1. Introduction
With the introduction of antiretroviral therapy (ART) in 1996, HIV-associated morbidity and mortality have significantly decreased. Today, the life expectancy of people living with HIV (PLWH) is close to that of the general population provided that they receive timely diagnosis and start treatment when their CD4 counts are ≥350 cells/μL [
1]. However, despite the considerable advances achieved in the field, PLWH are often diagnosed at a late disease stage, defined as having a CD4
+ T-cell count less than 350 cells/μL or presenting with an AIDS-defining event, regardless of the CD4
+ T-cell count [
2,
3]. Late HIV presentation is a persistent issue in the global fight against HIV because it is associated with increased mortality and morbidity [
4,
5,
6], increased medical care costs [
7,
8,
9,
10] and increased sexual and vertical transmission due to late ART initiation [
6,
10,
11]. Early initiation of ART, especially when the CD4
+ T-cell count is greater than 350/mm
3, offers many benefits, including improved immunological recovery and subsequent reductions in both severe AIDS-related and severe non-AIDS-related events, as well as limited establishment of HIV reservoirs [
12,
13]. Therefore, it is critical to identify factors associated with late presentation for HIV care to improve the effectiveness of HIV testing strategies, with a focus on susceptible and possibly neglected subgroups.
Nonetheless, it is important to assess each region’s specific population and epidemiological context to determine the most appropriate response against HIV. In a previously published study, we analysed the characteristics of patients who presented for care at our centre from 2006 to 2017. Forty-four percent of the patients were late presenters [
14]. Here, we aimed to determine the proportion and predictors of late presentation (LP) and late presentation with advanced HIV disease (LP-AD) in recent years.
2. Materials and Methods
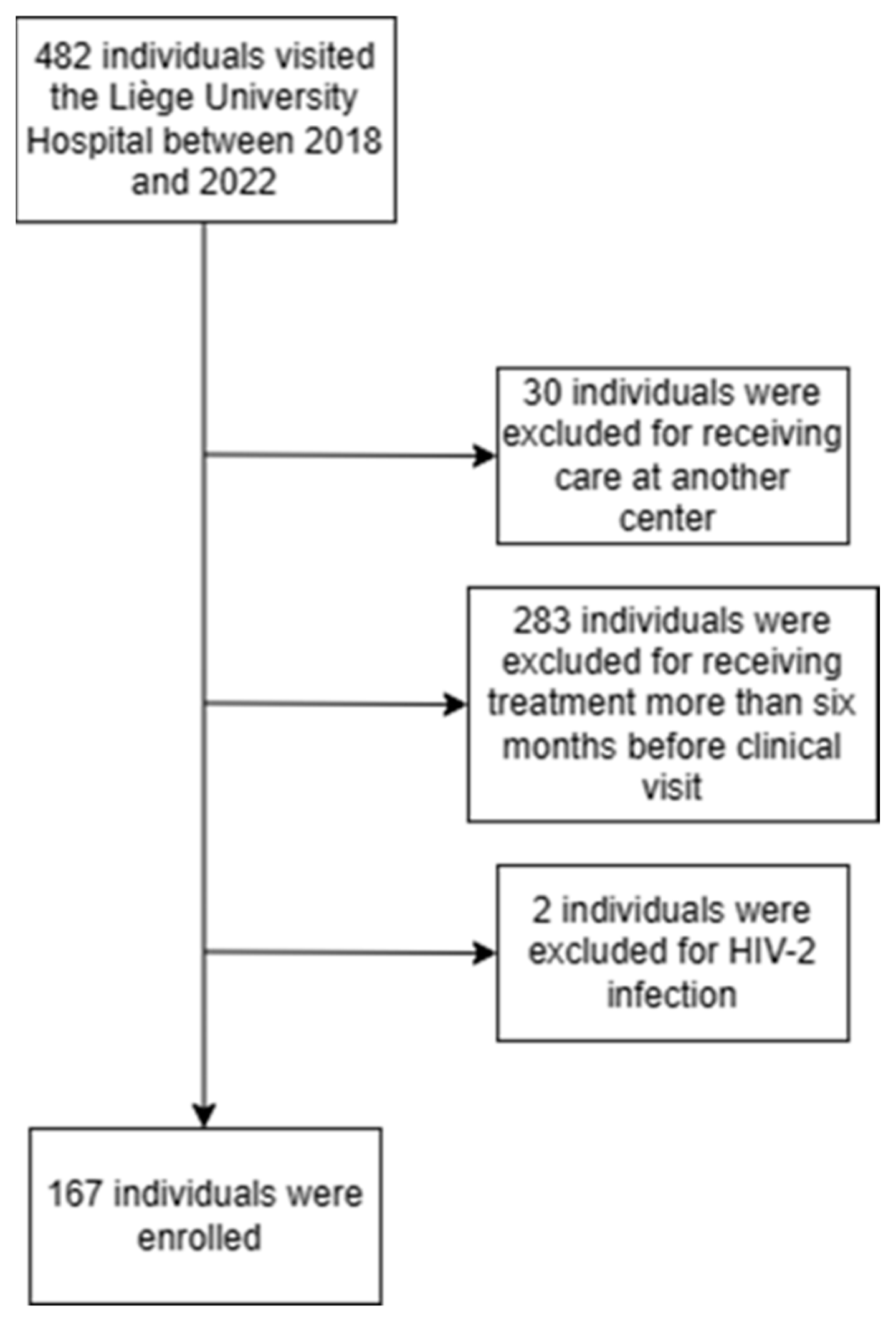
In this retrospective cohort study, we included HIV-1-infected individuals aged at least 16 years who presented for clinical care at Liège University Hospital (Belgium) for the first time between 1 January 2018 and 31 July 2022. Patients who had already received care for HIV infection at another clinical centre as well as patients who were treated for more than six months before the first clinic visit were excluded from the study.
According to a consensus definition of late presenters, “the term ‘presentation for care’ means attendance at a health care facility that is able to monitor progression of HIV infection and initiate appropriate medical care, including ART, as appropriate” [
15]. Consequently, people were also included if they had already been diagnosed but had not received care for their infection.
Patients were classified according to their CD4
+ T-cell count at ART initiation and history of AIDS-defining events within the six months following the first visit [
15]. Late HIV presenters (LPs) were defined as individuals with a CD4
+ T-cell count < 350 cells/mm
3 at presentation for care or who experienced an AIDS-defining event in the six months following the first visit. LPs were further stratified as late presenters with advanced HIV disease (LPs-AD) if the CD4
+ T-cell count was <200 cells/mm
3 at presentation for care or if an AIDS-defining event occurred (regardless of the CD4
+ T-cell count) in the six months following their first visit. Seroconverters (individuals with an HIV-negative test or a clinical history of primary infection over the past 12 months) with a CD4
+ T-cell count <350 cells/mm
3 were classified as non-LPs. By definition, such people were diagnosed soon after HIV infection and would not have been reached by interventions that promoted earlier targeted screening. Patients infected with HIV-2 were excluded from the analyses because the kinetics of the decrease in the CD4
+ T-cell count differed in these patients.
We collected the baseline characteristics of the PLWH from the electronic medical registry. These data included demographic and clinical characteristics, including age, sex, ethnicity, country of origin, mode of acquisition, information regarding AIDS-defining illnesses and the first CD4
+ T-cell count and year of first presentation for care. Finally, we also recorded the screening context, categorised as voluntary screening, medical condition screening, refugee (defined as a person fleeing armed conflict or persecution and asking for or benefiting from assistance by the state, the Red Cross or other organisations) screening, incidental screening (for instance, before a blood donation), pregnancy screening, screening due to having an HIV+ partner or other/unknown reasons. These variables were chosen because they are commonly studied in the literature [
14,
16,
17,
18], which allowed for comparisons with past studies and especially with our previous study [
14].
Statistical Analysis
The normality of the distribution of each quantitative variable was investigated using means and medians, Shapiro–Wilk tests, histograms, quantile–quantile plots (Q–Q plots) and box plots. As the quantitative variables did not have a normal distribution, they are summarised as medians, interquartile ranges (IQRs) and extreme values. Categorical variables are summarised with frequency tables. Development over time of late presentation (LP and LP-AD) as well as the impact of individuals’ characteristics on late presentation were analysed using binary logistic regression models. Univariate logistic models were constructed, and variables with p values lower than 0.10 were selected for multivariable logistic models. Collinearity between origin and ethnicity led us to include only origin in the multivariate models. For univariate models, adjusted p values (Holm–Bonferroni method) are also presented. To identify potential factors associated with late presentation, participants were further divided into 3 subgroups according to their CD4+ T-cell count and AIDS-defining event status.
Analyses were carried out on the maximum amount of data available, and no missing values were replaced. The results were considered significant at the 10% alpha level (p < 0.10). Data analysis was performed using SAS (version 9.4 (SAS Institute Inc., Cary, NC, USA) for Windows) and R (version 4.2.1 (The R Foundation for Statistical Computing, Vienna, Austria) for Windows).
Approval for the study protocol was obtained from the local ethics review committee (Comité d’Ethique Hospitalo-Facultaire Universitaire de Liège, reference number 2023-39). Individual consent was waived due to the retrospective nature of the study and the anonymisation of the data.
4. Discussion
Compared to our previous study [
14], many changes were observed between the time periods 2006–2017 and 2018–2022. First, the population was older (median age of 34.0 years (IQR 27.0–42.0) vs. 37.0 years (IQR 29.0–45.5)) in 2018–2022. Although heterosexual transmission still remained the most common mode of acquisition, it decreased from 61.0% in 2006–2017 to 42.5% in 2018–2022. In contrast to the 2006–2017 period, although Belgian MSM and heterosexual women from SSA remained the most represented groups, they did not account for the majority of individuals in the cohort. This means that other population profiles are becoming more prevalent, resulting in a diversified epidemic, which is corroborated by the literature [
19].
We found that older patients and patients from sub-Saharan Africa were at risk of late presentation with advanced HIV disease. This could be explained by patients’ fear of the perceived consequences of a positive test result, notably the fear of stigma and discrimination [
20,
21,
22]. Past adverse experiences such as loss of acquaintances during the early days of the HIV epidemic may also explain late testing and late presentation, especially among older patients [
22].
Our results differ from the LP risk factors reported in our previous study, which highlighted age, male sex, non-Belgian origin and heterosexual transmission as risk factors for late presentation and age, non-Belgian origin, heterosexual transmission and testing for medical conditions as risk factors for late presentation with advanced HIV disease [
14]. The discrepancies between the two studies can be explained by the small sample size of the present study, which included 167 individuals compared to the 604 individuals included in the previous study. This lack of statistical power would also explain the wide confidence intervals observed for some variables, such as age (
Table 4 and
Table 5). The large number of individuals excluded due to receiving treatment more than six months before their clinical visit can be explained by Belgium’s link to sub-Saharan Africa, notably the Democratic Republic of the Congo (past colony), which results in many migrants from this region.
Other studies performed during a similar timeframe (2017 to 2020, 2019 to 2020 and 2015 to 2020) also revealed that male and older patients are at greater risk of late HIV presentation [
23,
24,
25]. Additionally, other LP risk factors, including bisexual transmission, heterosexual transmission, being married, SSA origin, tuberculosis or hepatitis C virus coinfection, lower socioeconomic status and the fear of stigma, have been reported in various studies [
25,
26,
27,
28,
29,
30,
31,
32,
33]. The discrepancies observed among those studies highlight the importance of identifying populations at risk of late presentation and developing specific guidelines according to the region.
Notably, this study aimed to determine the proportions and predictors of LP and LP-AD between 2018 and 2022, a period marked by the COVID-19 pandemic. This pandemic may have influenced our findings, as there was a decrease in new HIV diagnoses, in the follow-up of PLWH and in comorbidity screening during the first wave of the pandemic in Belgium [
34,
35]. This could be explained by several factors, such as the restrictions on medical appointments, the closing of several screening centres and the misinterpretation of symptoms of HIV infection as symptoms of COVID-19 infection.
The possible bias and limitations of this study should be noted. First, limiting the study population to individuals presenting for care at Liège University Hospital may have influenced the results, as profiles may be limited, resulting in selection bias. A greater number of participants is needed to draw more solid conclusions about the at-risk population. Conversely, this study’s strength lies in the fact that the chosen healthcare facility includes the “AIDS reference centre of Liège”, which provides individuals and their families with multidisciplinary care and is “hidden” within the facility (“AIDS reference centre” is not written anywhere) [
36]. This may have resulted in widening the scope of individuals presenting at the facility and may have attenuated the selection bias.
Since additional risk factors for late presentation could have been missed, it would be interesting to extend this study to other testing centres in Liège to better investigate the potential impact of the real diversity of the population. It would also be interesting to complete a qualitative study among late presenters to assess the impact of the COVID-19 pandemic on late presentations.
Since most screenings were performed due to a medical problem, voluntary screening should be promoted through information campaigns. Although these information campaigns should focus on high-prevalence groups, they should also target other groups, as the variety of profiles of late presenters seems to be increasing.


 ,
, 

{kind=link}