Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
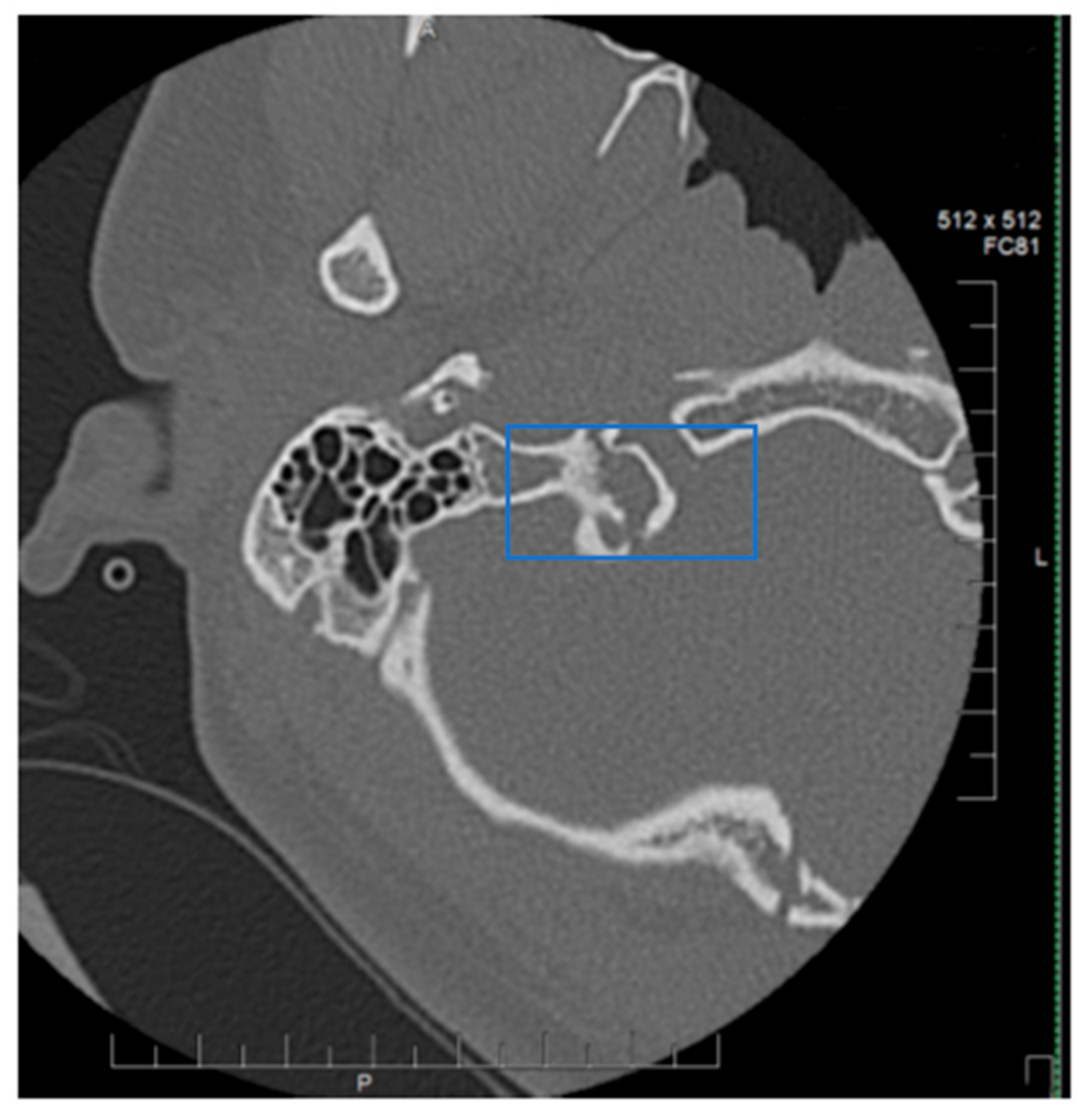
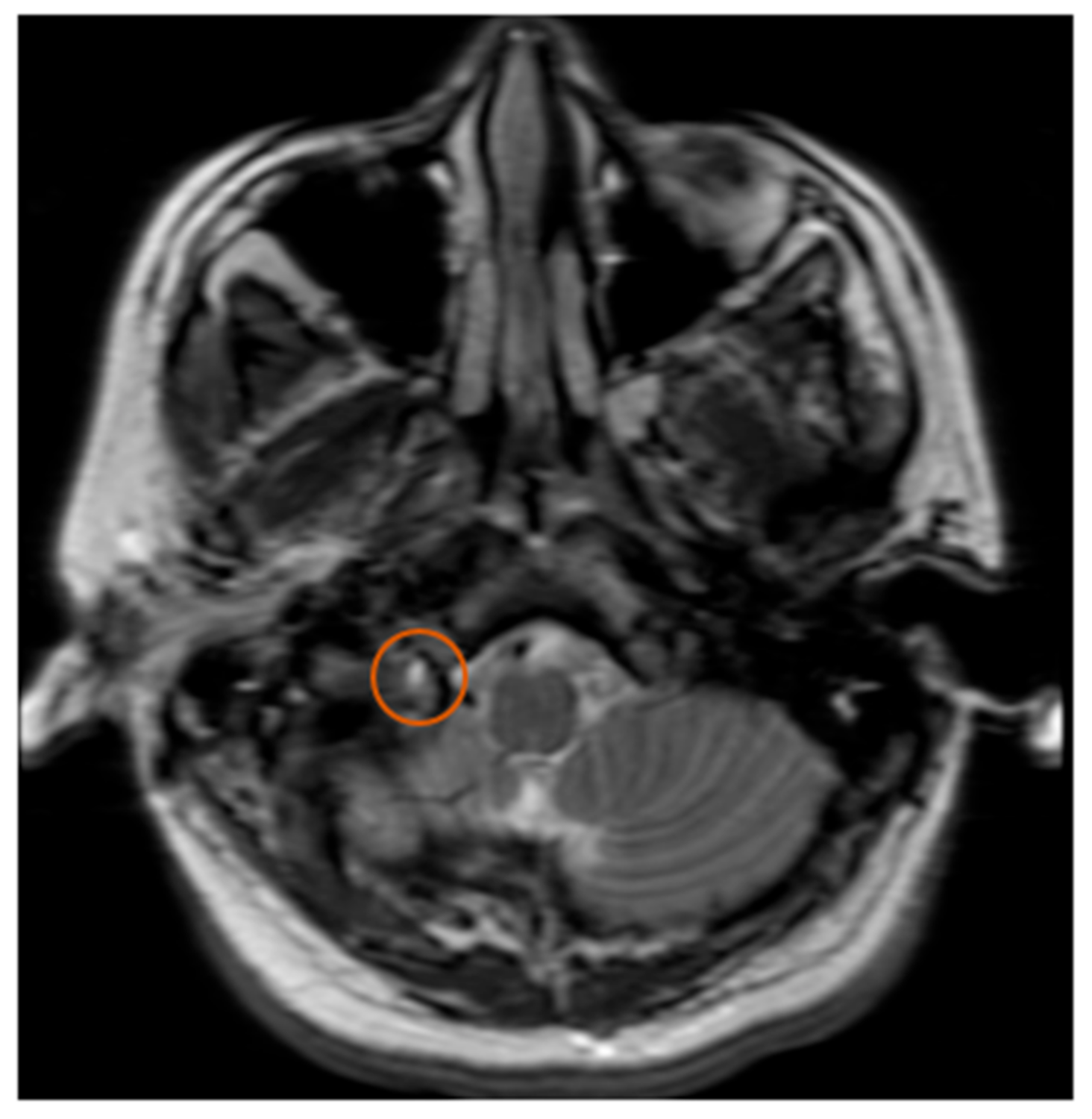
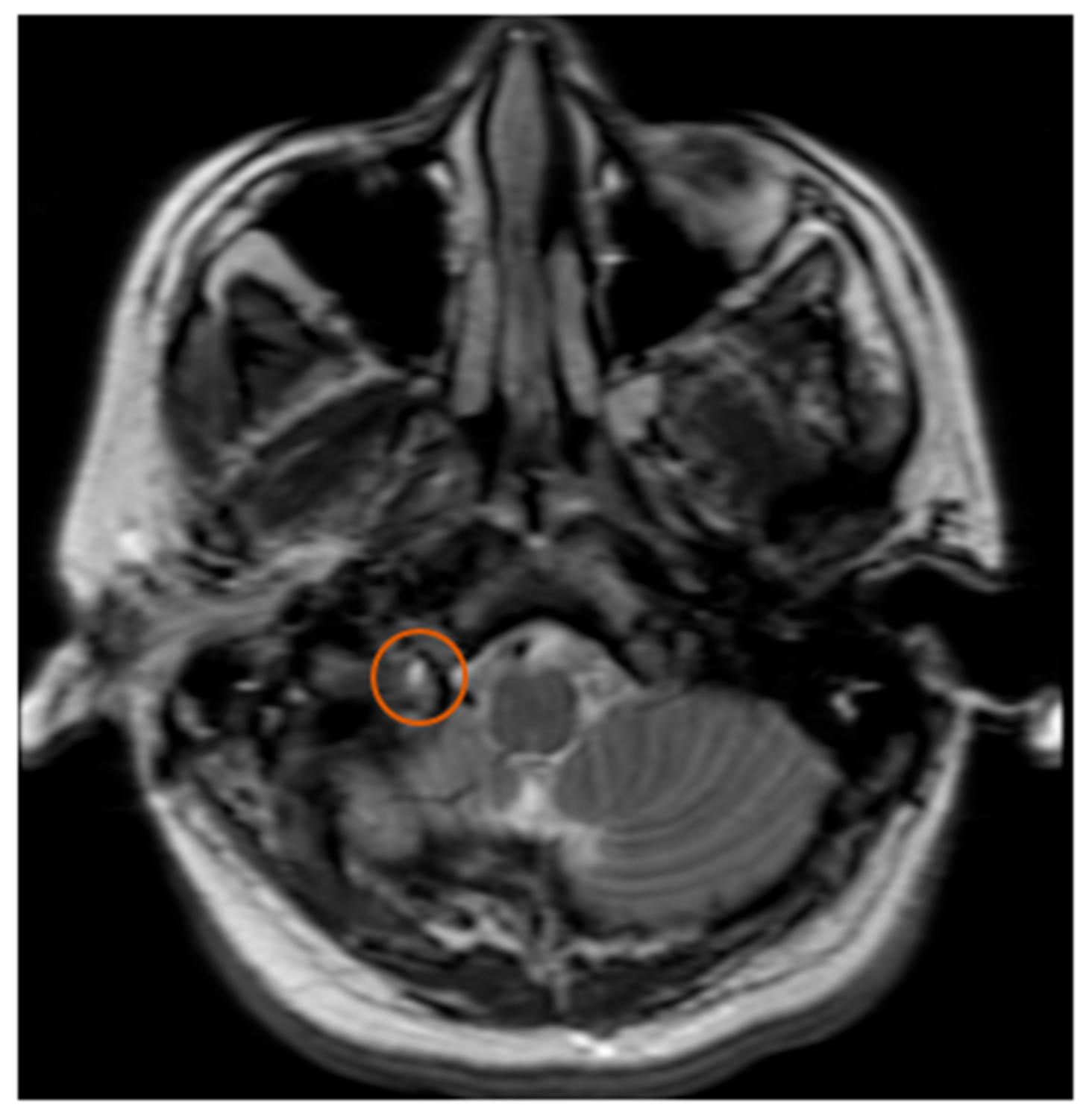
2. Case Report
3. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Collet, F.J. Sur un nouveau syndrome paralytique pharyngo-laryngé par blessures du guerre (hemiplegia glosso-laryngo-scapulo-pharyngée). Lyon Méd. 1915, 124, 121–1292. [Google Scholar]
- Sicard, J.A. Syndrome du carrefour condylo-déchiré postérieur (type pur de paralysie des quatre derniers nerfs crâniens). Mars. Méd. 1917, 53, 385–397. [Google Scholar]
- Neo, S.; Lee, K.E. Collet-Sicard syndrome: A rare but important presentation of internal jugular vein thrombosis. Pr. Neurol. 2016, 17, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Oushy, S.; Graffeo, C.S.; Perry, A.; Morris, J.M.; Carlson, M.L.; Van Gompel, J.J. Collet-Sicard Syndrome Attributable to Extramedullary Plasmacytoma of the Jugular Foramen. World Neurosurg. 2018, 110, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Larsen, Á.; Feria-Vilar, I.; Collado, R.; Segura, T. Síndrome de Collet-Sicard metastásico. Neurología 2017, 32, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.S.; Coumas, J.M.; Danylevich, A.; Hayes, E.; Dunn, E.J. Fracture of the occipital condyle: Case report and review of the literature. J. Trauma: Inj. Infect. Crit. Care 1990, 30, 240–241. [Google Scholar] [CrossRef]
- Bridgman, S.A.; McNab, W. Traumatic occipital condyle fracture, multiple cranial nerve palsies, and torticollis: A case report and review of the literature. Surg. Neurol. 1992, 38, 152–156. [Google Scholar] [CrossRef]
- Orbay, T.; Aykol, S.; Seckin, Z.; Ergun, R. Late hypoglossal nerve palsy following fracture of the occipital condyle. Surg. Neurol. 1989, 31, 402–404. [Google Scholar] [CrossRef]
- Kato, M.; Tanaka, Y.; Toyoda, I.; Ogura, S.; Yoshimura, S.; Iwama, T. Delayed lower cranial nerve palsy (Collet–Sicard syndrome) after head injury. Inj. Extra 2006, 37, 104–108. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamrazian, E.; Mehta, B. Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma. Neurol. Int. 2020, 12, 136-139. https://doi.org/10.3390/neurolint12030019
Tamrazian E, Mehta B. Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma. Neurology International. 2020; 12(3):136-139. https://doi.org/10.3390/neurolint12030019
Chicago/Turabian StyleTamrazian, Eric, and Bijal Mehta. 2020. "Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma" Neurology International 12, no. 3: 136-139. https://doi.org/10.3390/neurolint12030019
APA StyleTamrazian, E., & Mehta, B. (2020). Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma. Neurology International, 12(3), 136-139. https://doi.org/10.3390/neurolint12030019