

Humoral Response to SARS-CoV-2 Antigen in Patients Treated with Monoclonal Anti-CD20 Antibodies: It Is Not All about B Cell Recovery

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment and Data Extraction
- -
- anti-spike IgG titers following recall SARS-CoV-2 contact increased compared to anti-CD20 pre-treatment levels;
- -
- anti-CD20 therapy was ongoing for ≥12 months prior to the recall antigen exposure and to the respective anti-spike IgG assessment.
2.2. Laboratory Parameters
2.3. Statistics
2.4. Ethics
3. Results
3.1. Demographics
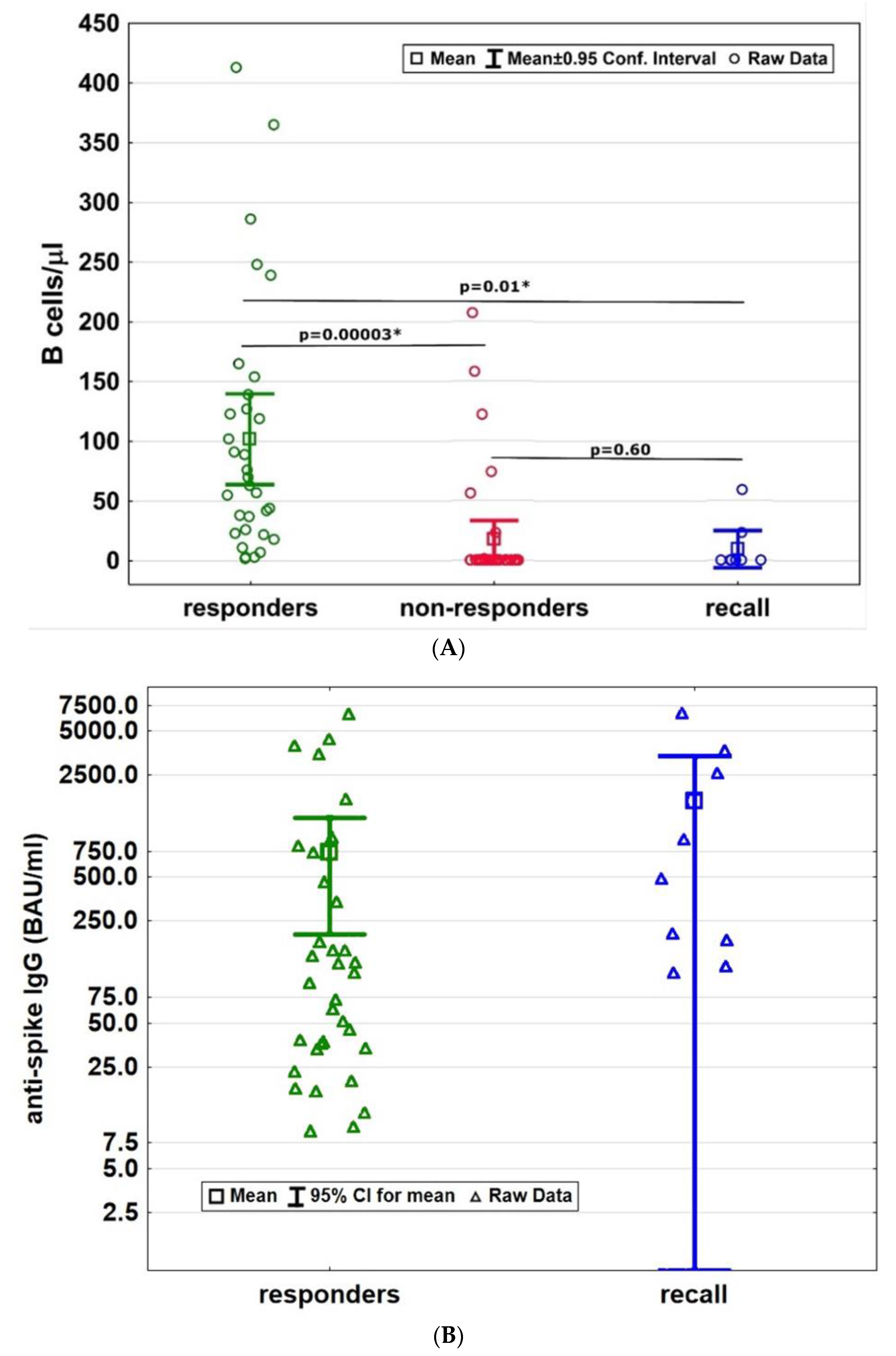
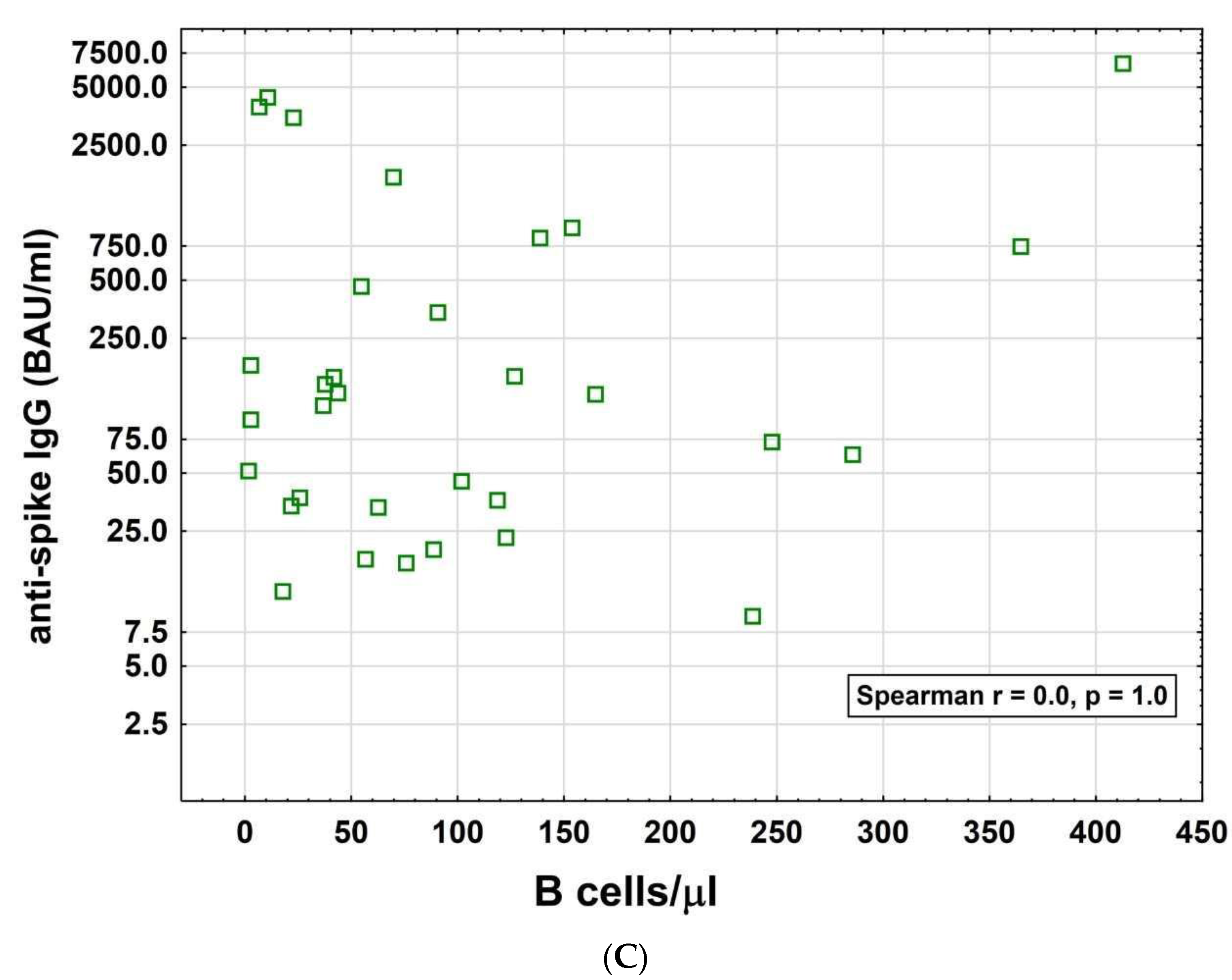
3.2. B Cell Recovery and Humoral Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hohlfeld, R. B-cells as therapeutic targets in neuro-inflammatory diseases. Clin. Immunol. 2018, 186, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Montalban, X.; Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Comi, G.; de Seze, J.; Giovannoni, G.; Hartung, H.P.; Hemmer, B.; et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Waubant, E.; Arnold, D.L.; Vollmer, T.; Antel, J.; Fox, R.J.; Bar-Or, A.; Panzara, M.; Sarkar, N.; Agarwal, S.; et al. B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. N. Engl. J. Med. 2008, 358, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; De Rossi, N.; Schiavetti, I.; Carmisciano, L.; Cordioli, C.; Moiola, L.; Radaelli, M.; Immovilli, P.; Capobianco, M.; Trojano, M.; et al. Disease-Modifying Therapies and Coronavirus Disease 2019 Severity in Multiple Sclerosis. Ann. Neurol. 2021, 89, 780–789. [Google Scholar] [CrossRef]
- Louapre, C.; Maillart, E.; Papeix, C.; Zeidan, S.; Biotti, D.; Lepine, Z.; Wahab, A.; Zedet, M.; Labauge, P.; Tilikete, C.; et al. Outcomes of coronavirus disease 2019 in patients with neuromyelitis optica and associated disorders. Eur. J. Neurol. 2021, 28, 3461–3466. [Google Scholar] [CrossRef]
- Luna, G.; Alping, P.; Burman, J.; Fink, K.; Fogdell-Hahn, A.; Gunnarsson, M.; Hillert, J.; Langer-Gould, A.; Lycke, J.; Nilsson, P.; et al. Infection Risks Among Patients With Multiple Sclerosis Treated With Fingolimod, Natalizumab, Rituximab, and Injectable Therapies. JAMA Neurol. 2020, 77, 184–191. [Google Scholar] [CrossRef]
- Simpson-Yap, S.; De Brouwer, E.; Kalincik, T.; Rijke, N.; Hillert, J.A.; Walton, C.; Edan, G.; Moreau, Y.; Spelman, T.; Geys, L.; et al. Associations of Disease-Modifying Therapies With COVID-19 Severity in Multiple Sclerosis. Neurology 2021, 97, e1870–e1885. [Google Scholar] [CrossRef]
- Louapre, C.; Ibrahim, M.; Maillart, E.; Abdi, B.; Papeix, C.; Stankoff, B.; Dubessy, A.L.; Bensa-Koscher, C.; Creange, A.; Chamekh, Z.; et al. Anti-CD20 therapies decrease humoral immune response to SARS-CoV-2 in patients with multiple sclerosis or neuromyelitis optica spectrum disorders. J. Neurol. Neurosurg. Psychiatry 2022, 93, 24–31. [Google Scholar] [CrossRef]
- Zabalza, A.; Cardenas-Robledo, S.; Tagliani, P.; Arrambide, G.; Otero-Romero, S.; Carbonell-Mirabent, P.; Rodriguez-Barranco, M.; Rodriguez-Acevedo, B.; Restrepo Vera, J.L.; Resina-Salles, M.; et al. COVID-19 in multiple sclerosis patients: Susceptibility, severity risk factors and serological response. Eur. J. Neurol. 2021, 28, 3384–3395. [Google Scholar] [CrossRef]
- Apostolidis, S.A.; Kakara, M.; Painter, M.M.; Goel, R.R.; Mathew, D.; Lenzi, K.; Rezk, A.; Patterson, K.R.; Espinoza, D.A.; Kadri, J.C.; et al. Cellular and humoral immune responses following SARS-CoV-2 mRNA vaccination in patients with multiple sclerosis on anti-CD20 therapy. Nat. Med. 2021, 27, 1990–2001. [Google Scholar] [CrossRef]
- Baker, D.; MacDougall, A.; Kang, A.S.; Schmierer, K.; Giovannoni, G.; Dobson, R. Seroconversion following COVID-19 vaccination: Can we optimize protective response in CD20-treated individuals? Clin. Exp. Immunol. 2022, 207, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Moser, T.; O’Sullivan, C.; Otto, F.; Hitzl, W.; Pilz, G.; Schwenker, K.; Mrazek, C.; Haschke-Becher, E.; Trinka, E.; Wipfler, P.; et al. Long-term immunological consequences of anti-CD20 therapies on humoral responses to COVID-19 vaccines in multiple sclerosis: An observational study. Ther. Adv. Neurol. Disord. 2022, 15, 17562864221092092. [Google Scholar] [CrossRef] [PubMed]
- Moser, T.; Otto, F.; O’Sullivan, C.; Hitzl, W.; Pilz, G.; Harrer, A.; Trinka, E.; Wipfler, P. Recall response to COVID-19 antigen is preserved in people with multiple sclerosis on anti-CD20 medications—A pilot study. Mult. Scler. Relat. Disord. 2022, 59, 103560. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Bar-Or, A.; Arnold, D.; Comi, G.; Hartung, H.-P.; Hauser, S.L.; Lublin, F.; Selmaj, K.; Traboulsee, A.; Chin, P.; et al. P 2 Effect of ocrelizumab on humoral immunity markers in the phase iii, double-blind, double-dummy, IFNβ-1a–controlled OPERA I and OPERA II studies. Clin. Neurophysiol. 2017, 128, e326–e327. [Google Scholar] [CrossRef]
- Moser, T.; O’Sullivan, C.; Puttinger, C.; Feige, J.; Pilz, G.; Haschke-Becher, E.; Cadamuro, J.; Oberkofler, H.; Hitzl, W.; Harrer, A.; et al. Pre-Existing Humoral Immunological Memory Is Retained in Patients with Multiple Sclerosis Receiving Cladribine Therapy. Biomedicines 2021, 9, 1584. [Google Scholar] [CrossRef]
- Moser, T.; Schwenker, K.; Seiberl, M.; Feige, J.; Akgun, K.; Haschke-Becher, E.; Ziemssen, T.; Sellner, J. Long-term peripheral immune cell profiling reveals further targets of oral cladribine in MS. Ann. Clin. Transl. Neurol. 2020, 7, 2199–2212. [Google Scholar] [CrossRef]
- Baker, D.; MacDougall, A.; Kang, A.S.; Schmierer, K.; Giovannoni, G.; Dobson, R. CD19 B cell repopulation after ocrelizumab, alemtuzumab and cladribine: Implications for SARS-CoV-2 vaccinations in multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 57, 103448. [Google Scholar] [CrossRef]
- Achiron, A.; Mandel, M.; Dreyer-Alster, S.; Harari, G.; Magalashvili, D.; Sonis, P.; Dolev, M.; Menascu, S.; Flechter, S.; Falb, R.; et al. Humoral immune response to COVID-19 mRNA vaccine in patients with multiple sclerosis treated with high-efficacy disease-modifying therapies. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211012835. [Google Scholar] [CrossRef]
- Kornek, B.; Leutmezer, F.; Rommer, P.S.; Koblischke, M.; Schneider, L.; Haslacher, H.; Thalhammer, R.; Zimprich, F.; Zulehner, G.; Bsteh, G.; et al. B Cell Depletion and SARS-CoV-2 Vaccine Responses in Neuroimmunologic Patients. Ann. Neurol. 2022, 91, 342–352. [Google Scholar] [CrossRef]
- Tolf, A.; Wiberg, A.; Muller, M.; Nazir, F.H.; Pavlovic, I.; Lauren, I.; Mangsbo, S.; Burman, J. Factors Associated With Serological Response to SARS-CoV-2 Vaccination in Patients With Multiple Sclerosis Treated With Rituximab. JAMA Netw. Open 2022, 5, e2211497. [Google Scholar] [CrossRef]
- Maarouf, A.; Rico, A.; Boutiere, C.; Perriguey, M.; Demortiere, S.; Pelletier, J.; Audoin, B.; Under the aegis of OFSEP. Extending rituximab dosing intervals in patients with MS during the COVID-19 pandemic and beyond? Neurol. Neuroimmunol. Neuroinflamm 2020, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- Rolfes, L.; Pawlitzki, M.; Pfeuffer, S.; Nelke, C.; Lux, A.; Pul, R.; Kleinschnitz, C.; Kleinschnitz, K.; Rogall, R.; Pape, K.; et al. Ocrelizumab Extended Interval Dosing in Multiple Sclerosis in Times of COVID-19. Neurol. Neuroimmunol. Neuroinflamm 2021, 8, e1035. [Google Scholar] [CrossRef] [PubMed]
- Ibarrondo, F.J.; Hofmann, C.; Fulcher, J.A.; Goodman-Meza, D.; Mu, W.; Hausner, M.A.; Ali, A.; Balamurugan, A.; Taus, E.; Elliott, J.; et al. Primary, Recall, and Decay Kinetics of SARS-CoV-2 Vaccine Antibody Responses. ACS Nano 2021, 15, 11180–11191. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Responders (>7 BAU/mL) | Non-Responders (<7 BAU/mL) | Recall Cohort | p-Values |
|---|---|---|---|---|
| n (%) | 34 (43) | 37 (46) | 9 (11) | n.s. |
| Diagnosis, n (%) | n.s. | |||
| ● RRMS | 7 (21) | 7 (19) | 2 (22) | |
| ● PPMS | 6 (18) | 15 (41) | 5 (56) | |
| ● SPMS | 20 (59) | 11 (30) | 1 (11) | |
| ● Others | 1 (3) | 4 (11) | 1 (11) | |
| Mean age (years, ±SD) | 52 ± 12 | 46 ± 11 | 45 ± 12 | 0.04 |
| Female, n (%) | 16 (47) | 24 (65) | 3 (33) | n.s. |
| COVID-19 infection, n (%) | 5 (15) | 5 (14) | 2 (22) | n.s. |
| Anti-CD20 agent, n (%) | n.s. | |||
| ● ocrelizumab | 12 (35) | 24 (65) | 6 (67) | |
| ● rituximab | 22 (65) | 13 (35) | 3 (33) | |
| Mean intervals between last infusion and B-cell count (months, ±SD) | 17 ± 11.6 | 7 ± 4.3 | 6 ± 3.1 | 0.01 |
| Mean intervals between last SARS-CoV-2 contact and antibody assessment (days, ±SD) | 91 ± 74.5 | 92 ± 65.2 | 67 ± 63.9 | n.s. |
| B cells/µL at the time of antibody assessment (mean, ±SD) | 101.8 (±105.4) | 17.3 (±47.4) | 9.1 (±20.2) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feige, J.; Berek, K.; Seiberl, M.; Hilpold, P.; Hitzl, W.; Di Pauli, F.; Hegen, H.; Deisenhammer, F.; Trinka, E.; Harrer, A.; et al. Humoral Response to SARS-CoV-2 Antigen in Patients Treated with Monoclonal Anti-CD20 Antibodies: It Is Not All about B Cell Recovery. Neurol. Int. 2022, 14, 943-951. https://doi.org/10.3390/neurolint14040075
Feige J, Berek K, Seiberl M, Hilpold P, Hitzl W, Di Pauli F, Hegen H, Deisenhammer F, Trinka E, Harrer A, et al. Humoral Response to SARS-CoV-2 Antigen in Patients Treated with Monoclonal Anti-CD20 Antibodies: It Is Not All about B Cell Recovery. Neurology International. 2022; 14(4):943-951. https://doi.org/10.3390/neurolint14040075
Chicago/Turabian StyleFeige, Julia, Klaus Berek, Michael Seiberl, Patrick Hilpold, Wolfgang Hitzl, Franziska Di Pauli, Harald Hegen, Florian Deisenhammer, Eugen Trinka, Andrea Harrer, and et al. 2022. "Humoral Response to SARS-CoV-2 Antigen in Patients Treated with Monoclonal Anti-CD20 Antibodies: It Is Not All about B Cell Recovery" Neurology International 14, no. 4: 943-951. https://doi.org/10.3390/neurolint14040075
APA StyleFeige, J., Berek, K., Seiberl, M., Hilpold, P., Hitzl, W., Di Pauli, F., Hegen, H., Deisenhammer, F., Trinka, E., Harrer, A., Wipfler, P., & Moser, T. (2022). Humoral Response to SARS-CoV-2 Antigen in Patients Treated with Monoclonal Anti-CD20 Antibodies: It Is Not All about B Cell Recovery. Neurology International, 14(4), 943-951. https://doi.org/10.3390/neurolint14040075