
Lupus Nephritis, Autoantibody Production and Kidney Outcomes in Males with Childhood-Onset Systemic Lupus Erythematosus

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, L.J.; Wallace, D.J.; Ishimori, M.L.; Scofield, R.H.; Weisman, M.H. Review: Male systemic lupus erythematosus: A review of sex disparities in this disease. Lupus 2010, 19, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.; Isenberg, D. Effect of gender on clinical presentation in systemic lupus erythematosus. Rheumatology 2013, 52, 2108–2115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, K.K.; Jones, D.P.; Hastings, M.C.; Gaber, L.W.; Ault, B.H. Short-term outcomes of severe lupus nephritis in a cohort of predominantly African-American children. Pediatr. Nephrol. 2006, 21, 655–662. [Google Scholar] [CrossRef]
- Brunner, H.I.; Gladman, D.D.; Ibanez, D.; Urowitz, M.D.; Silverman, E.D. Difference in disease features between childhood-onset and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2008, 58, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.O.; von Scheven, E.; Yazdany, J.; Panopalis, P.; Trupin, L.; Julian, L.; Katz, P.; Criswell, L.A.; Yelin, E. Differences in long-term disease activity and treatment of adult patients with childhood- and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2009, 61, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Son, M.B.F.; Johnson, V.M.; Hersh, A.O.; Lo, M.S.; Costenbader, K.H. Outcomes in Hospitalized Pediatric Patients With Systemic Lupus Erythematosus. Pediatrics 2014, 133, e106–e113. [Google Scholar] [CrossRef] [Green Version]
- Hiraki, L.T.; Feldman, C.H.; Liu, J.; Alarcón, G.S.; Fischer, M.A.; Winkelmayer, W.C.; Costenbader, K.H. Prevalence, incidence, and demographics of systemic lupus erythematosus and lupus nephritis from 2000 to 2004 among children in the US medicaid beneficiary population. Arthritis Rheum. 2012, 64, 2669–2676. [Google Scholar] [CrossRef] [Green Version]
- Apenteng, T.; Kaplan, B.; Meyers, K. Renal outcomes in children with lupus and a family history of autoimmune disease. Lupus 2006, 15, 65–70. [Google Scholar] [CrossRef]
- Al-Mayouf, S.M.; Al Sonbul, A. Influence of gender and age of onset on the outcome in children with systemic lupus erythematosus. Clin. Rheumatol. 2008, 27, 1159–1162. [Google Scholar] [CrossRef]
- Miettunen, P.M.; Ortiz-Alvarez, O.; Petty, R.E.; Cimaz, R.; Malleson, P.N.; Cabral, D.A.; Ensworth, S.; Tucker, L.B. Gender and ethnic origin have no effect on longterm outcome of childhood-onset systemic lupus erythematosus. J. Rheumatol. 2004, 31, 1650–1654. [Google Scholar]
- Hari, P.; Bagga, A.; Mahajan, P.; Dinda, A. Outcome of lupus nephritis in Indian children. Lupus 2009, 18, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Thorner, P.S.; Baumal, R.; Arbus, G.S. Sex differences in childhood lupus nephritis. Am. J. Dis. Child. 1984, 138, 586–588. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.S.; Cho, H.Y.; Kim, E.J.; Kang, H.G.; Ha, I.S.; Cheong, H.I.; Kim, J.G.; Lee, H.S.; Choi, Y. Clinical outcomes of childhood lupus nephritis: A single center′s experience. Pediatr. Nephrol. 2007, 22, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, B.; Vivarelli, M.; Gianviti, A.; Benetti, E.; Peruzzi, L.; Barbano, G.; Corona, F.; Ventura, G.; Pecoraro, C.; Murer, L.; et al. Lupus nephritis in children and adolescents: Results of the Italian Collaborative Study. Nephrol. Dial. Transplant. 2013, 28, 1487–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraki, L.T.; Lu, B.; Alexander, S.R.; Shaykevich, T.; Alarcon, G.S.; Solomon, D.H.; Winkelmayer, W.C.; Costenbader, K.H. End-stage renal disease due to lupus nephritis among children in the US, 1995–2006. Arthritis Rheum. 2011, 63, 1988–1997. [Google Scholar] [CrossRef] [Green Version]
- Hahn, B.H.; McMahon, M.A.; Wilkinson, A.; Wallace, W.D.; Daikh, D.I.; Fitzgerald, J.D.; Karpouzas, G.A.; Merrill, J.T.; Wallace, D.J.; Yazdany, J.; et al. American college of rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 2012, 64, 797–808. [Google Scholar] [CrossRef] [Green Version]
- Churg, J.; Bernstein, J.; Glassock, R.J. Renal Disease: Classification and Atlas of Glomerular Diseases, 2nd ed.; Igaky-Shoin: New York, NY, USA, 1995. [Google Scholar]
- Askenazi, D.; Myones, B.; Kamdar, A.; Warren, R.; Perez, M.; De Guzman, M.; Minta, A.; Hicks, M.J.; Kale, A. Outcomes of children with proliferative lupus nephritis: The role of protocol renal biopsy. Pediatr. Nephrol. 2007, 22, 981–986. [Google Scholar] [CrossRef]
- Sorof, J.M.; Perez, M.D.; Brewer, E.D.; Hawkins, E.P.; Warren, R.W. Increasing incidence of childhood class V lupus nephritis. J. Rheumatol. 1998, 25, 1413–1418. [Google Scholar]
- ANA Complete Profile. Available online: https://muhealth.testcatalog.org/show/ANA-Comp) (accessed on 5 March 2022).
- Pierangeli, S.S.; de Groot, P.G.; Dlott, J.; Favaloro, E.; Harris, E.N.; Lakos, G.; Ortel, T.; Meroni, P.L.; Otomo, K.; Pengo, V.; et al. ‘Criteria’aPL tests: Report of a task force and preconference workshop at the 13th International Congress on Antiphospholipid Antibodies, Galveston, Texas, April 2010. Lupus 2011, 20, 182–190. [Google Scholar] [CrossRef]
- Petri, M.; Kim, M.Y.; Kalunian, K.C.; Grossman, J.; Hahn, B.H.; Sammaritano, L.R.; Lockshin, M.; Merrill, J.T.; Belmont, H.M.; Askanase, A.D.; et al. Combined oral contraceptives in women with systemic lupus erythematosus. N. Engl. J. Med. 2005, 353, 2550–2558. [Google Scholar] [CrossRef]
- Gladman, D.; Ginzler, E.; Goldsmith, C.; Fortin, P.; Liang, M.; Urowitz, M.; Bacon, P.; Bombardieri, S.; Hanly, J.; Hay, E.; et al. Systemic lupus international collaborative clinics: Development of a damage index in systemic lupus erythematosus. J. Rheumatol. 1992, 19, 1820–1821. [Google Scholar] [PubMed]
- Mina, R.; von Scheven, E.; Ardoin, S.P.; Eberhard, B.A.; Punaro, M.; Ilowite, N.; Hsu, J.; Klein-Gitelman, M.; Moorthy, L.N.; Muscal, E.; et al. Consensus treatment plans for induction therapy of newly diagnosed proliferative lupus nephritis in juvenile systemic lupus erythematosus. Arthritis Care Res. 2012, 64, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Wu, T.; Xie, C.; Vanarsa, K.; Han, J.; Mahajan, T.; Oei, H.B.; Ahn, C.; Zhou, X.J.; Putterman, C.; et al. Urine VCAM-1 as a marker of renal pathology activity index in lupus nephritis. Arthritis Res. Ther. 2012, 14, R164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michel, M.; Johanet, C.; Meyer, O.; Frances, C.; Wittke, F.; Michel, C.; Arfi, S.; Tournier-Lasserve, E.; Piette, J.C. Familial lupus erythematosus. Clinical and immunologic features of 125 multiplex families. Medicine 2001, 80, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Lau, C.S.; Chan, T.M.; Wong, R.W. Clinical characteristics and outcome of southern Chinese males with systemic lupus erythematosus. Lupus 1999, 8, 188–196. [Google Scholar] [CrossRef]
- Tan, T.C.; Fang, H.; Magder, L.S.; Petri, M.A. Differences between Male and Female Systemic Lupus Erythematosus in a Multiethnic Population. J. Rheumatol. 2012, 39, 759–769. [Google Scholar] [CrossRef]
- Soto, M.E.; Vallejo, M.; Guillen, F.; Simon, J.A.; Arena, E.; Reyes, P.A. Gender impact in systemic lupus erythematosus. Clin. Exp. Rheumatol. 2004, 22, 713–721. [Google Scholar]
- Parodis, I.; Arnaud, L.; Gerhardsson, J.; Zickert, A.; Sundelin, B.; Malmstrom, V.; Svenungsson, E.; Gunnarsson, I. Antiphospholipid Antibodies in Lupus Nephritis. PLoS ONE 2016, 11, e0158076. [Google Scholar] [CrossRef] [Green Version]
- Loizou, S.; Samarkos, M.; Norsworthy, P.J.; Cazabon, J.K.; Walport, M.J.; Davies, K.A. Significance of anticardiolipin and anti-beta(2)-glycoprotein I antibodies in lupus nephritis. Rheumatology 2000, 39, 962–968. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.A.; Marcos, J.C.; Marcos, A.I.; Pons-Estel, B.A.; Wojdyla, D.; Arturi, A.; Babini, J.C.; Catoggio, L.J.; Alarcon-Segovia, D. Male systemic lupus erythematosus in a Latin-American inception cohort of 1214 patients. Lupus 2005, 14, 938–946. [Google Scholar] [CrossRef]
- Andrade, R.M.; Alarcon, G.S.; Fernandez, M.; Apte, M.; Vila, L.M.; Reveille, J.D. Accelerated damage accrual among men with systemic lupus erythematosus: XLIV. Results from a multiethnic US cohort. Arthritis Rheum. 2007, 56, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.F.; Drenkard, C.; Molina, J.; Cardiel, M.H.; Uribe, O.; Anaya, J.M.; Gomez, L.J.; Felipe, O.; Ramirez, L.A.; Alarcon-Segovia, D. Systemic lupus erythematosus in males. A study of 107 Latin American patients. Medicine 1996, 75, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Contreras, G.; Lenz, O.; Pardo, V.; Borja, E.; Cely, C.; Iqbal, K.; Nahar, N.; de La Cuesta, C.; Hurtado, A.; Fornoni, A.; et al. Outcomes in African Americans and Hispanics with lupus nephritis. Kidney Int. 2006, 69, 1846–1851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prete, P.E.; Majlessi, A.; Gilman, S.; Hamideh, F. Systemic lupus erythematosus in men: A retrospective analysis in a Veterans Administration Healthcare System population. J. Clin. Rheumatol. 2001, 7, 142–150. [Google Scholar] [CrossRef]
- Wang, Y.F.; Xu, Y.X.; Tan, Y.; Yu, F.; Zhao, M.H. Clinicopathological characteristics and outcomes of male lupus nephritis in China. Lupus 2012, 21, 1472–1481. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALL cSLE | Males (n = 95) | Females (n = 545) | ||
|---|---|---|---|---|
| Age at SLE diagnosis, median, (IQR *) | 14 | (11–15) | 14 | (11–16) |
| Ethnicity, n (%) | ||||
| Hispanic | 44 | (46) | 212 | (39) |
| Non-Hispanic White | 15 | (16) | 84 | (15) |
| Asian | 10 | (11) | 48 | (9) |
| Black | 22 | (23) | 179 | (33) |
| Mixed | 1 | (1) | 16 | (3) |
| Unknown | 3 | (3) | 6 | (1) |
| Family history of autoimmune disease | 44 | (46) | 215 | (39) |
| Family history of SLE, n (%) | 27 | (28) | 105 | (19) |
| cSLE with LN Ever | Males (n = 59) | Females (n = 314) | ||
| Age at SLE diagnosis, median, (IQR *) | 13 | (11–14) | 14 | (11–15) |
| Ethnicity, n (%) | ||||
| Hispanic | 26 | (44) | 121 | (39) |
| Non-Hispanic White | 12 | (20) | 47 | (15) |
| Asian | 5 | (8) | 24 | (8) |
| Black | 14 | (24) | 107 | (34) |
| Mixed | 0 | (0) | 11 | (4) |
| Unknown | 2 | (3) | 4 | (1) |
| Family history of autoimmune disease | 27 | (46) | 108 | (34) |
| Family history of SLE, n (%) | 17 | (29) | 50 | (16) |
| Non-renal cSLE | Males (n = 36) | Females (n = 231) | ||
| Age at SLE diagnosis, median, (IQR *) | 13 | (11–16) | 13 | (10–14) |
| Ethnicity, n (%) | ||||
| Hispanic | 18 | (50) | 91 | (39) |
| Non-Hispanic White | 3 | (8) | 37 | (16) |
| Asian | 5 | (14) | 24 | (10) |
| Black | 8 | (22) | 72 | (31) |
| Mixed | 1 | (3) | 5 | (2) |
| Unknown | 1 | (3) | 2 | (1) |
| Family history of autoimmune disease | 17 | (47) | 107 | (46) |
| Family history of SLE, n (%) | 10 | (28) | 55 | (24) |
| Feature | Males, n (%) | Females, n (%) |
|---|---|---|
| WHO Class | ||
| Class I | 1 (2) | 11 (4) |
| Class II | 11 (19) | 27 (9) |
| Class III | 14 (24) | 60 (19) |
| Class IV | 10 (17) | 75 (24) |
| Class V | 9 (15) | 54 (17) |
| Mixed class III + V | 6 (10) | 22 (7) |
| Mixed class IV + V | 6 (10) | 26 (8) |
| Class VI | 0 (0) | 1 (0.3) |
| Not biopsied/unknown | 2 (3) | 38 (12) |
| Feature | Males, n (%) |
|---|---|
| Histopathology | |
| Mesangial hypercellularity | 53 (90) |
| Cellular crescents | 8 (14) |
| Endocapillary proliferation | 12 (24) |
| Membranous lesions | 28 (48) |
| Clinical manifestation * | |
| Elevated serum creatinine (n = 37) | 9 (24) |
| Nephritis (n = 37) | 30 (81) |
| Nephrotic syndrome (n = 35) | 15 (35) |
| Hypertension (n = 36) | 17 (47) |
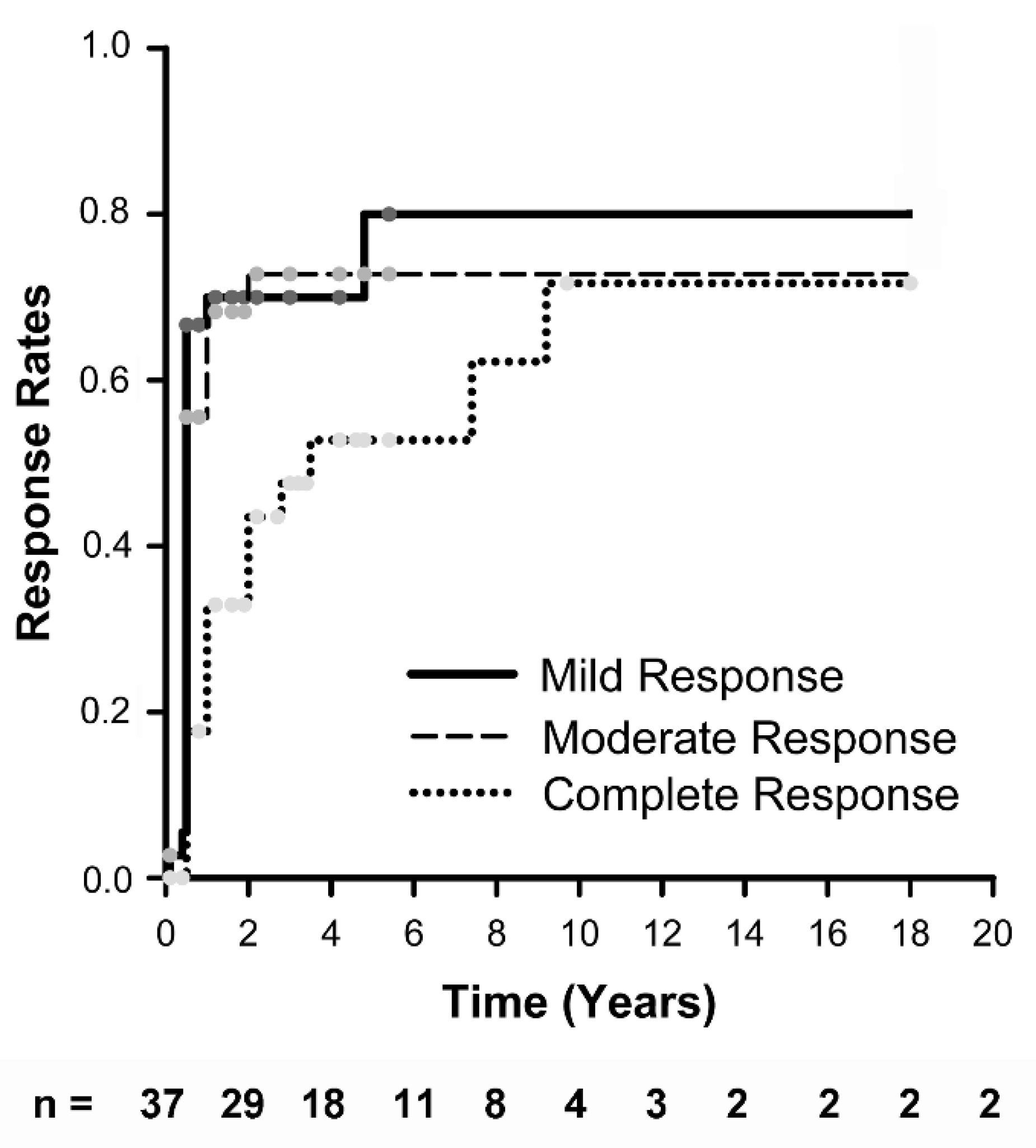
| Onset (n = 37) | 6 mos (n = 36) | 12 mos (n = 33) | 24 mos (n = 34) | Latest F/U * (n = 37) | |
|---|---|---|---|---|---|
| Responders (%) § | 0% | 66% | 63% | 61% | 49% |
| Complete response | 0 | 17% | 33% | 35% | 38% |
| Moderate response | 0 | 35% | 27% | 18% | 19% |
| Mild response | 0 | 14% | 3% | 0% | 3% |
| Renal Flares (%) § | 0% | 0% | 9% | 21% | 22% |
| Proteinuric (n) | 0 | 0 | 2 | 3 | 3 |
| Nephritic (n) | 0 | 0 | 1 | 4 | 5 |
| Median GFR (IQR) §§ | 122 (103–135) | 118 (102–139) | 122 (106–147) | 124 (94–135) | 125 (90–140) |
| Immunomodulatory drugs ¥, median number (range) | 1 (0–2) | 3 (2–4) | 4 (3–5) | 4 (3–6) | 4 (1–7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wenderfer, S.E.; Orjuela, A.; Bekheirnia, M.R.; Pereira, M.; Muscal, E.; Braun, M.C.; De Guzman, M. Lupus Nephritis, Autoantibody Production and Kidney Outcomes in Males with Childhood-Onset Systemic Lupus Erythematosus. Pediatr. Rep. 2022, 14, 220-232. https://doi.org/10.3390/pediatric14020030
Wenderfer SE, Orjuela A, Bekheirnia MR, Pereira M, Muscal E, Braun MC, De Guzman M. Lupus Nephritis, Autoantibody Production and Kidney Outcomes in Males with Childhood-Onset Systemic Lupus Erythematosus. Pediatric Reports. 2022; 14(2):220-232. https://doi.org/10.3390/pediatric14020030
Chicago/Turabian StyleWenderfer, Scott E., Alvaro Orjuela, Mir Reza Bekheirnia, Maria Pereira, Eyal Muscal, Michael C. Braun, and Marietta De Guzman. 2022. "Lupus Nephritis, Autoantibody Production and Kidney Outcomes in Males with Childhood-Onset Systemic Lupus Erythematosus" Pediatric Reports 14, no. 2: 220-232. https://doi.org/10.3390/pediatric14020030
APA StyleWenderfer, S. E., Orjuela, A., Bekheirnia, M. R., Pereira, M., Muscal, E., Braun, M. C., & De Guzman, M. (2022). Lupus Nephritis, Autoantibody Production and Kidney Outcomes in Males with Childhood-Onset Systemic Lupus Erythematosus. Pediatric Reports, 14(2), 220-232. https://doi.org/10.3390/pediatric14020030