
An Overview of Guidelines for Supplemental Feeding of Infants in Swedish Maternity Clinics




Abstract
:1. Introduction
2. Material and Methods
2.1. Collection of Data
2.2. Data Analysis
3. Results
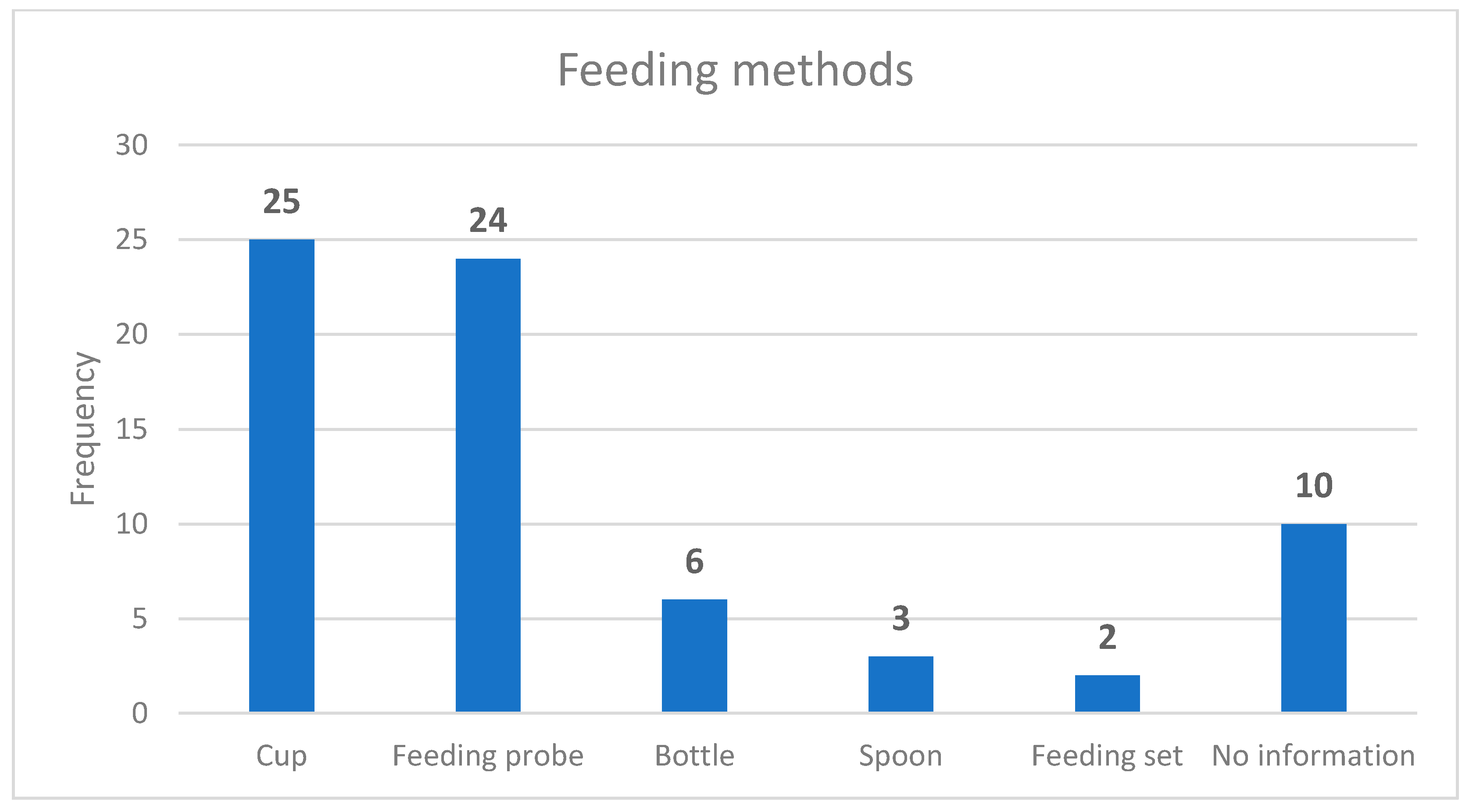
3.1. Feeding Methods and Risk Factors
3.2. Breastfeeding Support
3.3. Discontinuation of Supplemental Feeding
4. Discussion
Methodological Considerations
5. Conclusions and Suggestions for Future Direction
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Baby-Friendly Hospital Initiative. Revised, Updated and Expanded for Integrated Care. 2009. Available online: https://apps.who.int/iris/bitstream/handle/10665/43593/9789241594967_eng.pdf (accessed on 11 December 2020).
- Wackernagel, D.; Bonamy, A.-K.E.; Gustafsson, A.; Reims, A.; Pupp, I.H.; Ahlsson, F.; Elfving, M.; Domellöf, M. Vårdprogram—Neonatal Hypoglykemi Hos Nyfödda Med Gestationsålder ≥ 35 Veckor [The National Care Program—Neonatal Hypoglycaemia in New-Borns with Gestational Age ≥ 35 Weeks]. 2017. Available online: https://neo.barnlakarforeningen.se/wp-content/uploads/sites/14/2017/12/Nationellt_postnatal_hypoglykemi_v%C3%A5rdprogram_final.pdf (accessed on 11 December 2020).
- Socialstyrelsen. Statistics on Breastfeeding. 2017. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2019-9-6379.pdf (accessed on 11 December 2020).
- Karimi, F.Z.; Sadeghi, R.; Maleki-Saghooni, N.; Khadivzadeh, T. The effect of mother-infant skin to skin contact on success and duration of first breastfeeding: A systematic review and meta-analysis. Taiwan J. Obs. Gynecol. 2019, 58, 1–9. [Google Scholar] [CrossRef]
- Svensson, K.; Velandia, M.; Matthiesen, A.-S.; Welles-Nyström, B.; Widström, A.-M. Effects of mother-infant skin-to-skin contact on severe latch-on problems in older infants: A randomized trial. Int. Breastfeed J. 2013, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Widström, A.-M.; Brimdyr, K.; Svensson, K.; Cadwell, K.; Nissen, E. A plausible pathway of imprinted behaviors: Skin-to-skin actions of the newborn immediately after birth follow the order of fetal development and intrauterine training of movements. Med. Hypotheses 2020, 134, 109432. [Google Scholar] [CrossRef]
- Svensson, K.; Zwedberg, S. Reproduktiv Hälsa: Barnmorskans Kompetensområde [Reproductive health: The midwife’s area of expertise]; Studentlitteratur: Lund, Sweden, 2016; pp. 653–655. [Google Scholar]
- Ransjö-Arvidsson, A.B.; Sjödin, M.; Widström, A.M. Föräldra-barn-interaktion, amning och stöd efter födelsen. [Parent-child interaction, breastfeeding and postpartum support]. In Obstetrik; Hagberg, H., Marsál, K., Westgren, M., Eds.; Studentlitteratur: Lund, Sweden, 2014; pp. 577–587. [Google Scholar]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G.; Group, T.L.B.S. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Wackernagel, D.; Gustafsson, A.; Edstedt Bonamy, A.K.; Reims, A.; Ahlsson, F.; Elfving, M.; Domellöf, M.; Hansen Pupp, I. Swedish national guideline for prevention and treatment of neonatal hypoglycaemia in newborn infants with gestational age ≥ 35 weeks. Acta Paediatr. 2020, 109, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Mosca, F.; Giannì, M.L. Human milk: Composition and health benefits. Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [Green Version]
- Hansstein, F.V.J.A.J.o.H.P. The impact of breastfeeding on early childhood obesity: Evidence from the National Survey of Children’s Health. Am. J. Health Promot. 2016, 30, 250–258. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N. Rollins, Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Horta, B.L.; Loret De Mola, C.; Victora, C.G. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 14–19. [Google Scholar] [CrossRef]
- Strøm, M.; Mortensen, E.L.; Kesmodel, U.S.; Halldorsson, T.; Olsen, J.; Olsen, S.F. Is breast feeding associated with offspring IQ at age 5? Findings from prospective cohort: Lifestyle during pregnancy study. BMJ Open 2019, 9, e023134. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 96–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eidelman, A.; Schanler, R. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Bromiker, R.; Perry, A.; Kasirer, Y.; Einav, S.; Klinger, G.; Levy-Khademi, F. Early neonatal hypoglycemia: Incidence of and risk factors. A cohort study using universal point of care screening. J. Matern. Fetal Neonatal Med. 2019, 32, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Naif, M.H.; Hanoudi, B.M.; Ayoub, N.I. Evaluation of maternal and neonatal risk factors for neonatal hypoglycemia. IRAQI J. Comm. Med. 2013, 26, 13–18. [Google Scholar]
- Dalsgaard, B.T.; Rodrigo-Domingo, M.; Kronborg, H.; Haslund, H. Breastfeeding and skin-to-skin contact as non-pharmacological prevention of neonatal hypoglycemia in infants born to women with gestational diabetes; a Danish quasi-experimental study. Sex. Reprod. Health. 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Stomnaroska-Damcevski, O.; Petkovska, E.; Jancevska, S.; Danilovski, D. Neonatal hypoglycemia: A continuing debate in definition and management. Prilozi 2015, 36, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.; Harris, D.; Hegarty, J.; Alsweiler, J.; McKinlay, C. An emerging evidence base for the management of neonatal hypoglycaemia. Early Hum. Dev. 2017, 104, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Yu, J.; Wu, Y.; Zhang, H. Hypoglycemia incidence and risk factors assessment in hospitalized neonates. J. Matern. Fetal Neonatal Med. 2015, 28, 422–425. [Google Scholar] [CrossRef]
- Olsson, E.; Diderholm, B.; Blomqvist, Y.T. “Paying it Forward”—Swedish Women’s Experiences of Donating Human Milk. J. Hum. Lact. 2020, 35, 220–222. [Google Scholar] [CrossRef]
- Flint, A.; New, K.; Davies, M.W. Cup feeding versus other forms of supplemental enteral feeding for newborn infants unable to fully breastfeed. Cochrane Database Syst. Rev. 2016, 2016, Cd005092. [Google Scholar] [CrossRef]
- Mazo-Tomé, P.; Suárez-Rodríguez, M. Prevalence of exclusive breastfeeding in the healthy newborn. Boletín Med. Hosp. Infant. México 2018, 75, 49–56. [Google Scholar] [CrossRef]
- De Montigny, F.; Gervais, C.; Larivière-Bastien, D.; St-Arneault, K. The role of fathers during breastfeeding. Midwifery 2018, 58, 6–12. [Google Scholar] [CrossRef] [PubMed]
- McCoy, M.B.; Heggie, P.J.P. In-hospital formula feeding and breastfeeding duration. Pediatrics 2020, 146, e20192946. [Google Scholar] [CrossRef]
- Kellams, A.; Harrel, C.; Omage, S.; Gregory, C.; Rosen-Carole, C. Academy of Breastfeeding Medicine clinical protocol# 3: Supplementary feedings in the healthy term breastfed neonate, revised 2017. Breastfeed. Med. 2017, 12, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Socialstyrelsen. SOSFS 2008:33 Information Som Avser Uppfödning Genom Amning Eller Med Modersmjölksersättning. [Information Relating to Breeding through Breastfeeding or with Infant Formula]. 2008. Available online: https://www.socialstyrelsen.se/regler-och-riktlinjer/foreskrifter-och-allmanna-rad/konsoliderade-foreskrifter/200833-om-information-som-avser-uppfodning-genom-amning-eller-med-modersmjolksersattning/ (accessed on 11 December 2020).
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ (Clin. Res. Ed.) 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. J. Postgrad. Med. 2002, 48, 206–208. [Google Scholar]
- Chantry, C.; Dewey, K.; Peerson, J.; Wagner, E.; Nommsen-Rivers, L. In-hospital formula use increases early breastfeeding cessation among first-time mothers intending to exclusively breastfeed. J. Pediatr. 2014, 164, 1339–1345.e5. [Google Scholar] [CrossRef] [Green Version]
- Gu, M.-H.; Amanda, F.; Yuan, T.-M. Brain Injury in Neonatal Hypoglycemia: A Hospital-Based Cohort Study. Clinical Medicine Insights. Pediatrics 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Tozier, P.K. Colostrum versus formula supplementation for glucose stabilization in newborns of diabetic mothers. J. Obs. Gynecol. Neonatal Nurs. 2013, 42, 619–628. [Google Scholar] [CrossRef]
- Boban, M.; Zakarija-Grković, I. In-hospital formula supplementation of healthy newborns: Practices, reasons, and their medical justification. Breastfeed. Med. 2016, 11, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Hermanson, Å.; Åstrand, L.L. The effects of early pacifier use on breastfeeding: A randomised controlled trial. Women Birth 2020, 33, e473–e482. [Google Scholar] [CrossRef] [PubMed]
- Häggkvist, A.P.; Brantsæter, A.L.; Grjibovski, A.M.; Helsing, E.; Meltzer, H.M.; Haugen, M. Prevalence of breast-feeding in the Norwegian Mother and Child Cohort Study and health service-related correlates of cessation of full breast-feeding. Public Health Nutr. 2010, 13, 2076–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batista, C.; Rodrigues, V.; Ribeiro, V.; Nascimento, M. Nutritive and non-nutritive sucking patterns associated with pacifier use and bottle-feeding in full-term infants. Early Hum. Dev. 2019, 132, 18–23. [Google Scholar] [CrossRef]
- Bäckström, C.; Thorstensson, S.; Mårtensson, L.B.; Grimming, R.; Nyblin, Y.; Golsäter, M. ‘To be able to support her, I must feel calm and safe’: Pregnant women’s partners perceptions of professional support during pregnancy. BMC Pregnancy Childbirth 2017, 17, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widarsson, M.; Engström, G.; Tyden, T.; Lundberg, P.; Hammar, L.M. “Paddling upstream”: Fathers’ involvement during pregnancy as described by expectant fathers and mothers. J. Clin. Nurs. 2014, 24, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Abbass-Dick, J.; Dennis, C.-L. Maternal and paternal experiences and satisfaction with a co-parenting breastfeeding support intervention in Canada. Midwifery 2018, 56, 135–141. [Google Scholar] [CrossRef]
- Parry, J.E.; Ip, D.K.; Chau, P.Y.; Wu, K.M.; Tarrant, M. Predictors and consequences of in-hospital formula supplementation for healthy breastfeeding newborns. J. Hum. Lact. 2013, 29, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Zwedberg, S.; von Hofsten, M.; Jurell, O. Formula feeding after emergency cesarean section–a descriptive retrospective cohort study. J. Pregnancy Child Health 2015, 2, 2. [Google Scholar]
- Zhao, Y.; Lin, Q.; Wang, J.; Bao, J. Effects of prenatal individualized mixed management on breastfeeding and maternal health at three days postpartum: A randomized controlled trial. J. Early Hum. Dev. 2020, 141, 104944. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category |
|---|
| Author |
| Year developed |
| Stated year for next revision |
| References |
| Number of pages |
| Feeding methods |
| Risk factors |
| Breastfeeding support |
| Discontinuation of supplemental feeding |
| Guidelines n = 38 | |||
|---|---|---|---|
| Component | Included | Omitted | Extra Information |
| Author n (%) | 31 (82) | 7 (18) | 25 physicians 22 midwifes |
| Year developed n (%) | 34 (89) | 4 (11) | 2013–2019 |
| Stated year for next revision n (%) | 8 (24) | 30 (76) | The validity period varied between 2019–2022 |
| References n (%) | 19 (50) | 19 (50) | 18 international, 1 national |
| Number of pages, mean (min–max) | 19 (1–45) | ||
| Grade of Evidence /Level of Recommendation |
|---|
| High: Randomised studies. Further research is unlikely to change our confidence in the estimate of effect. |
| Moderate: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. |
| Low: Observational studies. Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. |
| Very low: Any estimate of effect is very uncertain. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerstis, B.; Richardsson, A.; Stenström, A.; Widarsson, M. An Overview of Guidelines for Supplemental Feeding of Infants in Swedish Maternity Clinics. Nurs. Rep. 2021, 11, 95-104. https://doi.org/10.3390/nursrep11010010
Kerstis B, Richardsson A, Stenström A, Widarsson M. An Overview of Guidelines for Supplemental Feeding of Infants in Swedish Maternity Clinics. Nursing Reports. 2021; 11(1):95-104. https://doi.org/10.3390/nursrep11010010
Chicago/Turabian StyleKerstis, Birgitta, Anna Richardsson, Alexandra Stenström, and Margareta Widarsson. 2021. "An Overview of Guidelines for Supplemental Feeding of Infants in Swedish Maternity Clinics" Nursing Reports 11, no. 1: 95-104. https://doi.org/10.3390/nursrep11010010
APA StyleKerstis, B., Richardsson, A., Stenström, A., & Widarsson, M. (2021). An Overview of Guidelines for Supplemental Feeding of Infants in Swedish Maternity Clinics. Nursing Reports, 11(1), 95-104. https://doi.org/10.3390/nursrep11010010