
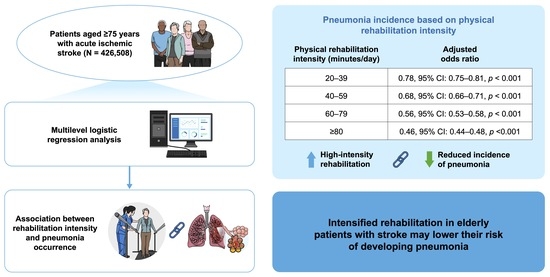
Physical Rehabilitation and Post-Stroke Pneumonia: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Study Participants
2.3. Assessment of Physical Rehabilitation Duration
2.4. Assessment of Pneumonia
2.5. Assessment of Covariates
2.6. Statistical Analysis
2.7. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kishore, A.K.; Vail, A.; Chamorro, A.; Garau, J.; Hopkins, S.J.; Di Napoli, M.; Kalra, L.; Langhorne, P.; Montaner, J.; Roffe, C.; et al. How is pneumonia diagnosed in clinical stroke research? A systematic review and meta-analysis. Stroke 2015, 46, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.; Mhina, C.; Philip, K.; Patel, S.D.; Aneni, E.; Osondu, C.; Lamikanra, O.; Akano, E.O.; Anikpezie, N.; Albright, K.C.; et al. Age- and Sex-Specific Trends in Medical Complications After Acute Ischemic Stroke in the United States. Neurology 2023, 100, e1282–e1295. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, J.C.; van de Beek, D.; Lyden, P.; Brady, M.C.; Bath, P.M.; van der Worp, H.B. Temporal Profile of Pneumonia After Stroke. Stroke 2022, 53, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, O.; Kapral, M.; Hall, R.; Asllani, E.; Selchen, D.; Saposnik, G.; Canadian Stroke Network; Stroke Outcome Research Canada (SORCan) Working Group. Risk factors, inpatient care, and outcomes of pneumonia after ischemic stroke. Neurology 2011, 77, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Li, F.; Tian, X.; Wang, W.; Jia, M.; Wang, X.; Liu, G. Risk factors for lung infection in stroke patients: A meta-analysis of observational studies. Expert Rev. Anti Infect. Ther. 2015, 13, 1289–1298. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Choo, Y.J.; Seo, K.C.; Yang, S. The Relationship Between Dysphagia and Pneumonia in Acute Stroke Patients: A Systematic Review and Meta-Analysis. Front. Neurol. 2022, 13, 834240. [Google Scholar] [CrossRef] [PubMed]
- Banda, K.J.; Chu, H.; Kang, X.L.; Liu, D.; Pien, L.; Jen, H.; Hsiao, S.S.; Chou, K. Prevalence of dysphagia and risk of pneumonia and mortality in acute stroke patients: A meta-analysis. BMC Geriatr. 2022, 22, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Lin, Y.; Chang, Y.; Chen, C.; Chiang, H.; Huang, L.; Yang, Y.; Hung, C. The Mortality and the Risk of Aspiration Pneumonia Related with Dysphagia in Stroke Patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1381–1387. [Google Scholar] [CrossRef]
- Brogan, E.; Langdon, C.; Brookes, K.; Budgeon, C.; Blacker, D. Can’t swallow, can’t transfer, can’t toilet: Factors predicting infections in the first week post stroke. J. Clin. Neurosci. 2015, 22, 92–97. [Google Scholar] [CrossRef]
- Teh, W.H.; Smith, C.J.; Barlas, R.S.; Wood, A.D.; Bettencourt-Silva, J.H.; Clark, A.B.; Metcalf, A.K.; Bowles, K.M.; Potter, J.F.; Myint, P.K. Impact of stroke-associated pneumonia on mortality, length of hospitalization, and functional outcome. Acta Neurol. Scand. 2018, 138, 293–300. [Google Scholar] [CrossRef]
- Barlas, R.S.; Clark, A.B.; Bettencourt-Silva, J.H.; Sawanyawisuth, K.; Kongbunkiat, K.; Kasemsap, N.; Tiamkao, S.; Myint, P.K. Pneumonia and Risk of Serious Adverse Outcomes in Hospitalized Strokes in Thailand. J. Stroke Cerebrovasc. Dis. 2019, 28, 1448–1454. [Google Scholar] [CrossRef]
- Katzan, I.L.; Dawson, N.V.; Thomas, C.L.; Votruba, M.E.; Cebul, R.D. The cost of pneumonia after acute stroke. Neurology 2007, 68, 1938–1943. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Collier, J.M.; Bate, P.J.; Thuy, M.N.; Bernhardt, J. Very early versus delayed mobilisation after stroke. Cochrane Database Syst. Rev. 2018, 10, CD006187 (1-81). [Google Scholar] [CrossRef] [PubMed]
- AVERT Trial Collaboration Group. Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): A randomised controlled trial. Lancet 2015, 386, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, S.; Ogasawara, K.; Kuroda, S.; Itabashi, R.; Toyoda, K.; Itoh, Y.; Iguchi, Y.; Shiokawa, Y.; Takagi, Y.; Ohtsuki, T.; et al. Japan Stroke Society Guideline 2021 for the Treatment of Stroke. Int. J. Stroke 2022, 17, 1039–1049. [Google Scholar] [CrossRef]
- Ingeman, A.; Andersen, G.; Hundborg, H.H.; Svendsen, M.L.; Johnsen, S.P. Processes of care and medical complications in patients with stroke. Stroke 2011, 42, 167–172. [Google Scholar] [CrossRef]
- Fujita, A.; Iwata, M.; Hagii, J.; Metoki, N.; Shiroto, H.; Tsuda, E. The effects of combined early oral health care and early mobilisation on the incidence of stroke-associated pneumonia. J. Stroke Cerebrovasc. Dis. 2023, 32, 106893. [Google Scholar] [CrossRef]
- Bath, P.M.; Lee, H.S.; Everton, L.F. Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst. Rev. 2018, 10, CD000323 (1-142). [Google Scholar] [CrossRef]
- Yagi, M.; Yasunaga, H.; Matsui, H.; Morita, K.; Fushimi, K.; Fujimoto, M.; Koyama, T.; Fujitani, J. Impact of Rehabilitation on Outcomes in Patients With Ischemic Stroke: A Nationwide Retrospective Cohort Study in Japan. Stroke 2017, 48, 740–746. [Google Scholar] [CrossRef]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and Profile of Diagnosis Procedure Combination (DPC): Development of a Real Data Collection System for Acute Inpatient Care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef]
- Yasunaga, H. Real World Data in Japan: Chapter Ⅱ The Diagnosis Procedure Combination Database. Ann. Clin. Epidemiol. 2019, 1, 76–79. [Google Scholar] [CrossRef]
- Yamaura, R.; Kaneko, T.; Ishikawa, K.B.; Ikeda, S.; Fushimi, K.; Yamazaki, T. Factors Associated With Time to Achieve Physical Functional Recovery in Patients With Severe Stoke After Inpatient Rehabilitation: A Retrospective Nationwide Cohort Study in Japan. Arch. Rehabil. Res. Clin. Transl. 2022, 4, 100229. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Yasunaga, H.; Inokuchi, R.; Horiguchi, H.; Fushimi, K.; Matsubara, T.; Nakajima, S.; Yahagi, N. Effects of edaravone on early outcomes in acute ischemic stroke patients treated with recombinant tissue plasminogen activator. J. Neurol. Sci. 2014, 345, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Todo, T.; Usui, M.; Takakura, K. Treatment of severe intraventricular hemorrhage by intraventricular infusion of urokinase. J. Neurosurg. 1991, 74, 81–86. [Google Scholar] [CrossRef]
- Ono, Y.; Ono, S.; Yasunaga, H.; Matsui, H.; Fushimi, K.; Tanaka, Y. Clinical characteristics and outcomes of myxedema coma: Analysis of a national inpatient database in Japan. J. Epidemiol. 2017, 27, 117–122. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Nakajima, M.; Okada, Y.; Sonoo, T.; Goto, T. Development and Validation of a Novel Method for Converting the Japan Coma Scale to Glasgow Coma Scale. J. Epidemiol. 2023, 33, 531–535. [Google Scholar] [CrossRef]
- Williams, P.T. Dose-response relationship between exercise and respiratory disease mortality. Med. Sci. Sports Exerc. 2014, 46, 711–717. [Google Scholar] [CrossRef]
- Matsugaki, R.; Muramatsu, K.; Fushimi, K.; Matsuda, S. Dementia and acute care of ischemic stroke in Japan: A retrospective observational study using the Japanese Diagnosis Procedure Combination database. Geriatr. Gerontol. Int. 2023, 23, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Cuesy, P.G.; Sotomayor, P.L.; Piña, J.O.T. Reduction in the Incidence of Poststroke Nosocomial Pneumonia by Using the “Turn-mob” Program. J. Stroke Cerebrovasc. Dis. 2010, 19, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Al-Khaled, M.; Matthis, C.; Binder, A.; Mudter, J.; Schattschneider, J.; Pulkowski, U.; Strohmaier, T.; Niehoff, T.; Zybur, R.; Eggers, J.; et al. Dysphagia in Patients with Acute Ischemic Stroke: Early Dysphagia Screening May Reduce Stroke-Related Pneumonia and Improve Stroke Outcomes. Cerebrovasc. Dis. 2016, 42, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Boaden, E.; Burnell, J.; Hives, L.; Dey, P.; Clegg, A.; Lyons, M.W.; Lightbody, C.E.; Hurley, M.A.; Roddam, H.; McInnes, E.; et al. Screening for aspiration risk associated with dysphagia in acute stroke. Cochrane Database Syst. Rev. 2021, 10, CD012679. [Google Scholar] [CrossRef] [PubMed]
- Gosselink, R.; Bott, J.; Johnson, M.; Dean, E.; Nava, S.; Norrenberg, M.; Schonhofer, B.; Stiller, K.; van de Leur, H.; Vincent, J.L. Physiotherapy for adult patients with critical illness: Recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Med. 2008, 34, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Stanwell, P.; Bivard, A.; Spratt, N.; Walker, R.; Kitsos, G.H.; Parsons, M.W.; Evans, M.; Jordan, L.; Nilsson, M.; et al. The influence of initial stroke severity on mortality, overall functional outcome and in-hospital placement at 90 days following acute ischemic stroke: A tertiary hospital stroke register study. Neurol. India 2017, 65, 1252–1259. [Google Scholar] [CrossRef] [PubMed]
- Romano, J.G.; Gardener, H.; Campo-Bustillo, I.; Khan, Y.; Tai, S.; Riley, N.; Smith, E.E.; Sacco, R.L.; Khatri, P.; Alger, H.M.; et al. MaRISS Investigators* Predictors of Outcomes in Patients With Mild Ischemic Stroke Symptoms: MaRISS. Stroke 2021, 52, 1995–2004. [Google Scholar] [CrossRef]
- Henke, C.; Foerch, C.; Lapa, S. Early Screening Parameters for Dysphagia in Acute Ischemic Stroke. Cerebrovasc. Dis. 2017, 44, 285–290. [Google Scholar] [CrossRef]
- Yamana, H.; Moriwaki, M.; Horiguchi, H.; Kodan, M.; Fushimi, K.; Yasunaga, H. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J. Epidemiol. 2017, 27, 476–482. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Duration of Physical Rehabilitation | ||||||
|---|---|---|---|---|---|---|
| Total (n = 426,508) | <20 min/Day (n = 43,505) | 20–39 min/Day (n = 125,126) | 40–59 min/Day (n = 123,718) | 60–79 min/Day (n = 73,172) | 80 min/Day (n = 60,987) | |
| Age, median (IQR) | 83.0 (79.0, 88.0) | 84.0 (79.0, 88.0) | 83.0 (79.0, 88.0) | 83.0 (79.0, 88.0) | 83.0 (79.0, 88.0) | 83.0 (79.0, 87.0) |
| Sex | ||||||
| men | 206,564 (48.4%) | 20,208 (46.4%) | 60,618 (48.4%) | 60,210 (48.7%) | 35,860 (49.0%) | 29,668 (48.6%) |
| women | 219,944 (51.6%) | 23,297 (53.6%) | 64,508 (51.6%) | 63,508 (51.3%) | 37,312 (51.0%) | 31,319 (51.4%) |
| Subtype of ischemic stroke | ||||||
| Arterial thrombosis | 160,613 (37.7%) | 14,021 (32.2%) | 45,424 (36.3%) | 47,311 (38.2%) | 29,146 (39.8%) | 24,711 (40.5%) |
| Arterial embolism | 134,911 (31.6%) | 15,827 (36.4%) | 41,543 (33.2%) | 38,997 (31.5%) | 21,323 (29.1%) | 17,221 (28.2%) |
| Others | 130,984 (30.7%) | 13,657 (31.4%) | 38,159 (30.5%) | 37,410 (30.2%) | 22,703 (31.0%) | 19,055 (31.2%) |
| Charlson comorbidity index | ||||||
| 0 | 142,996 (33.5%) | 14,669 (33.7%) | 42,495 (34.0%) | 41,323 (33.4%) | 24,559 (33.6%) | 19,950 (32.7%) |
| 1 | 134,435 (31.5%) | 13,761 (31.6%) | 39,641 (31.7%) | 39,556 (32.0%) | 23,128 (31.6%) | 18,349 (30.1%) |
| 2 | 85,057 (19.9%) | 8519 (19.6%) | 24,682 (19.7%) | 24,616 (19.9%) | 14,558 (19.9%) | 12,682 (20.8%) |
| 3≤ | 64,020 (15.0%) | 6556 (15.1%) | 18,308 (14.6%) | 18,223 (14.7%) | 10,927 (14.9%) | 10,006 (16.4%) |
| Japan Coma Scale score at admission | ||||||
| 0 | 157,335 (36.9%) | 14,341 (33.0%) | 46,992 (37.6%) | 45,397 (36.7%) | 27,662 (37.8%) | 22,943 (37.6%) |
| 1–3 | 200,509 (47.0%) | 17,503 (40.2%) | 54,944 (43.9%) | 59,339 (48.0%) | 36,803 (50.3%) | 31,920 (52.3%) |
| 10–30 | 48,999 (11.5%) | 6816 (15.7%) | 15,832 (12.7%) | 14,471 (11.7%) | 6894 (9.4%) | 4986 (8.2%) |
| 100–300 | 19,665 (4.6%) | 4845 (11.1%) | 7358 (5.9%) | 4511 (3.6%) | 1813 (2.5%) | 1138 (1.9%) |
| Modified Rankin Scale score before admission | ||||||
| 0 | 163,342 (38.3%) | 15,442 (35.5%) | 47,664 (38.1%) | 47,430 (38.3%) | 28,490 (38.9%) | 24,316 (39.9%) |
| 1 | 75,758 (17.8%) | 7490 (17.2%) | 22,369 (17.9%) | 22,273 (18.0%) | 13,120 (17.9%) | 10,506 (17.2%) |
| 2 | 57,076 (13.4%) | 5563 (12.8%) | 16,821 (13.4%) | 17,057 (13.8%) | 9920 (13.6%) | 7715 (12.7%) |
| 3 | 51,049 (12.0%) | 4921 (11.3%) | 14,808 (11.8%) | 14,976 (12.1%) | 8896 (12.2%) | 7448 (12.2%) |
| 4 | 55,459 (13.0%) | 6016 (13.8%) | 15,998 (12.8%) | 15,764 (12.7%) | 9391 (12.8%) | 8290 (13.6%) |
| 5 | 23,709 (5.6%) | 4046 (9.3%) | 7430 (5.9%) | 6190 (5.0%) | 3343 (4.6%) | 2700 (4.4%) |
| Acute care | ||||||
| Intravenous thrombolysis | 29,556 (6.9%) | 2502 (5.8%) | 8840 (7.1%) | 9393 (7.6%) | 5118 (7.0%) | 3703 (6.1%) |
| Endovascular thrombectomy | 16,480 (3.9%) | 1582 (3.6%) | 5144 (4.1%) | 5226 (4.2%) | 2622 (3.6%) | 1906 (3.1%) |
| Mechanical ventilation | 3227 (0.8%) | 1119 (2.6%) | 1280 (1.0%) | 518 (0.4%) | 199 (0.3%) | 111 (0.2%) |
| Tube feeding | 29,162 (6.8%) | 3175 (7.3%) | 9763 (7.8%) | 8766 (7.1%) | 4205 (5.7%) | 3253 (5.3%) |
| Fiscal year | ||||||
| 2014 | 64,972 (15.2%) | 9720 (22.3%) | 20,345 (16.3%) | 17,233 (13.9%) | 9511 (13.0%) | 8163 (13.4%) |
| 2015 | 70,889 (16.6%) | 8016 (18.4%) | 21,715 (17.4%) | 19,623 (15.9%) | 11,622 (15.9%) | 9913 (16.3%) |
| 2016 | 73,779 (17.3%) | 7468 (17.2%) | 21,667 (17.3%) | 21,136 (17.1%) | 12,545 (17.1%) | 10,963 (18.0%) |
| 2017 | 73,113 (17.1%) | 6287 (14.5%) | 21,232 (17.0%) | 21,868 (17.7%) | 13,051 (17.8%) | 10,675 (17.5%) |
| 2018 | 73,411 (17.2%) | 6501 (14.9%) | 20,450 (16.3%) | 22,214 (18.0%) | 13,324 (18.2%) | 10,922 (17.9%) |
| 2019 | 70,344 (16.5%) | 5513 (12.7%) | 19,717 (15.8%) | 21,644 (17.5%) | 13,119 (17.9%) | 10,351 (17.0%) |
| Hospital volume (patients/year) | ||||||
| −73 | 142,787 (33.5%) | 19,710 (45.3%) | 43,445 (34.7%) | 40,364 (32.6%) | 22,229 (30.4%) | 17,039 (27.9%) |
| 74–133 | 142,124 (33.3%) | 13,599 (31.3%) | 44,344 (35.4%) | 43,642 (35.3%) | 23,793 (32.5%) | 16,746 (27.5%) |
| 134– | 141,597 (33.2%) | 10,196 (23.4%) | 37,337 (29.8%) | 39,712 (32.1%) | 27,150 (37.1%) | 27,202 (44.6%) |
| Intensity of Physical Rehabilitation | ||||||
|---|---|---|---|---|---|---|
| <20 min/Day (n = 43,505) | 20–39 min/Day (n = 125,126) | 40–59 min/Day (n = 123,718) | 60–79 min/Day (n = 73,172) | 80 min/Day (n = 60,987) | p-Value | |
| Pneumonia (ICD-10: J12-J18, J69) | 5849 (13.4%) | 12,678 (10.1%) | 10,972 (8.9%) | 5384 (7.4%) | 3917 (6.4%) | <0.001 |
| Pneumonia (ICD-10: J12-J18) | 2006 (4.6%) | 4040 (3.2%) | 3473 (2.8%) | 1766 (2.4%) | 1539 (2.5%) | <0.001 |
| Aspiration pneumonia (ICD-10: J69) | 3843 (8.8%) | 8638 (6.9%) | 7499 (6.1%) | 3618 (4.9%) | 2378 (3.9%) | <0.001 |
| Age-Sex Adjusted | Multivariate Adjusted * | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | p-Value for Trend | OR | 95% CI | p-Value | p-Value for Trend | |||
| Duration of physical rehabilitation | ||||||||||
| <20 min/day | Reference | Reference | ||||||||
| 20–39 min/day | 0.69 | 0.67 | 0.72 | <0.001 | <0.001 | 0.78 | 0.75 | 0.81 | <0.001 | <0.001 |
| 40–59 min/day | 0.56 | 0.54 | 0.58 | <0.001 | 0.68 | 0.66 | 0.71 | <0.001 | ||
| 60–79 min/day | 0.42 | 0.40 | 0.44 | <0.001 | 0.56 | 0.53 | 0.58 | <0.001 | ||
| 80 min/day | 0.33 | 0.31 | 0.35 | <0.001 | 0.46 | 0.44 | 0.48 | <0.001 | ||
| Age-Sex Adjusted | Multivariate Adjusted * | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | p-Value for Trend | OR | 95% CI | p-Value | p-Value for Trend | |||
| Non-aspiration pneumonia (n = 12,824) | ||||||||||
| Duration of physical rehabilitation | ||||||||||
| <20 min/day | Reference | Reference | ||||||||
| 20–39 min/day | 0.70 | 0.66 | 0.74 | <0.001 | <0.001 | 0.79 | 0.74 | 0.83 | <0.001 | <0.001 |
| 40–59 min/day | 0.56 | 0.53 | 0.59 | <0.001 | 0.68 | 0.64 | 0.72 | <0.001 | ||
| 60–79 min/day | 0.41 | 0.38 | 0.44 | <0.001 | 0.54 | 0.50 | 0.58 | <0.001 | ||
| 80 min/day | 0.35 | 0.32 | 0.38 | <0.001 | 0.47 | 0.43 | 0.51 | <0.001 | ||
| Aspiration pneumonia (n = 25,976) | ||||||||||
| Duration of physical rehabilitation | ||||||||||
| <20 min/day | Reference | Reference | ||||||||
| 20–39 min/day | 0.71 | 0.68 | 0.74 | <0.001 | <0.001 | 0.80 | 0.77 | 0.84 | <0.001 | <0.001 |
| 40–59 min/day | 0.59 | 0.57 | 0.62 | <0.001 | 0.72 | 0.68 | 0.75 | <0.001 | ||
| 60–79 min/day | 0.46 | 0.43 | 0.48 | <0.001 | 0.60 | 0.57 | 0.64 | <0.001 | ||
| 80 min/day | 0.35 | 0.33 | 0.37 | <0.001 | 0.49 | 0.46 | 0.52 | <0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, T.; Matsugaki, R.; Matsuda, S. Physical Rehabilitation and Post-Stroke Pneumonia: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database. Neurol. Int. 2023, 15, 1459-1468. https://doi.org/10.3390/neurolint15040094
Nishimura T, Matsugaki R, Matsuda S. Physical Rehabilitation and Post-Stroke Pneumonia: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database. Neurology International. 2023; 15(4):1459-1468. https://doi.org/10.3390/neurolint15040094
Chicago/Turabian StyleNishimura, Takehiro, Ryutaro Matsugaki, and Shinya Matsuda. 2023. "Physical Rehabilitation and Post-Stroke Pneumonia: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database" Neurology International 15, no. 4: 1459-1468. https://doi.org/10.3390/neurolint15040094
APA StyleNishimura, T., Matsugaki, R., & Matsuda, S. (2023). Physical Rehabilitation and Post-Stroke Pneumonia: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database. Neurology International, 15(4), 1459-1468. https://doi.org/10.3390/neurolint15040094