y.; Zhao, J.; Wang, X.; Che, H. Igrnet: A deep learning model for non-invasive, real-time diagnosis of prediabetes through electrocardiograms. Sensors 2020, 20, 2556. [Google Scholar] [CrossRef]
- Larabi-Marie-Sainte, S.; Aburahmah, L.; Almohaini, R.; Saba, T. Current Techniques for Diabetes Prediction: Review and Case Study. Appl. Sci. 2019, 9, 4604. [Google Scholar] [CrossRef]
- Gevaert, O. Meta-Learning Reduces the Amount of Data Needed to Build AI Models in Oncology. Br. J. Cancer 2021, 125, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Qiu, L.; Ren, Y.; Cheng, Z.; Li, L.; Yao, S.; Zhang, C.; Luo, Z.; Lu, H. A meta-learning approach to improving radiation response prediction in cancers. Comput. Biol. Med. 2022, 150, 106163. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Vettoruzzo, A.; Bouguelia, M.-R.; Vanschoren, J.; Rognvaldsson, T.; Santosh, K.C. Advances and Challenges in Meta-Learning: A Technical Review. IEEE Trans. Pattern Anal. Mach. Intell. 2024, 46, 1–20. [Google Scholar] [CrossRef]
- Tefera, M.A.; Manie, Y.C.; Yao, C.-K.; Fan, T.-P.; Peng, P.-C. Meta-Learning for Boosting the Sensing Quality and Utility of FSO-Based Multichannel FBG Sensor System. IEEE Sens. J. 2023, 23, 31506–31512. [Google Scholar] [CrossRef]
- Vanschoren, J. Meta-Learning: A Survey. arXiv 2018, arXiv:1810.03548. [Google Scholar]
- Manie, Y.C.; Li, J.W.; Peng, P.C.; Shiu, R.K.; Chen, Y.Y.; Hsu, Y.T. Using a Machine Learning Algorithm Integrated with Data De-Noising Techniques to Optimize the Multipoint Sensor Network. Sensors 2020, 20, 1070. [Google Scholar] [CrossRef]
- Arsene, C.T.; Hankins, R.; Yin, H. Deep learning models for denoising ECG signals. In Proceedings of the 2019 27th European Signal Processing Conference (EUSIPCO), A Coruna, Spain, 2–6 September 2019; pp. 1–5. [Google Scholar]
- Mishra, A.; Dharahas, G.; Gite, S.; Kotecha, K.; Koundal, D.; Zaguia, A.; Kaur, M.; Lee, H.-N. ECG Data Analysis with Denoising Approach and Customized CNNs. Sensors 2022, 22, 1928. [Google Scholar] [CrossRef]
- Dubosson, F.; Ranvier, J.-E.; Bromuri, S.; Calbimonte, J.-P.; Ruiz, J.; Schumacher, M. The open D1NAMO dataset: A multi-modal dataset for research on non-invasive type 1 diabetes management. Inform. Med. Unlocked 2018, 13, 92–100. [Google Scholar] [CrossRef]
- Xiao, Q.; Lee, K.; Mokhtar, S.A.; Ismail, I.; Pauzi, A.L.b.M.; Zhang, Q.; Lim, P.Y. Deep Learning-Based ECG Arrhythmia Classification: A Systematic Review. Appl. Sci. 2023, 13, 4964. [Google Scholar] [CrossRef]
- Uwaechia, A.N.; Ramli, D.A. A Comprehensive Survey on ECG Signals as New Biometric Modality for Human Authentication: Recent Advances and Future Challenges. IEEE Access 2021, 9, 97760–97802. [Google Scholar] [CrossRef]
- Manie, Y.C.; Yao, C.K.; Peng, P.C. Free-Space Optical and Optical Networks. In Handbook of Radio and Optical Networks Convergence; Kawanishi, T., Ed.; Springer: Singapore, 2024; pp. 1–32. [Google Scholar]
- Dehnaw, A.M.; Manie, Y.C.; Du, L.-Y.; Yao, C.-K.; Li, Y.-L.; Hayle, S.T.; Peng, P.-C. Bidirectional Free Space Optics Communication for Long-Distance Sensor System. J. Light. Technol. 2023, 41, 5870–5878. [Google Scholar] [CrossRef]
- Swapna, G.; Soman, K.P.; Vinayakumar, R. Automated detection of diabetes using CNN and CNN-LSTM network and heart rate signals. Procedia Comput. Sci. 2018, 132, 1253–1262. [Google Scholar]
- Li, J.; Igbe, T.; Liu, Y.; Kandwal, A.; Wang, L.; Nie, Z. Non-invasive monitoring of three glucose ranges based on ECG by using DBSCAN-CNN. IEEE J. Biomed. Health Inform. 2021, 25, 3340–3350. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Bajaj, V. A Robust Framework for Automated Screening of Diabetic Patient Using ECG Signals. IEEE Sens. J. 2022, 22, 24222–24229. [Google Scholar] [CrossRef]
- Aggarwal, Y.; Das, J.; Mazumder, P.M.; Kumar, R.; Sinha, R.K. Heart rate variability features from nonlinear cardiac dynamics in identification of diabetes using artificial neural network and support vector machine. Biocybern. Biomed. Eng. 2020, 40, 1002–1009. [Google Scholar] [CrossRef]
- Choudhury, A.; Gupta, D. A Survey on Medical Diagnosis of Diabetes Using Machine Learning Techniques. In Recent Developments in Machine Learning and Data Analytics; Springer: Singapore, 2019; pp. 67–68. [Google Scholar]
- Saxena, R.; Sharma, S.K.; Gupta, M.; Sampada, G.C. A Comprehensive Review of Various Diabetic Prediction Models: A Literature Survey. J. Healthc. Eng. 2022, 2022, e8100697. [Google Scholar] [CrossRef]
- Pati, A.; Parhi, M.; Pattanayak, B.K. A review on prediction of diabetes using machine learning and data mining classification techniques. Int. J. Biomed. Eng. Technol. 2023, 41, 83–109. [Google Scholar] [CrossRef]
- Vijayan, V.V.; Anjali, C. Prediction and diagnosis of diabetes mellitus—A machine learning approach. In Proceedings of the 2015 IEEE Recent Advances in Intelligent Computational Systems (RAICS), Trivandrum, India, 10–12 December 2015; pp. 122–127. [Google Scholar]
- Cordeiro, R.; Karimian, N.; Park, Y. Hyperglycemia Identification Using ECG in Deep Learning Era. Sensors 2021, 21, 6263. [Google Scholar] [CrossRef]
- Arbi, K.F.; Soulimane, S.; Saffih, F.; Bechar, M.A.; Azzoug, O. Blood Glucose Estimation Based on ECG Signal. Phys. Eng. Sci. Med. 2023, 46, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Dénes-Fazakas, L.; Siket, M.; Szilágyi, L.; Kovács, L.; Eigner, G. Detection of Physical Activity Using Machine Learning Methods Based on Continuous Blood Glucose Monitoring and Heart Rate Signals. Sensors 2022, 22, 8568. [Google Scholar] [CrossRef]
- Park, J.-U.; Kim, Y.; Lee, Y.; Urtnasan, E.; Lee, K.-J. A Prediction Algorithm for Hypoglycemia Based on Support Vector Machine Using Glucose Level and Electrocardiogram. J. Med. Syst. 2022, 46, 10. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method and Reference | Accuracy |
|---|---|
| IGRNet [10] | 78.1% |
| DNN [34] | 94.53 |
| Exponential GPR and CNN [35] | 94% |
| Logistic Regression [36] | 92.2% |
| SVM [37] | 89% |
| Without pre-train (in this paper) | 81% |
| Meta-learning without DWT denoising (in this paper) | 85% |
| Meta-learning with DWT denoising (Proposed) | 96.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tefera, M.A.; Dehnaw, A.M.; Manie, Y.C.; Yao, C.-K.; Bogale, S.D.; Peng, P.-C. Advanced Denoising and Meta-Learning Techniques for Enhancing Smart Health Monitoring Using Wearable Sensors. Future Internet 2024, 16, 280. https://doi.org/10.3390/fi16080280
Tefera MA, Dehnaw AM, Manie YC, Yao C-K, Bogale SD, Peng P-C. Advanced Denoising and Meta-Learning Techniques for Enhancing Smart Health Monitoring Using Wearable Sensors. Future Internet. 2024; 16(8):280. https://doi.org/10.3390/fi16080280
Chicago/Turabian StyleTefera, Minyechil Alehegn, Amare Mulatie Dehnaw, Yibeltal Chanie Manie, Cheng-Kai Yao, Shegaw Demessie Bogale, and Peng-Chun Peng. 2024. "Advanced Denoising and Meta-Learning Techniques for Enhancing Smart Health Monitoring Using Wearable Sensors" Future Internet 16, no. 8: 280. https://doi.org/10.3390/fi16080280